
What role can health mutuals and community-based health insurance play in social health protection systems?
Review of experiences
Abstract
Social health protection systems are constantly evolving, offering a wide range of institutional, administrative, and financial arrangements. International standards in social health protection are outcome-based, and grant flexibility in the institutional and administrative arrangements chosen by each state to implement these guarantees, as long as certain fundamental principles are upheld. These principles include the establishment of state-guaranteed benefit entitlements, solidarity in financing, and broad risk pooling. The flagship Social Security (Minimum Standards) Convention, 1952 (No. 102), globally recognized as a reference for system design, is thus conceived around the idea that systems are adaptable and that no single model applies universally.
At the global level, mutuals primarily focus on providing complementary or supplementary coverage to basic health schemes. Only a small number of countries incorporate mutuals and community-based health insurance (CBHI) into the architecture of their basic health coverage systems. This working paper explores various country experiences where mutuals and CBHI contribute to basic health coverage within national social protection systems. Despite a wealth of literature on mutuals and CBHI, little is known about the practical methods used to integrate them into national social health protection architectures.
This work is based on a literature review (Niang et al., 2023) and seventeen case studies spanning countries in Europe, Africa, Asia, and Latin America.
This comparative analysis highlights that the involvement of mutuals and AMBCs in national social health protection schemes is the result of a historical process unique to each country, evolves dynamically over time, and varies significantly in the conceptual and legal frameworks that govern them.
Executive Summary
Social health protection (SHP) is a human right rooted in the right to social security and the right to health enshrined in the Universal Declaration of Human Rights (1948) and the International Covenant on Economic, Social and Cultural Rights (1966). This fundamental right is formalized through a range of legal instruments, including ILO standards, 1 which provide a flexible framework for the progressive expansion of all types of social protection system based on social solidarity.
Today, it contributes to the achievement of the Sustainable Development Goals (SDGs) of the 2030 Agenda for Sustainable Development (2030 Agenda), particularly targets 1.3 and 3.8 on universal social protection and universal health coverage (UHC), which is a priority shared at the global level. In addition to the availability of a quality healthcare system, UHC relies on social protection strategies for health, based on the values of solidarity and social justice. These strategies aim to free the demand for healthcare from its financial constraints, thereby enabling everyone to have access to healthcare services regardless of their resources, in the event of illness, accident or disability.
Social health protection systems are constantly evolving and there is now a variety of institutional, administrative and financial arrangements. International standards in SHP are results-based and are not prescriptive in terms of the institutional and administrative arrangements chosen by each State to implement these guarantees, provided that they respect certain basic principles, including the establishment of state-guaranteed benefit entitlements, solidarity in financing and broad risk pooling. The flagship Social Security (Minimum Standards) Convention, 1952 (No. 102), which is recognized worldwide as a benchmark for the development of systems, is built around the idea that systems are flexible and that there is no single model.
At the global level, the role of mutual benefit societies (mutuals) tends to be focused on complementary or supplementary cover to the basic health cover scheme and only a small proportion of countries use mutuals and community-based health insurance (CBHI) in their basic health cover scheme architecture. This working paper examines these different country experiences where mutuals and CBHI have a role in basic health cover within the national social protection system. Despite an abundance of literature on mutuals and CBHI, the description of the operational methods used to integrate them into national SHP systems architecture is still not widely documented and the scope of the definitions varies widely, making comparisons difficult.
The terms "mutual" and "community-based health insurance" are often used interchangeably in the literature. Yet they often refer to very different realities. These two terms tend to bring together a heterogeneous range of organizations from the social and solidarity-based economy, national programmes or even from processes of decentralization of public schemes, which do not all share the common and commonly understood characteristics of mutuality. For the purposes of this working paper, the term mutual is therefore used in a very broad sense, reflecting this diversity, and a more precise classification is also proposed.
This work is based on a literature review
This comparative analysis shows that the involvement of mutuals/CBHI in national SHP schemes is the result of an historical process specific to each country concerned, changes significantly over time and there is great variability in the conceptual and legal frameworks in which they operate.
In countries where mutuals/CBHI have developed in the absence of an organized national SHP system, these have frequently led to an increased use of healthcare by beneficiaries and to their financial protection. On the other hand, they have not led to a significant increase in population coverage and have encountered problems of financial viability, including linked to the low level of pooling of funds.
The experiences that have been successful in terms of extending cover are those in which:
-
from the outset, a national SHP system led to the creation of community mechanisms to ensure its integrated implementation at the local level (Lao People’s Democratic Republic, Rwanda, United Republic of Tanzania);
-
the national SHP institution absorbed the mutuals or CBHI that existed prior to the creation of the national SHP system (Cambodia, Ghana); and
-
the SHP scheme has delegated certain management functions, generally to mutuals or CBHI that existed prior to the SHP system (Belgium, Colombia, Côte d’Ivoire, France, Germany, Japan, Morocco, Uruguay).
