
Mortality from COVID-19 in the US: Did unions save lives?
Abstract
This paper builds on the existing literature on the effect of unionization on OSH by providing an analysis of unionization’s effects on COVID-19 mortality. It combines data from the NVSS with the CPS into a unique dataset. It finds that a 10 percentage-point increase in unionization is associated with a reduction in mortality from 26 per 100,000 workers to 24 per 100,000 workers. This means that if the United States had the union density of 35 percent that it had in 1954 instead of today’s rate of 10 percent, the COVID-19 mortality rate for working people would have fallen from 26 to 19 per 100,000.
Introduction
When compared with other industrialized countries, and indeed, most countries in the world, the United States fared poorly in the face of COVID-19. Estimates of excess mortality during the COVID-19 pandemic rank the United States as having the fourth highest rate, at 179 deaths per 100,000
However, another institutional failing that has received relatively less attention is the lack of or limited protections provided to American workers at the workplace. Protections against dismissal, comprehensive coverage of occupational safety and health (OSH), and access to paid sick leave and employer-provided health insurance are working conditions that are not only important for overall job quality, but which had potential consequences for forestalling the spread of the COVID-19 pandemic. However, these protections are not covered by most legal statutes governing employment in the United States, or if covered, coverage is incomplete, as in the case of OSH.
But workers whose employment contracts are governed by collective bargaining agreements – those that belong to a union or work in a unionized workplace – are more likely to have such protections. In the 1950s, one in three American workers was unionized and benefited from the strengthened labour protections of their collective bargaining contract. By 2022, the percentage of American workers that was unionized had fallen to one in ten (or 10.1 percent, with collective bargaining coverage slightly higher at 12.1 percent)1. Unionization is especially low in the private sector, at just 6 percent, compared with 33 percent in the public sector (BLS, 2023).
The low rate of unionization is surprising given that 54 percent of American workers surveyed in 2017 stated that they would choose union representation if given an option, much higher than the one-third recorded in similar surveys undertaken in 1977 and 1995 (Kochan et al., 2019). Survey respondents also confirmed that there were important gaps in their ability to voice opinions or concerns in a wide range of workplace issues ranging from benefits and schedules, to how to organize their work most effectively. In particular, 45 percent of workers indicated that they would like to have more say than they had in their ability to perform their job safely.
This study tests whether unionization, and by implication the greater protections and voice that it can bestow, helped to mitigate COVID-19 mortality in 2020. It uses a novel approach that combines data on COVID-19 mortality and unionization during 2020 (the only year for which this data are available) to estimate whether unionization had a mitigating effect. It finds that a 10 percentage point increase in unionization would reduce workers’ likelihood of dying from COVID-19 from 26 per 100,000 to 24 per 100,000. The next section provides explanation on the mechanisms by which unionization could have such an impact, as well as providing some examples of steps taken by unions during the pandemic to protect the workforce.
Occupational safety and health, unions and the COVID-19 pandemic
The United States is an outlier when it comes to labour and social protection. There is no federal regulation mandating paid sick leave, paid maternity leave, or paid annual leave.2 Health care coverage is also not universal, and as a result, 11 percent of employed persons were uninsured in 2021 (Keisler-Starkey and Bunch, 2022). Protection from dismissal is also lacking; private-sector, non-unionized employees are hired under “employment-at-will”, which permits dismissal without grounds, with limited exceptions.3 The lack of employment protection, in turn, has implications for compliance with the limited but existing labour rights, as workers may be reluctant to raise objections regarding non-compliance or even concerns, such as about health and safety risks, out of fear of dismissal.
US laws on occupational safety and health and the overall OSH systems in the United States are also weak and outmoded, particularly when compared with other countries and international guidance (Cooney et al., 2023). The main federal statute governing OSH in the U.S. is the Occupational Safety and Health Act of 1970 (OSHAct).4 The OSHAct limits obligations and rights to the employer-employee relationship, which means that rather than protecting all persons who work in a given workplace as is the case, for example, in Australia’s Work Health and Safety Act 2011, protections are limited to “employees”, and thus excludes workers classified as independent contractors, interns, or volunteers. The OSHAct applies to private-sector workers, though the US federal government has extended protection to federal public sector workers by presidential Executive Order. This means, however, that at the state and county level, public sector workers are excluded from protection unless specific legal regulations have been passed, or if the public sector workers are covered by a collective bargaining agreement that includes OSH provisions. In West Virginia, for example, the OSH law for public sector workers only covers employees of the state (not county and municipal workers) and specifically excludes “the department of corrections, the department of health and the Legislature,” which meant that many high-risk essential workers -- unless they were covered by a collective bargaining agreement -- were not covered by OSH regulations during the COVID-10 pandemic (Spieler, 2023).
In addition to gaps in the coverage of OSH laws, enforcement is also weak. In 2020, the number of OSHA inspectors was at its lowest level since the agency was established fifty years ago. Overall, there were 774 federal and 1024 state inspectors to inspect 10.1 million workplaces, or one inspector for every 82,881 workers (Spieler, 2023). This is far below the ILO recommendation for industrialized countries of one inspector per 10,000 workers (ILO, 2006).
Labour inspection is an important means for enforcing compliance with existing regulation, but it is not the only means; collective representation at the workplace also improves compliance. Unionization and the collectively negotiated agreements that regulate unionized workplaces, routinely include provisions on OSH, and in some instances include the establishment of bipartite safety and health committees that work to abate safety and health hazards. Unions can also play a role in educating workers on the prevention of hazards, and workers may feel more comfortable addressing safety (or other) concerns to their representatives as opposed to management. In turn, unions representatives can more easily engage with management to address concerns.
Indeed, studies on the effects of unionization on safety and health in the United States find that unionized establishments are more likely to receive safety and health inspections, face greater scrutiny in the course of those inspections, and pay higher penalties for violating health and safety standards than comparable non-union establishments (
Unions can also improve occupational safety and health through other benefits that are often included in collective bargaining agreements. As mentioned, paid sick leave is not guaranteed by federal labour law.5 As a result, coverage of paid sick leave is highly uneven, and often lacking amongst lower earners. In 2010, only one-third of workers in the bottom quartile of the wage distribution had access to paid sick leave, compared with 81 percent of workers in the top. Because small business and part-time workers are often excluded from employer-provided benefits, just 27 percent of food preparation, food service and childcare workers had paid sick leave (US Joint Economic Committee, 2010). Unionization, however, is effective for extending coverage. In 2019, 91 percent of unionized workers had paid sick leave coverage compared with 73 percent of non-unionized workers. Workers who feel that they can stay at home when they are ill without losing their job or losing wages are more likely to call in sick when they are ill, potentially mitigating the spread of contagious diseases, such as COVID-19.
During the COVID-19 pandemic, unions were active in strengthening OSH protocols at the workplace level, in addition to lobbying and taking legal action at the local, state and national levels.6 At the workplace level, a review of collective agreements negotiated during the pandemic revealed agreements to institute stricter safety and health protocols such as physical distancing, restrictions on the number of customers at a given worksite, 7 as well as the provision of personal protective equipment (PPE) (Fischer-Daly and Brown, 2021). Some agreements included the creation of union-management councils to monitor and mitigate the spread of the virus at work.8 In addition, there were memoranda of understanding (MOUs) and side agreements, especially in health care and education, that addressed suspending operations in case of an outbreak at work, as well as programs for regular screening, testing, and contract tracing for COVID-19.9 Other agreements expanded access to or eased the use of paid leave, allowing employees to take time off in case they, or a household member contracted the virus (Fischer-Daly and Brown, 2021).10
The role of unions leading to higher standards of compliance with OSH during the COVID-19 pandemic seems to have resulted in tangible improvements in health outcomes, based on the few studies that have been carried out testing this relationship. Perhaps the most well-known are two studies comparing health outcomes at unionized and non-unionized nursing homes (Dean et al., 2020, 2022). Nursing homes were epicenters of both outbreaks and mortality during the COVID-19 pandemic. The first study, covering 300 nursing homes in New York State, finds that when compared with non-unionized nursing homes, residents in unionized nursing homes had a 30 percent lower COVID-19 mortality rate, or a 1.29 percentage point reduction in mortality. Unions were associated with greater access to PPE, one mechanism that could explain the better outcomes. A follow-up study of nursing homes across the continental United States found that unions were associated with 10.8 percent lower COVID-19 mortality rates among nursing home residents, as well 6.8 percent lower COVID-19 infection rates among staff
Another study analysing the role of unions in mitigating infection from COVID-19 is
Articles analysing the implication of unionization on mortality more generally include Zoorob (2018) and
This paper builds on these studies to analyse the impact of unionization on COVID-19 mortality for the United States. Like Zoorob (2018), the analysis uses legislative instruments to correct for possibility endogeneity arising from unionization, but unlike Zoorob (2018), it estimates the effects of unions on mortality using individuals and not states as the unit of analysis. It also focuses on 2020 and solely on mortality from COVID-19.
Data and Methodology
The principal challenge in studying the relationship between unions and mortality is that there is no database with information on both the living and the dead. The National Vital Statistics System (NVSS), maintained by the Center for Disease Control, publishes a registry of all births and deaths during a given year. Information on union membership, on the other hand, is provided by the Census Bureau through the Current Population Survey (CPS). The CPS is a household survey with a rotating panel. Union membership is asked of all outgoing employed individuals.
Because of the need to respect the anonymity of respondents, neither the CPS nor the NVSS provide respondents’ names or social security numbers. As a result, it is not possible to directly link data on union membership and mortality. There are, however, numerous variables that can be found in both databases: such as age, sex, and race (education level is also in both databases, but it is encoded differently in each). Simply piling the CPS and NVSS data one on top of the other allows for the calculus of mortality data for any variable that is in both databases. By appending the two databases, we have a new microdata set of the living (from CPS) and the dead from (NVSS). Since the NVSS is a complete registry of all deaths, each observation has weight 1. Since the CPS is a sample survey, each observation carries with it the survey sampling weight provided in the microdata. With this piled database, any analysis involving variables that are in both databases can be undertaken, whether univariate of multivariate.