In several countries, the role of mutuals within SHP systems has evolved between these different models, which can thus be seen as a continuum in some countries. Conversely, some cases do not yet fall into these categories, where the system is still under construction, as in Burkina Faso.
The experiences where true delegation of management took place:
-
mainly concern “front office” functions, with the “back office” functions (design of scheme parameters, pooling of funds and risks) remaining a public function; and
-
have been facilitated by the clear architecture of the SHP system, with public funding and compulsory membership, and by a professionalization of actors.
The option of integrating mutuals into the implementation of the national strategy for UHC requires the organization of an enabling environment (see below):
-
When management is delegated, it must necessarily be based on an agreement between the health insurance administrator and the mutual in order to clearly define the objectives of the delegation, the mutual’s remit and the operating procedures. The examples observed in Côte d'Ivoire, France, Mali, and Morocco show that these agreements also impose technical constraints on mutuals so as to guarantee their ability to fulfil their functions.
-
Delegation of management must take place within a clear political and regulatory framework. The role of the State is important. It must lead a national dialogue with all stakeholders in order to define the fundamental principles of health insurance and then put in place oversight and regulatory measures.
In countries where SHP systems are emerging, external partners and national non-governmental organizations (NGOs) often influence national options oriented towards CBHI. This responds to the concerns over short-term results of development support programmes. However, building sustainable SHP requires long-term investment.
Introduction
Social health protection (SHP) is a human right rooted in the right to social security and the right to health enshrined in the Universal Declaration of Human Rights (1948) and the International Covenant on Economic, Social and Cultural Rights (1966). This fundamental right is formalized through a range of legal instruments, including ILO standards, which provide a flexible framework for the progressive expansion of all types of social protection system based on social solidarity.
Today, it contributes to the achievement of the Sustainable Development Goals (SDGs) of the 2030 Agenda for Sustainable Development (2030 Agenda), particularly targets 1.3 and 3.8 on universal social protection and universal health coverage (UHC), which is a priority shared at the global level. In addition to the availability of a quality healthcare system, UHC relies on social protection strategies for health, based on the values of solidarity and social justice. These strategies aim to free the demand for healthcare from its financial constraints, thereby enabling everyone to have access to healthcare services regardless of their resources, in the event of illness, accident or disability.
International SHP standards are results-based and are not prescriptive in terms of the institutional and administrative arrangements chosen by each State to implement these guarantees, provided that they respect certain basic principles, including the establishment of state-guaranteed benefit entitlements, solidarity in financing and broad risk pooling. These standards recognize that any system must be adapted to domestic circumstances to be acceptable and effective and that countries may use different approaches to achieve the goal of universal protection through the optimal mix of different institutional arrangements and sources of financing. Countries that have achieved universal coverage in SHP generally combine a variety of funding sources and institutional mechanisms. The flagship Social Security (Minimum Standards) Convention, 1952 (No. 102), which is recognized worldwide as a benchmark for the development of systems, is built around the idea that systems are flexible and that there is no single social security model. Every country must work to develop its own sustainable and progressively comprehensive social protection system, in a manner adapted to national circumstances (ILO, 2020b). In practice, the chosen administrative architecture for the provision of SHP benefits varies from country to country, and mutual benefit societies (mutuals) or community-based health insurance (CBHI) have been identified as playing a role
At the global level, the role of mutuals tends to be focused on complementary or supplementary cover to the basic health cover scheme. However, some countries, which have embarked on major reforms of their health and social protection systems, use mutuals in their basic health cover scheme architecture. These processes have prompted this review of experiences, with a view to examining the role given to mutuals and the methods used for implementation.
Historically, mutuals developed in Europe, Japan and Latin America in contexts where the public protection system was nascent
Despite an abundance of literature on mutuals, the description of the operational methods used to integrate them into national SHP systems architecture is still not widely documented and the scope of the definitions varies widely, making comparisons difficult. This work is also based on a previous literature review
This document presents a summary of these studies, organized into three main sections (see below).
-
The first section proposes a set of definitions of SHP and mutuals in order to map out the scoping review.
-
The second section provides an overview of the role of mutuals and CBHI within SHP systems, based in particular on the above-mentioned scoping review and the 17 countries selected for the case studies.
-
Lastly, the third section deals specifically with the delegation of management and proposes various lessons drawn from these experiences, concerning the current and potential role of mutuals in the context of the West African Economic and Monetary Union (WAEMU).