NVSS data use the International Classification of Diseases 10th Revision (ICD-10) code to classify cause of death. COVID-19 deaths are defined as those deaths whose ICD-10 is U071, B342 or U049. This gives 353,494 deaths from COVID-19 for the year 2020, which is a little higher than the official CDC published tally of 350,831 (Murphy et al., 2021). Since the lethality of COVID-19 is highly age-dependent, there are “only” 57,151 deaths among the 18 to 62 population. Once those not in the workforce are also excluded, COVID-19 deaths in 2020 drop to 44,564 and once those whose industry and occupation code do not match with CPS codes are excluded, the total falls to 38,325. The total living population with jobs and occupation codes that match those in the NVSS is 143 million people. This is about one million short of the average employed population from April to December 2020, which was about 144 million according to the full-sample CPS. The average COVID-19 mortality rate among these 143 million workers is about 26 per 100,000, which is much less than the total mortality rate of 91 per 100,000 calculated by the CDC for 2020 (Ahmad et al., 2020), but this is to be expected since most of the mortality is among people aged more than 62, who are excluded from this study. It is this 26 per 100,000 universe of mortality that we attempt to explain as a function of union status and other covariates.
Union status, however, is not found in the NVSS data. The usual shared demographic variables – age, sex, race – do not have enough granularity to be used to bring information on union membership into the NVSS, but in 2020, unlike the preceding years, the NVSS microdata included industry and occupation of each decedent. The variables for occupation and industry are both provided at the four-digit level.
Once occupation codes corresponding to homemakers, retirees, students and other codes for which union variables are not relevant are dropped, there are 16,854 occupation-industry cells in the NVSS data. Cell size varies from 1 to 25,798, with an average of 30 observations and a median of 2. The largest cell (the one with 25,798 decedents) corresponds to laborers in the construction industry.
Since the CPS outgoing rotation group is but a subsample of the CPS, we piled the 2018, 2019 and 2020 CPS to increase observations under the assumption that union density is relatively stable. In this piled dataset, there are 402,457 observations on union membership (with an average unionization rate of 11.79%). Once these observations are aggregated into occupation-industry cells, there are 27,003 cells, with cell sizes varying between 1 and 5,676 (unweighted) observations. The mean is 13 and the median once again is 2.
The fact that there are more cells in the CPS data than in the NVSS data could mean that some younger workers are in cells that have no decedents and are thus not in the NVSS data. It could also mean that there are differences in how industry and occupation codes are encoded in each of the databases (while they are coded using the same system, those filling in the blanks do not necessarily receive the same training). In any case, there are 12,231 merged cells, which allows for considerable variation for estimation commands. The size of the cell will be used for sensitivity analysis.
Table 1 – Industry-Occupation Cell Sizes
|
Cell size |
Number of cells |
Percentage of cells |
|---|---|---|
|
1 |
3,306 |
27% |
|
2 |
1,763 |
14% |
|
3 |
1,069 |
9% |
|
4 |
759 |
6% |
|
5 |
635 |
5% |
|
6 |
448 |
4% |
|
7 |
334 |
3% |
|
8 |
280 |
2% |
|
9 |
242 |
2% |
|
10 |
240 |
2% |
|
More than 10 |
3,155 |
26% |
|
All |
12,231 |
100% |
Now that unionization and mortality have been combined into a single dataset, the next step is to address the endogeneity of the unionization variable. Unionization is considered endogenous as it affects workplace outcomes such as the level of wages or the degree of safety and health at the workplace, but at the same time these workplace attributes (wages, OSH standards, other working conditions) can be catalysts for unionization.
Attempts to address endogeneity, particularly in the context of the literature on unionization and earnings, have given rise to an extensive literature on how to arrive at non-endogenous estimates of the effects of union membership on various outcomes. Corrections for endogenous union membership range from the use of longitudinal data in which observing the same person in different states will supposedly correct for nonrandom union status
Given the limits of our data, the only choice from the above list of methods for dealing with endogenous union membership is instrumental variables and for this we must find a variable or set of variables whose correlation with mortality variable passes exclusively through the union variable. Luckily for the econometrician, much of labour law and labour regulation in the United States is at the state-level, and there is wide variation in how friendly states are to unions. Two variables we used as indicators of a pro-union stance are:
-
The existence of right-to-work laws, which are state laws that prohibit union-security measures, particularly the union shop, under which workers are required to join a union within a specified time after they begin employment. Right-to-work laws have been associated with decreasing union coverage by more than 10 percent
(Chun 2023) . The variable we used was simply an indicator variable that assumed the value 1 if there were right-to-work laws in 2020 in a given state and 0 if not. The data are from the National Conference of State Legislatures.11 -
Pre-emption. Many cities, counties, and other local governments instituted their own labour standards, such as on minimum wages, workplace scheduling or paid leave. In response, some state legislatures have passed pre-emption laws that invalidate these local statutes. The Economic Policy Institute (EPI) codifies such laws in its database.12 There are six different variables in the EPI database and we aggregated them using Multiple Correspondence Analysis into a single pro-labour index that varies form -2.03 when a state has all possible types of pre-emption laws on the books (Kansas, Tennessee and Michigan) to 1.17 when a state allows local government free reign in setting labour standards (Connecticut, Minnesota, Nebraska, New York, Vermont, and Washington).