This summary is followed by case studies for each country.
Conceptual framework
Key messages
-
Countries have a wide range of institutional, administrative and financial arrangements for constructing their national SHP systems, with a common objective of moving progressively towards UHC.
-
The current and interchangeable use of the terms “mutual” and “CBHI” covers very different circumstances; there is not always conceptual clarity in their use, nor a single legal framework at the global level to oversee them.
-
The characteristics of these entities (mutuals/CBHI) are also influenced by the role they play in the SHP system in some countries.
1.1. Social health protection
The ILO defines social health protection (SHP) as "a series of public or publicly organized and mandated private measures against social distress and economic loss caused by the reduction of productivity, stoppage or reduction of earning or the cost of necessary treatment that can result from ill health” (Scheil-Adlung, 2007). SHP is firmly grounded in international law: the Universal Declaration of Human Rights, the International Covenant on Economic, Social and Cultural Rights, ILO Convention No. 102 and the Social Protection Floors Recommendation, 2012 (No. 202). The latter defines SHP as access to healthcare without financial hardship, guaranteed by the State over the life cycle, and income security in cases of sickness and maternity. It contributes to the achievement of the SDGs under the 2030 Agenda, and in particular targets 1.3 and 3.8 on universal social protection and universal health coverage (box 1).
Box 1. Universal social protection throughout the life cycle and universal health coverage: Two key goals of the 2030 Agenda for Sustainable Development (2030 Agenda)
Universal social protection (USP) is firmly grounded in the international human rights framework and international social security standards, including the Universal Declaration of Human Rights, the International Covenant on Economic, Social and Cultural Rights, ILO Convention No. 102 and Recommendation No. 202. USP refers to comprehensive, sustainable and adequate protection for all throughout the life cycle, according to the three core dimensions described below.
-
Universal coverage for persons protected. All should have effective access to social protection throughout the life cycle, if and when needed.
-
Comprehensive protection with regard to the social risks and contingencies that are covered. This includes access to healthcare and income security. Convention No. 102 sets out nine contingencies that every person may face over the course of life. These are the need for medical care and the need for benefits in the event of: sickness; unemployment; old-age; employment injury; family responsibilities; maternity; invalidity; and survivorship (paid to certain relatives in the event of the death of a breadwinner). This dimension also includes protection against new and emerging risks, such as long-term care needs.
-
Adequate protection. Benefits provided need to be set at a level that effectively prevents poverty, vulnerability and social exclusion, maintains a decent standard of living and allows people to lead healthy and dignified lives (ILO, 2021).
In the SDGs, progress on USP is measured through indicator 1.3.1 – Proportion of population covered by social protection floors/systems.
Universal health coverage is defined by the World Health Organization (WHO) as a situation in which all people have access to the full range of quality health services they need, when and where they need them, without financial hardship. It covers the full continuum of essential health services, from health promotion to prevention, treatment, rehabilitation, and palliative care across the life course.
In the SDGs, progress on UHC is measured through two indicators:
-
coverage of essential services (SDG indicator 3.8.1)
-
catastrophic health spending (and related indicators) (SDG indicator 3.8.2)
Virtually all countries have constructed systems based on a combination of different financing mechanisms, which translates into a wide variety of systems on an international scale. This is the result of a pragmatic approach by each country to dealing with a number of specific problems linked to the distribution of the population geographically and by category, the availability of health services, decentralized administration, and so on. International social protection standards recognize this plurality in the institutional and administrative arrangements that each State chooses to implement these guarantees, provided that they respect certain basic principles, in order to build systems that are adapted to domestic circumstances, and are acceptable, effective and financially sustainable (see box 2).
Box 2. International social health protection standard
Universality
The Medical Care Recommendation, 1944 (No. 69) introduced the principle of universality, setting out that healthcare services should cover all members of the community, “whether or not they are gainfully occupied” (para. 8). The right to health was subsequently formally enunciated by human rights instruments. The human rights to health and social security create an obligation to guarantee universal effective access to adequate protection. In this context, SHP represents the optimal mechanism for substantiating these human rights (ILO, 2020).
Financing and institutional arrangements
International social security standards promote collectively financed mechanisms to cover the costs of health services, recognizing recourse to taxes and contributions made by workers, employers and government. Likewise, these standards recognize a range of institutional arrangements, namely national healthcare services, by which public services deliver affordable health interventions, and national social health insurance, by which an autonomous public entity collects revenues from different sources (social contributions and/or government transfers) to purchase health services, either only from public providers, or from both public and private providers. In practice, most countries use a combination of financing sources and institutional arrangements to achieve universal coverage for their population.
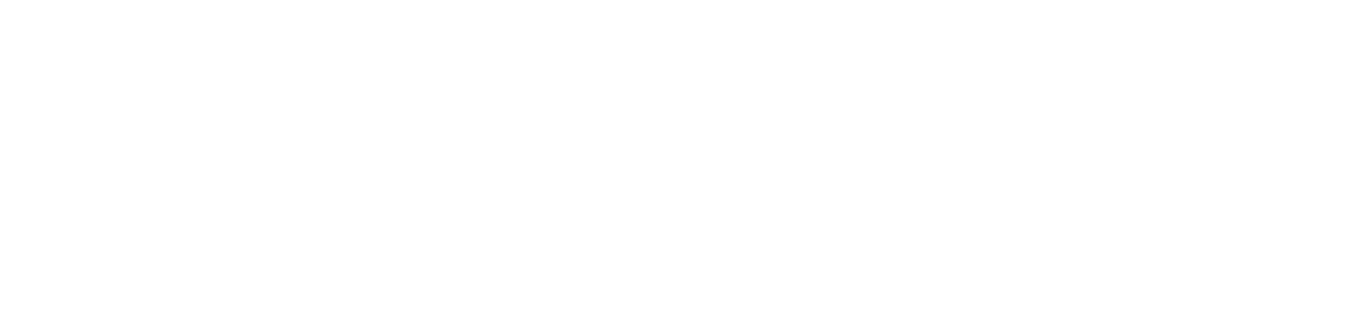
The ILO underlines that “there is no one-size-fits-all approach. International standards provide guiding principles for Governments to ensure universal protection in a way that reflects risk-sharing, equity and solidarity in a fiscally, economically and socially sustainable fashion” (ILO, 2020). Strategies to extend coverage have a twofold objective (see below).
-
Horizontal extension of coverage aims to cover the entire population with at least a minimum level of protection across four basic social protection floor guarantees, including healthcare, in line with ILO Recommendation No. 202).
-
Vertical extension of coverage aims to improve benefit adequacy progressively, ensuring higher levels of protection. International social security standards establish a minimum level of benefit to be guaranteed by law, encompassing two dimensions:
-
range of services actually accessible
-
financial protection against the costs of such services
With respect to the first element, the range of services to be included has to be progressively widened. While social protection floors should include the provision, at a minimum, of “essential healthcare” as defined nationally, including free prenatal and postnatal care for the most vulnerable, countries should progressively move towards greater protection for all, as reflected in Convention No. 102 and the Medical Care and Sickness Benefits Convention, 1969 (No. 130), which stipulate the provision in national law of access to a comprehensive range of services. To be considered adequate, in line with human rights compliance monitoring mechanisms, health services need to meet the criteria of availability, accessibility, acceptability and quality (Recommendation No. 202, Para. 5(a)).
With respect to the second element (financial protection), ILO instruments provide for the right to healthcare “without financial hardship”. Direct payments from households should not be a primary source of financing for healthcare systems. The rules regarding cost-sharing must be designed to avoid hardship, with no or limited contributions and free maternity care.
As illustrated in figure 1, once countries have achieved effective protection for the entire population covering a range of services and financial protection aligned with guaranteed levels of protection in conformity with international standards, complementary and supplementary mechanisms can be put in place under state regulation.
Figure 1. Two-dimensional strategy on the extension of coverage
Source: ILO, 2012.
Within this framework, the State, which is responsible for the SHP system, may choose to entrust one or more ministries or public agencies with its implementation. They may also delegate certain functions to operational bodies. For example, Indonesia has a national health insurance agency, Malaysia has a very low-cost national public health service managed by the Ministry of Health, Thailand has three public agencies covering different population groups, and Switzerland mandates private insurers to implement compulsory, collectively financed health insurance. All of these systems also tend to regulate voluntary private insurance to cover services deemed non-essential (elective surgery, and so on), or to complement basic financial protection by covering the co-payment or additional services (single room during hospitalization, and so on).
1.2. Mutuals and community-based health insurance
The terms "mutual" and "community-based health insurance" (CBHI) (the latter in English describing health insurance mechanisms put in place at the community level) are generally used interchangeably in the literature. However, these organizations often refer to distinct circumstances, and these terms tend to draw together a heterogeneous mix of organizations from the social and solidarity economy, national programmes and even the process to decentralize public schemes, which do not all share the common and generally understood characteristics of mutuality.