For the main estimations, we merged the two state-level instruments described above with the CPS data using the FIPS (Federal Information Processing System) codes for region and state. We then ran a linear probability model in which the probability of belonging to a union was estimated using the two instruments as well as the variables to be used in the subsequent mortality estimation. The results are in Table 213.
Table 2 – Determinants of Unionization
|
Linear probability model |
||||
|
Union |
Coef. |
p-value |
Coef. |
p-value |
|
Right to work |
-0.083 |
0% |
0.083 |
0% |
|
Pre-emption |
0.002 |
1% |
0.02 |
1% |
|
Higher education |
0.009 |
0% |
||
|
Age |
0.006 |
0% |
||
|
Age2 |
0.000 |
0% |
0.000 |
0% |
|
Sex (male) |
-0.013 |
0% |
-0.013 |
0% |
|
Race (relative to white) |
||||
|
Black |
0.013 |
0% |
0.013 |
0% |
|
Native American |
-0.034 |
0% |
-0.035 |
0% |
|
Asian |
-0.004 |
3% |
-0.004 |
5% |
|
Other |
0.1600 |
0% |
0.012 |
0% |
|
R2 |
0.1600 |
0.1599 |
||
|
Number of Jobs |
402,457 |
402.457 |
||
|
Prob>chi2 |
0.00% |
0.00% |
||
Source: CPS microdata; Economic Policy Institute; National Conference of State Legislatures.
The predicted union probabilities were then aggregated into the occupation-industry cells and incorporated into the previously prepared NVSS-CPS database. Since the NVSS data do not disseminate state identifiers, this means that the two-stage least squares cannot be estimated using a single database. In principle, this is not an insurmountable obstacle. As shown by
One additional data problem is that education was not coded in the same way in the NVSS and CPS data. We thus used two approaches: the first was not to use it and the second was to code it into a binary variable indicating who has higher education and who does not. Our a priori preferred approach is not to use education14, but the results will be presented using both approaches.15
Results
Table 3 below shows the basic results. Being a man increases COVID-19 death rates relative to women, as being black or native American (relative to whites). Older workers were at greater risk than younger ones. These results correspond with well-known findings about COVID-19 mortality in the United States
Table 3 – Probit Determinants of COVID-19 Mortality (Union Density Instrumented Linear Model)
|
CDF percentile – no education |
CDF percentile – higher education |
||||||||||
|
5 |
10 |
50 |
90 |
95 |
5 |
10 |
50 |
90 |
95 |
||
|
Union density |
-0.228 |
-0.221 |
-0.189 |
-0.160 |
-0.151 |
-0.070 |
-0.059 |
-0.025 |
0.036 |
0.042 |
|
|
Higher education |
-0.106 |
-0.104 |
-0.096 |
-0.086 |
-0.085 |
||||||
|
Sex |
0.394 |
0.397 |
0.404 |
0.411 |
0.414 |
0.142 |
0.146 |
0.156 |
0.166 |
0.168 |
|
|
Age |
0.028 |
0.028 |
0.031 |
0.032 |
0.033 |
0.090 |
0.091 |
0.095 |
0.098 |
0.099 |
|
|
Age2 |
0.000 |
0.000 |
0.000 |
0.000 |
0.000 |
-0.001 |
-0.001 |
-0.001 |
-0.001 |
-0.001 |
|
|
Race |
|||||||||||
|
Black |
0.220 |
0.222 |
0.228 |
0.234 |
0.237 |
0.137 |
0.141 |
0.150 |
0.161 |
0.162 |
|
|
Native American |
0.215 |
0.222 |
0.241 |
0.261 |
0.265 |
0.307 |
0.317 |
0.347 |
0.372 |
0.381 |
|
|
Asian |
-0.053 |
-0.051 |
-0.041 |
-0.031 |
-0.028 |
0.318 |
0.325 |
0.342 |
0.364 |
0.372 |
|
|
Other |
-0.675 |
-0.670 |
-0.618 |
-0.568 |
-0.558 |
-0.368 |
-0.335 |
-0.248 |
-0.162 |
-0.122 |
|
Source: NVSS and CPS micro data.
Note: The output above is the result of a probit model in which the output variable is to have died from COVID-19 in the last nine months of 2020. The union density variable was instrumented using the linear probability model shown on Table 2. Occupation and industry controls, as well as month dummy variables, were also included in the estimation, but the output is too long to be shown here. The numbers shown are the percentiles of the distribution of bootstrapped results.
Union density also reduces mortality. The coefficients of the two estimations (with and without higher education), at -0.189 and -0.025, are both negative, but their magnitude varies, with the magnitude of the estimation with education being lower.