This reflects a more general diversity within the social and solidarity economy, where definitions differ according to national contexts as well as the legal framework (ILO, 2022), which can act as a brake on the delegation of public services. However, an international definition was adopted by the ILO in 2022 and then taken up by the United Nations General Assembly in 2023: 2
“The [social and solidarity economy (SSE)] encompasses enterprises, organizations and other entities that are engaged in economic, social, and environmental activities to serve the collective and/or general interest, which are based on the principles of voluntary cooperation and mutual aid, democratic and/or participatory governance, autonomy and independence, and the primacy of people and social purpose over capital in the distribution and use of surpluses and/or profits as well as assets. SSE entities aspire to long-term viability and sustainability, and to the transition from the informal to the formal economy and operate in all sectors of the economy. They put into practice a set of values which are intrinsic to their functioning and consistent with care for people and planet, equality and fairness, interdependence, self-governance, transparency and accountability, and the attainment of decent work and livelihoods. According to national circumstances, the SSE includes cooperatives, associations, mutual societies, foundations, social enterprises, self-help groups and other entities operating in accordance with the values and principles of the SSE.” (ILC.110/Resolution II, part II). 5.)
Furthermore, some countries have used the term "mutual" to designate decentralized public administration bodies (Niang et al., 2023). The use of the terms "mutuality" and "mutuals" thus covers a wide range of organizations from the social and solidarity economy.
The International Association for Mutual Benefit Societies (AIM) confirms that there is no clear definition and that there is a diversity of legal forms. However, the AIM underscores that mutuals have five main characteristics:
-
Mutuals are private legal entities.
-
Mutuals are a grouping of people.
-
The governance of mutuals is democratic.
-
The principle of solidarity is very important among members.
-
Profits are used for the benefit of the members (AIM, 2017).
Box 3. Examples of definitions from around the world
In Europe
In March 2013, the European Parliament adopted a legislative own-initiative report on the Statute for a European mutual society, with the aim of increasing the visibility and recognition of mutuality at the European level and allowing mutual societies to access and benefit from the internal market. The European Commission defined mutual societies as “an autonomous association of persons (legal entities or natural persons) united voluntarily, whose primary purpose is to satisfy their common needs and not to make profits or provide a return on capital. It is managed according to solidarity principles between members who participate in the corporate governance. It is therefore accountable to those whose needs it is created to serve”. There is therefore no clear legal concept of what defines a mutual-type organization in the various Member States, as there are differences concerning traditions, history, (political) choices, markets, governance models and rules. However, the 2013 own-initiative report identifies a set of essential traits (see below) that differentiate mutuals from other economic agents.
-
Mutuals are private entities governed by private law, independent and neither controlled by the government nor funded by public subsidies.
-
Mutuals are a grouping of persons (physical or moral) and a pooling of funds.
-
They are subject to democratic governance.
-
Mutuals organize services and provisions in the interests of their members, on a basis of solidarity and in a collectively financed manner.
-
In return, the members pay a contribution or equivalent, the amount of which may be variable.
-
The members cannot exercise any individual right over the assets of the mutual.
-
The profits are used for the benefit of its members (discounted premiums, and so on) or are reinvested to improve services for the members (ISSA, 2013).
Within the West African Economic and Monetary Union (WAEMU)
A definition is also provided in West Africa through Directive No. 07/2009/CM/UEMOA on regulating social mutual schemes within the WAEMU (2009). This defines mutual organizations, including mutual health organizations, as “associations which, primarily through their members' contributions, aim to carry out, in the interest of their members and their dependants, action in terms of a provident fund, mutual assistance and solidarity to prevent social risks related to the person and to address their consequences”. Article 12 of the Directive sets out the principles for mutuals that distinguish them from other forms of insurance. These principles are described below.
-
Voluntary and non-discriminatory membership consists of a voluntary act of participation in a social mutual society not based on gender, race, nationality, political or religious affiliation.
-
Not-for-profit means that activities are carried out for a purpose other than making a profit.
-
Democratic and participative operation means the participation of members, either directly or through their representatives, in the running of the institution.
-
The commitment to solidarity is based on mutual aid between members, with a view to sharing the risks.
-
Autonomy and independence entail the free administration of the institution's assets in compliance with prudential regulation.
-
Voluntary work means that members of the governing body perform their duties free of charge.
-
Responsible participation obliges members to observe a certain loyalty towards the institution and towards other members.
In Japan
The Ministry of Health, Labour and Welfare defines mutual aid associations as "a social security system designed to help cooperative members help each other and improve the stability and welfare of each other's lives" (Ministry of Health, Labour and Welfare of Japan, daini kyosei kumiai 2020).
In Colombia
Mutual associations are not-for-profit enterprises in the solidarity economy, under private law and solidarity-based with social-interest objectives, freely and democratically constituted by the association of natural persons, not-for-profit legal entities or a combination thereof, which undertake to make contributions to the mutual social fund, in order to help each other to meet their needs and those of the community in general, always with a view to social interest or collective welfare (Law No. 2143 of 2021, article 2).
According to these definitions, a mutual organization is a not-for-profit association of persons (membership being voluntary) with the aim of dealing with the consequences of various social risks for its members and their families. A mutual is financed primarily by its members' contributions, which may be supplemented by other resources, including state subsidies. It is managed by the representatives of its members, and a mutual enjoys complete institutional independence provided it complies with certain principles set out in law. It therefore differs from other SHP mechanisms in that it has a democracy less removed from its contributing members. Mutuals also differ from commercial health insurance in that it is not-for-profit, has a much higher degree of solidarity in a number of respects, and is democratic (Boyer et al., 2000).
It emerges from the scoping review carried out on the subject and the case studies that, depending on the country, the autonomy and independence of mutuals and CBHI are not necessarily a defining element in all national contexts, particularly in Ghana, Rwanda and the United Republic of Tanzania. Similarly, with regard to the voluntary nature of membership, although the freedom to choose a mutual is sometimes mentioned, this does not mean that membership of an SHP scheme is voluntary. Several countries, such as Belgium, France and Morocco, combine compulsory SHP membership with the free choice of a mutual (Niang et al., 2023).
1.2 A wide range of mutual organizations emerging from diverse and dynamic historical processes
The case studies show that there are two main groups of mutual organizations, distinguishable by how they started, their founding objectives and their involvement in, and development within, the SHP system.
Mutuals originating from the world of work
A first group is composed of corporate or work-related mutuals, which originated as mutual benefit societies in industry or were set up by various organizations such as trade unions, professional associations, cooperatives, workers’ organizations in the informal economy, and agricultural organizations. Mutual societies thus appeared and spread widely in Europe during the nineteenth century, on the initiative of industrial workers and other socio-professional groups, with a view to collecting and pooling funds to protect themselves against social risks and to organizing safety nets for members (Grijpstra et al., 2011). In these countries, mutuals were already in existence and covered certain population groups before the introduction of social security schemes. The latter were then constructed from national traditions giving rise to a variety of models, including mutuals.
Box 4. The Belgian example
Mutuals in Belgium are social and solidarity economy organizations emerging from initiatives from different ideological worlds, which have retained their origins even though their religious or ideological references have lost some of their importance over time. The mutuals are grouped into five major unions:
-
Alliance nationale des mutualités chrétiennes (National Alliance of Christian Mutual Insurance Funds)
-
Union nationale des mutualités neutres (National Union of Non-denominational Mutual Insurance Funds)
-
Union nationale des mutualités socialistes (National Union of Socialist Mutual Insurance Funds)
-
Union nationale des mutualités libérales (National Union of Liberal Mutual Insurance Funds)
-
Union nationale des mutualités libres (National Union of Occupational Mutual Insurance Funds)
One of the special features of the Belgian health insurance system is the place and role of mutual societies. Unlike other countries, Belgian mutual societies are responsible for compulsory insurance.
In France, for example, the Morice Law of 9 April 1947, setting up the scheme for civil servants, delegated the management of compulsory health insurance for civil servants to mutuals. Subsequently, Law No. 48-1473 of 23 September 1948 entrusted management of the scheme for students to the Mutuelle des Etudiants, (Students’ Mutual, LMDE) as part of a public service delegation. In Belgium, the State supported the development of the mutual society movement from the nineteenth century onwards, before adopting a compulsory health insurance system for all salaried workers in 1944, with its management being entrusted to mutual societies. The role of mutuals diversified after the Second World War and the emergence of compulsory social protection systems, with mutuals being integrated to manage the compulsory scheme, for example in Belgium and Germany, or as part of a shared management arrangement with the State, as in France, or by offering complementary insurance to the basic scheme managed by the State, as in Spain.
Against this background, and within the meaning of the definition of mutuals in the codes on mutual societies in France and Belgium, mutuals are based on the principle of co-opting, between people who trust each other and who share a strong social capital. These mutuals generally develop a high level of management skills and are pools of expertise that have been put to good use in national systems aimed at extending SHP. Similar processes can be observed in other countries, for example in Japan with mutual aid associations, particularly for civil servants, teachers and seafarers (box 5). The European mutual society movement also played a key role in the development of mutuals in Latin America in the nineteenth century and in Africa with European colonization. This can be seen, for example, in the creation of mutuals within government departments and enterprises, such as the Mutuelle générale des fonctionnaires et agents de l’État de Côte d’Ivoire (General Mutual Fund of Civil Servants and State Agents of Côte d’Ivoire, MUGEF-CI) in Côte d'Ivoire, which was set up in 1973 and now has more than 740,000 beneficiaries. Since 2011, it has been operating as a delegated management organization (DMO) as part of UHC implementation, which has forced it to restructure to comply with Directive No. 07/2009/CM/UEMOA on social mutual schemes in order to benefit from the status of a DMO. In Morocco, the management of the compulsory health insurance scheme for public-sector employees and retirees, which came into force in 2005, has been entrusted to the Caisse nationale des organismes de la prévoyance sociale (National Social Insurance Societies Fund, CNOPS), which is a national union of eight public-sector mutuals created in 1950.