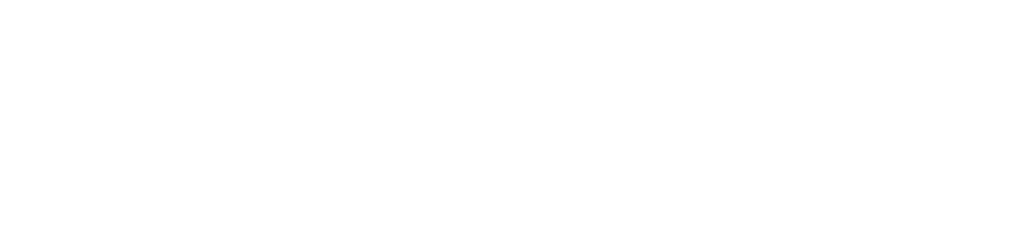
The two panels of Figure 1 show the cumulative distribution functions, estimated via bootstraps, of the union density coefficient for the estimates made with and without higher education. The standard error is larger for the estimation including higher education. This can be seen on Figure 1 as the slope of the cumulative distribution is steeper for the estimation that includes higher education. This also results in wider 90% and 95% confidence intervals, which means that when higher education is included, the coefficient is not significantly different from zero at 90% (the p-value is 74%).
Figure 1 – Distribution of the coefficient of the effect of Union density upon Covid-19 mortality
|
Panel 1 – No education variable |
Panel 2 – Higher education variable |
|
|
|


Source: NVSS and CPS micro data.
A value of -0.189 means that an increase in 10 percentage points in the unionization rate of an average worker’s industrial and occupation cell will reduce their likelihood of dying from COVID-19 from 26 per 100,000 to 24.2 per 100,000. If we apply this -0.189 reduction to shifting from a non-unionized to a unionized workplace – or in other words, a 100% increase in unionization – then the reduction in the likelihood of death from COVID-19 is much greater: from 26 per 100,000 to 12.6 per 100,000. In practice, it is the presence of a union in the workplace that makes the difference, even if some workers are not members, as there would still be a collective agreement regulating higher standards that would apply to all workers as well as union activities to ensure compliance at the workplace with the standards.
While these results are compelling, it is important to include sensitivity analysis to verify the findings. Since union data were matched using industry-occupation cells, a first possibility is to see how results vary according to the size of cell. The default is using any cell with at least a single observation. Table 4 shows how the results vary according to cell size. The answer is that the coefficients increase slightly with the elimination of smaller cells, but the result is not strong. This exercise is simply to show that the results still hold when controlling for different industry-occupation cell sizes; we still believe that -0.189 is the best estimate.
Table 4 – Union density coefficients, according to the industry-occupation cell sizes
|
Size of Cell |
||||||
|
With no education variable |
||||||
|
2 or more |
3 or more |
4 or more |
10 or more |
30 or more |
||
|
CDF percentile |
5 |
-0.253 |
-0.281 |
-0.291 |
-0.256 |
-0.381 |
|
10 |
-0.248 |
-0.272 |
-0.281 |
-0.289 |
-0.369 |
|
|
50 |
-0.224 |
-0.243 |
-0.235 |
-0.271 |
-0.336 |
|
|
90 |
-0.192 |
-0.209 |
-0.214 |
-0.298 |
-0.296 |
|
|
95 |
-0.183 |
-0.199 |
-0.208 |
-0.255 |
-0.288 |
|
|
With higher education |
||||||
|
2 or more |
3 or more |
4 or more |
10 or more |
30 or more |
||
|
CDF percentile |
5 |
-0.097 |
-0.108 |
-0.124 |
-0.125 |
-0.144 |
|
10 |
-0.073 |
-0.095 |
-0.100 |
-0.103 |
-0.111 |
|
|
50 |
-0.030 |
-0.039 |
-0.047 |
-0.047 |
-0.066 |
|
|
90 |
0.020 |
0.001 |
0.006 |
0.011 |
-0.022 |
|
|
95 |
0.042 |
0.018 |
0.012 |
0.014 |
-0.014 |
|
|
No of Jobs |
758,490 |
743,365 |
731,509 |
680,870 |
316,570 |
|
Source: NVSS and CPS micro data.
In addition to the sensitivity analysis above, a more in-depth analysis of the instruments themselves is shown in the annex. There, estimates using only right to work laws and only pre-emption are shown, as well as instruments constructed net of possible confounding factors such as income, infant mortality and number of hospital beds per 1,000 people. In all cases the results still hold, usually with very little substantive change.
Conclusion
Information from collective agreements as well as previous literature demonstrate how unions support both stronger regulations at workplace such as paid sick leave and more rigorous OSH protocols, in addition to improving compliance with regulations. Furthermore, the greater protections against dismissal that are prominent in most collective bargaining agreements give workers greater voice in expressing their concerns, which can be critical in the face of safety and health hazards. During the COVID-19 pandemic, unions were effective in securing enhanced OSH protections, such as access to PPE, restrictions on number of persons at a worksite and greater access to COVID-19 testing and leave. As documented by Dean et al. (2022), these efforts were effective in saving lives among nursing home residents but also in reducing infections among staff.
This paper builds on the existing literature on the effect of unionization on OSH by providing an analysis of unionization’s effects on COVID-19 mortality during 2020. It combines data from the NVSS with the CPS into a unique dataset. It finds that a 10 percentage-point increase in unionization is associated with a reduction in mortality from 26 per 100,000 workers to 24 per 100,000 workers. This means that if the United States had the union density of 35 percent that it had in 1954 instead of today’s rate of 10 percent, the COVID-19 mortality rate for working people would fall from 26 to 19 per 100,000. While there are obviously strong hypotheses behind this counterfactual, we believe that this paper, together with the previous literature, demonstrates that unions do indeed save lives.
Annex: Validity of the Instruments
For an instrumental variable to be valid, three conditions must be met.
The first is relevance. The instrument must be correlated with the endogenous variable. In our case, this is easily met: states without Right to Work Laws and with limited pre-emption have higher unionization. If this condition were not met, the first stage equation would not even produce significant results.
The second is the exclusion restriction: the instrument affects the dependent variable only through the endogenous variable. In other words, there can be no direct causal relationship between Right to Work Laws or pre-emption and our final variable, mortality. It is not hard to argue this since there is no plausible story in which either Right to Work Laws or pre-emption could possibly increase or decrease COVID-19 mortality and even less be caused by COVID-19 mortality.
Nevertheless, in order to further argue both relevance and the exclusion restriction, estimates with only one of the two IV models were also made. The results of the first stage are shown below.
Table A1 – Only one instrumental variable: First stage results
|
|
Linear probability model |
||||||||
|
Union |
Coef. |
p-value |
Coef. |
p-value |
Coef. |
p-value |
Coef. |
p-value |
|
|
Right to work |
-0.085 |
0% |
-0.085 |
0% |
|||||
|
Pre-emption |
0.029 |
0% |
0.029 |
0% |
|||||
|
Higher education |
0.009 |
0% |
0.010 |
0% |
|||||
|
Age |
0.006 |
0% |
0.006 |
0% |
0.006 |
0% |
0.006 |
0% |
|
|
Age2 |
0.000 |
0% |
0.000 |
0% |
0.000 |
0% |
0.000 |
0% |
|
|
Sex (male) |
-0.013 |
0% |
-0.013 |
0% |
-0.014 |
0% |
-0.014 |
0% |
|
|
Race (relative to white) |
|
|
|
|
|
|
|
|
|
|
Black |
0.013 |
0% |
0.013 |
0% |
0.011 |
0% |
0.011 |
0% |
|
|
Native American |
-0.034 |
0% |
-0.034 |
0% |
-0.037 |
0% |
-0.037 |
0% |
|
|
Asian |
-0.004 |
4% |
-0.004 |
7% |
0.002 |
26% |
0.003 |
19% |
|
|
Other |
0.012 |
0% |
0.012 |
0% |
0.016 |
0% |
0.016 |
0% |
|
|
R2 |
0.1600 |
0.1599 |
0.1507 |
0.1506 |
|||||
|
Number of obs |
402,457 |
402,457 |
402,457 |
402,457 |
|||||
|
Prob > chi2 |
0.00% |
|
0.00% |
|
|
0.00% |
|
0.00% |
|
|
Probit |
|||||||||
|
Union |
Coef. |
p-value |
Coef. |
p-value |
Coef. |
p-value |
Coef. |
p-value |
|
|
Right to work |
-0.516 |
0% |
-0.516 |
0% |
|||||
|
Pre-emption |
0.178 |
0% |
0.178 |
0% |
|||||
|
Higher education |
0.052 |
0% |
0.053 |
0% |
|||||
|
Age |
0.044 |
0% |
0.045 |
0% |
0.043 |
0% |
0.043 |
0% |
|
|
Age2 |
0.000 |
0% |
0.000 |
0% |
0.000 |
0% |
0.000 |
0% |
|
|
Sex (male) |
-0.090 |
0% |
-0.090 |
0% |
-0.091 |
0% |
-0.092 |
0% |
|
|
Race (relative to white) |
|
|
|
|
|
|
|
|
|
|
Black |
0.099 |
0% |
0.098 |
0% |
0.087 |
0% |
0.086 |
0% |
|
|
Native American |
-0.188 |
0% |
-0.192 |
0% |
-0.204 |
0% |
-0.208 |
0% |
|
|
Asian |
-0.004 |
76% |
-0.002 |
88% |
0.030 |
1% |
0.032 |
1% |
|
|
Other |
0.076 |
0% |
0.077 |
0% |
0.098 |
0% |
0.098 |
0% |
|
|
Number of obs |
402,457 |
402,457 |
402,457 |
402,457 |
|||||
|
Prob > chi2 |
0.00% |
|
0.00% |
|
|
0.00% |
|
0.00% |
|
Table A1 shows that using only one of the instruments does not change the results relative to Table 2 in the main text. The coefficients for right to work increase only slightly from the -0.083 estimated using both instruments to -0.085. Those for pre-emption increase by a factor of ten from 0.002 to 0.029. This is likely because each variable is picking up some of the variation from the other.
Table A2, below, though, shows that using only one instrument makes no difference vis-à-vis the estimated results.
Table A2 – IV Regression Results using only one IV: Second stage results
|
5 |
10 |
50 |
90 |
95 |
|
|
Original estimates |
-0.228 |
-0.221 |
-0.189 |
-0.160 |
-0.151 |
|
Only pre-emption |
-0.233 |
-0.222 |
-0.194 |
-0.167 |
-0.156 |
|
Only right to work |
-0.226 |
-0.215 |
-0.185 |
-0.154 |
-0.148 |
Source: CPS and NVSS microdata; Economic Policy Institute; National Conference of State Legislatures.
The coefficients given to us by the regressions involving only one of the two instruments are essentially the same as the original estimates.