Box 5. Integration of mutuals into the National Health Insurance in Japan
Before the introduction of the National Health Insurance Act in 1958, there were mutuals in Japan set up by civil servants, seafarers and teachers. When national health insurance was introduced, the results of a survey showed that more than 90 per cent of people who had already joined a mutual wished to remain covered by it. Mutuals were integrated into the National Health Insurance with a mandate to cover specific population groups, including civil servants and private school staff. Their health benefits have been harmonized with all other schemes, although they can also offer supplementary cover. However, they set their own contribution rates. Mutuals receive state subsidies towards their operating costs.
Mutuals emerging due to external dynamics
More recently, since the 1990s, small-scale health insurance schemes have been promoted by national and international NGOs, donors and governments, as part of national UHC programmes (Mathauer et al., 2017), particularly on the African continent (box 6). These schemes are managed by, or more often with the participation of, communities and are referred to by the terms "community mutuals" or "community-based health insurance (CBHI)". They are particularly numerous in West Africa, where it is estimated that nine out of ten mutuals are small-scale organizations with fewer than 1,000 beneficiaries (Van Rompaey, 2013).
Box 6. Development of mutuals and community-based health insurance in Africa
In low-income countries, the development of SHP is recent, with the main impetus coming in the 1990s and 2000s. In West Africa, this development can be briefly summarized as three key phases of development (Letourmy, 2008):
-
A first phase, which dates back to the post-colonial era and schemes such as mutuals for the armed forces, came with the development of coverage mechanisms within the formal economy sector only, with very different approaches: compulsory public health insurance institutions (Rwandaise d'assurance-maladie, Rwandan Health Insurance, RAMA) in Rwanda, and the Fonds national d’assurance-maladie, National Health Insurance Fund, NHIF) in the United Republic of Tanzania); state healthcare provision for civil servants (budget allocations in Senegal); company medical schemes (Institutions de prévoyance maladie (IPM) in Senegal); setting up mutuals for civil servants and the armed forces (Côte d'Ivoire, Morocco, Senegal); direct employer responsibility (internal plans or contracts with private insurance companies in Burkina Faso); or the introduction of specific healthcare provision (Office de santé des travailleurs (OST) in Burkina Faso).
-
A second phase came in the 1990s and 2000s with the development of mutuals, CBHI and other microinsurance schemes for people in the informal and agricultural sectors. A wide range of schemes have emerged, both from local initiatives (NGOs, not-for-profit healthcare providers) or external initiatives (World Bank, ILO, international NGOs, European mutual societies, and so on).
-
The third phase developed from the momentum of global campaigns for national social protection floors, UHC and the 2030 Agenda. It is characterized by state involvement and the setting of health coverage policies that must cover all categories of the population and, very broadly speaking, merges the two previous phases. With this third phase, health insurance entered a phase of extension, albeit gradual and still insufficient, but very real. The case studies show that the national policies and strategies implemented in the various countries have developed progressively but differently, following pragmatic approaches and local or well-confined experiments; two major trends stand out (see below).
-
Some countries are developing a national SHP system that brings together all existing schemes in a single architecture to offer the same basic protection for all (examples Côte d'Ivoire and Ghana).
-
In other countries, the SHP system is fragmented, with a juxtaposition of schemes and programmes that divide the population into different categories, each with its own adapted scheme and cover (examples Mali, Rwanda, Senegal).
This dynamic can also be seen outside of Africa. In the Lao People’s Democratic Republic, for example, where a voluntary CBHI scheme has been set up under the supervision of the Ministry of Health to protect people in the informal economy, which accounts for 80 per cent of the total population. The scheme was launched as a pilot project in 2002 and gradually extended from 2006 with the support of external partners. In 2012, CBHI covered only 3 per cent of the total population, in 42 districts in nine provinces. From 2017, the CBHI approach was abandoned in favour of a non-contributory scheme managed by the national health insurance scheme and financed by resources from the national budget.