Finally, there is unconfoundedness. This means that the Instrument is not correlated with any other unobserved variables which may have a causal relationship with the outcome variable. This is harder to argue, since Right to Work Laws and pre-emption are more likely to be found in more conservative states which are also poorer and have worse health outcomes in general.
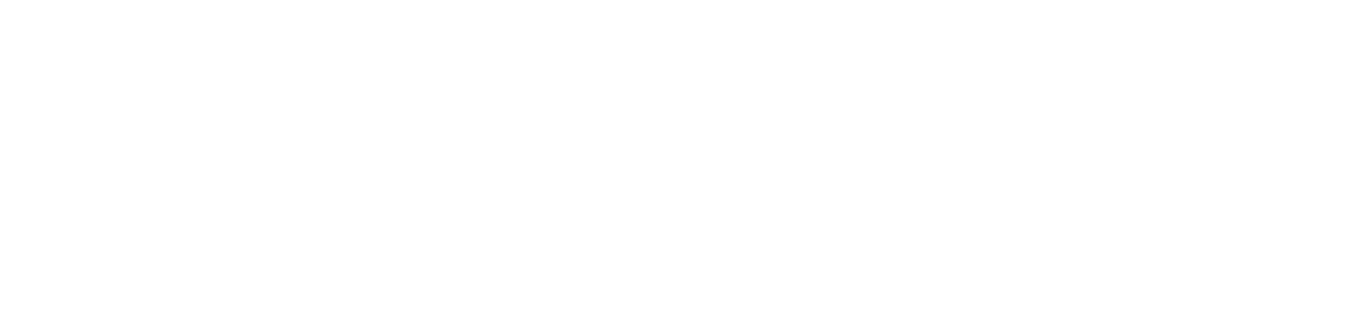
Figure A1 shows that Right to Work states have lower per capita incomes and higher infant mortality then those without such laws. In the other direction, Right to Work states have slightly more hospital beds. This suggests that laws that are barriers to unionization occur more frequently in places where other variables may lead to higher COVID-19 mortality.
Figure A1. Distribution of Income, Hospital Beds and Infant Mortality, by State, According to Right to Work Laws
|
Per Capita Income |
Hospital Beds per 1,000 People |
Infant Mortality per 1,000 Births |
|
|
|
|



Sources:
Per capita income by state: Bureau of Economic Analysis (https://apps.bea.gov/regional/downloadzip.cfm).
Hospital beds: Becker's Hospital Review.
Infant mortality: CDC Wonder (https://wonder.cdc.gov/WelcomeT.html)
T-tests of equal means between Right to Work states and the others show that the means are not equal with p-values indistinguishable from zero.
Table A2 – T-tests for difference in means between RTW states and other states
|
Variable |
Difference |
SE of difference |
Probability difference is zero |
|
Incomes |
10070.16 |
2221.751 |
0.01% |
|
Hospital beds |
-0.4773611 |
0.2011028 |
2.16% |
|
Infant mortality |
-1.355231 |
0.24873 |
0.01% |
Sources:
Per capita income by state: Bureau of Economic Analysis (https://apps.bea.gov/regional/downloadzip.cfm).
Hospital beds: Becker's Hospital Review.
Infant mortality: CDC Wonder (https://wonder.cdc.gov/WelcomeT.html)
In the case of pre-emption, the relationship is less clear cut. Table A3 shows the correlation between the pre-emption score and the same three variables above. While states with more pre-emption (less union-friendly) tend to have fewer hospital beds (less investment in health), they also have lower infant mortality and higher incomes.
Table A3 – Correlation between pre-emption, income, hospital beds per 1,000 and infant mortality
|
|
Per capita income |
Beds per 1,000 |
Infant mortality |
Pre-emption score |
|
Per capita income |
1 |
|
|
|
|
Beds per 1,000 |
-0.0462 |
1 |
||
|
Infant mortality per 1,000 births |
-0.6246 |
0.4994 |
1 |
|
|
Pre-emption score |
0.6171 |
-0.1504 |
-0.6142 |
1 |
Sources:
Per capita income by state: Bureau of Economic Analysis (https://apps.bea.gov/regional/downloadzip.cfm).
Hospital beds: Becker's Hospital Review.
Infant mortality: CDC Wonder (https://wonder.cdc.gov/WelcomeT.html)
The conclusion to be had is that it is difficult to make a compelling argument for unconfoundedness. The argument we will make is that it makes no difference. In order to do so, we will repeat the exact same instrumental variable procedure, but using the residuals of a regression in which Right to Work and pre-emption are explained by income, beds per 1,000 and infant mortality. By definition, these residuals will be orthogonal to all the explanatory variables and thus the confoundedness (at least with relation to these three variables) will be netted out.
Table A4 – Regressions explaining right to work and pre-emption
|
RTW |
Coefficient |
p-value |
|
income per capita |
-0.00002 |
0.028 |
|
Beds |
0.09378 |
0.313 |
|
infant mortality |
0.14694 |
0.07 |
|
Constant |
0.53292 |
0.475 |
|
pre-emption |
Coefficient |
p-value |
|
income per capita |
0.00004 |
0.024 |
|
Beds |
0.11426 |
0.521 |
|
infant mortality |
-0.39570 |
0.013 |
|
Constant |
-0.25738 |
0.857 |
Sources:
Per capita income by state: Bureau of Economic Analysis (https://apps.bea.gov/regional/downloadzip.cfm).
Hospital beds: Becker's Hospital Review.
Infant mortality: CDC Wonder (https://wonder.cdc.gov/WelcomeT.html)
Using the residuals from the two equations above, the whole IV procedure was repeated. The results are on Table A5 and, once again, show very clearly that it makes no difference.
Table A5 – IV Regression Results using residuals as IVs
|
|
5 |
10 |
50 |
90 |
95 |
|
Original estimates |
-0.228 |
-0.221 |
-0.189 |
-0.160 |
-0.151 |
|
Residuals |
-0.220 |
-0.203 |
-0.189 |
-0.194 |
-0.183 |
The estimate (column labelled 50) changes by almost nothing when using residuals: the changes are only in the fourth decimal place. Not only do the point estimates not change, but their distribution stays surprisingly the same.
One last table which we would like to include are the results using probit instruments (as opposed to estimates from a linear probability model), while Wooldridge (2010) discourages their use since they are consistent only in certain cases, we will include the results for the sake of completeness. Table A6 shows the first stage results.
Table A6 – Determinants of Unionization (Probit)
|
|
|
Probit |
|||
|
Union |
Coef. |
p-value |
Coef. |
p-value |
|
|
Right to work |
-0.500 |
0% |
-0.500 |
0% |
|
|
Pre-emption |
0.012 |
0% |
0.012 |
0% |
|
|
Higher education |
0.052 |
0% |
|||
|
Age |
0.045 |
0% |
0.044 |
0% |
|
|
Age2 |
0.000 |
0% |
0.000 |
0% |
|
|
Sex (male) |
-0.090 |
0% |
-0.090 |
0% |
|
|
Race (relative to white) |
|||||
|
Black |
0.099 |
0% |
0.100 |
0% |
|
|
Native American |
-0.194 |
0% |
-0.190 |
0% |
|
|
Asian |
-0.004 |
74% |
-0.006 |
63% |
|
|
Other |
0.076 |
0% |
0.075 |
0% |
|
|
Number of obs |
402,457 |
402,457 |
|||
|
Prob > chi2 |
|
0.00% |
|
0.00% |
|
Source: CPI microdata; Economic Policy Institute; National Conference of State Legislatures.
While the coefficients are different in magnitude from the linear probability model (as would be expected), all are significant and have the same sign.
Table A7 - shows the bootstrapped results for the second stage for the effect of unionization on mortality.
|
|
CDF percentile - no education |
|
CDF percentile - higher education |
||||||||
|
Variable |
5 |
10 |
50 |
90 |
95 |
|
5 |
10 |
50 |
90 |
95 |
|
Union density |
-0.212 |
-0.228 |
-0.232 |
-0.224 |
-0.235 |
-0.093 |
-0.077 |
-0.013 |
0.028 |
0.052 |
|
|
Higher education |
-0.106 |
-0.104 |
-0.096 |
-0.089 |
-0.088 |
||||||
|
Sex |
0.402 |
0.398 |
0.401 |
0.400 |
0.407 |
0.146 |
0.148 |
0.156 |
0.165 |
0.167 |
|
|
Age |
0.028 |
0.030 |
0.034 |
0.033 |
0.030 |
0.089 |
0.091 |
0.094 |
0.098 |
0.098 |
|
|
Age2 |
0.000 |
0.000 |
0.000 |
0.000 |
0.000 |
-0.001 |
-0.001 |
-0.001 |
-0.001 |
-0.001 |
|
|
Race (relative to white) |
|||||||||||
|
Black |
0.225 |
0.227 |
0.227 |
0.226 |
0.227 |
|
0.136 |
0.142 |
0.152 |
0.164 |
0.165 |
|
Native American |
0.259 |
0.242 |
0.199 |
0.278 |
0.266 |
0.309 |
0.324 |
0.353 |
0.377 |
0.379 |
|
|
Asian |
-0.060 |
-0.034 |
-0.047 |
-0.046 |
-0.039 |
0.321 |
0.326 |
0.347 |
0.370 |
0.373 |
|
|
Other |
-0.620 |
-0.595 |
-0.593 |
-0.614 |
-0.554 |
|
-0.365 |
-0.340 |
-0.255 |
-0.158 |
-0.127 |
Source: CPI and NVSS microdata; Economic Policy Institute; National Conference of State Legislatures.
Other than the results becoming somewhat stronger, there is no effect when using probit estimates in the first stage of the estimation.
References
Ahmad FB, Cisewski JA, Miniño A, Anderson RN. Provisional Mortality Data — United States, 2020. MMWR Morbidity and Mortality Weekly Rep 2021;70:519–522. DOI: http://dx.doi.org/10.15585/mmwr.mm7014e1
Acknowledgements
The authors would like to thank Margaret Poydock at EPI for help with finding data; Pedro H. G. F. Souza and Hannah Liepmann for detailed comments on earlier drafts, and participants at the research seminar of the ILO’s Research department for value feedback.