Similarly, in Cambodia, community mutuals were set up by NGOs across the country in the late 1990s to cover people in the informal economy and in rural areas. They were extended until 2012; however, they only ever reached 3 per cent of the total target population, before experiencing a decline and ceasing to exist after 2018. These mutuals provided the country with first-hand experience to enable the setting up of a national health insurance scheme. This currently covers only workers in the formal sector, but with the aim of gradually extending it to the entire population.
Classification
An important lesson can be drawn from the case studies on the capacity of mutuals to act as delegated managers. A clear distinction needs to be made between the different types of organizations commonly referred to as mutuals or CBHI, based in particular on their professionalization.
-
Professionalized mutuals : Often corporate in nature, they may originate from a variety of organizations such as trade unions, professional associations, cooperatives, workers’ organizations in the informal economy, and agricultural organizations. In this context, and within the meaning of the codes on mutual societies in Belgium or France, these entities are based on the fundamental principle of co-opting, between people who trust each other and who share a strong social capital. The case studies show that the expertise developed by professionalized mutuals is not made use of in many West African contexts. Yet they are pools of expertise that could be put to good use in national systems aimed at the extension of SHP. -
Community mutuals : Community mutuals and CBHI are generally set up through external financing, supported or not by national programmes, on the basis of geographical or administrative areas (village, commune, district, and so on). However, neither trust and social capital nor technical skills in social protection management arise spontaneously from this type of planning (Sossa, 2010). The promotion of community mutuals is often part of a programme approach, with no legislation guaranteeing beneficiaries a right to SHP, nor a regulatory framework guaranteeing adequate oversight to protect beneficiaries. They are therefore often developed in isolation, and their weakness in terms of management limits the potential for delegation of management by a public body responsible for SHP. -
Parastatal bodies commonly referred to as mutuals or CBHI : In a number of countries, the term mutual or CBHI actually refers to decentralized administrative branches forming part of the public or parastatal sector. As explained in the following section, this may be the result of an absorption of the mutual society bodies that preceded the creation of the national SHP system (for example, in Cambodia or the Lao People’s Democratic Republic), or of the architecture of the national SHP system seeking to highlight a certain participatory aspect by using this terminology.
It is therefore important not to underplay the mutual society movement or drown it in a mass of organizations if the aim is to use its social and management capital as a lever for extending social protection.
Overview of the role of mutuals and community-based health insurance in social health protection systems
Key messages
-
Few countries in the world use mutuals in their SHP system for base cover, and the role of mutuals is more often confined to complementary coverage.
-
There is a diverse range of mutuals and of SHP systems themselves, limiting comparability and opportunities for making them widespread. The characteristics of these entities (mutuals/CBHI) are also influenced by the role they play in the SHP system.
-
The experiences that have been successful in extension terms are those in which:
-
from the outset, there has been a centralized SHP model with community mechanisms/branches forming an integral part of the public service;
-
there has been absorption into the national SHP institution;
-
there has been delegation of management by the SHP scheme;
-
where mutuals or CBHI have developed outside these schemes, they have not extended base cover; and
-
there are cases that are not yet in these categories because the systems are under construction or in the process of reform.
-
-
More research and documentation is needed on the delegation of management in particular and the practical arrangements for its implementation, its legal framework and its impact.
2.1. A role primarily focused on complementary and supplementary cover at the global level
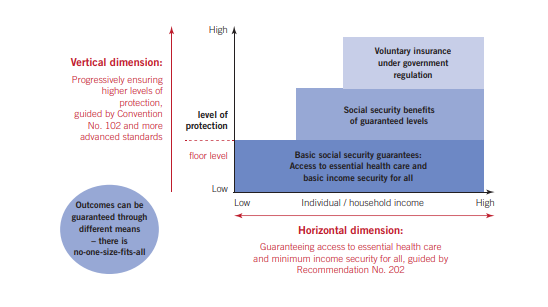
As illustrated in figure 2 below, mutual benefit societies are not found in every country in the world. Moreover, in most countries their role is limited to providing complementary or supplementary cover to the basic scheme, leading to few countries using mutuals in their SHP system for base cover.
Figure 2. Global map of members/policyholders of mutual insurers (2017)
Source: International Cooperative and Mutual Insurance Federation (ICMIF), 2019 2
2.2. The role given to mutuals and community-based health insurance in national social health insurance systems using them for their basic scheme
By studying the information available on the role played by mutuals and CBHI in national SHP systems for the basic scheme, a classification emerges, summarized in table 1, which may also in some cases be a situation that is continuously and dynamically evolving over time (some countries may, in time, be in one or more of the categories below).
Table
|
Delegation of management |
The management organization responsible for public insurance delegates certain management functions to autonomous mutuals for the implementation of base cover for their members. This is generally the case in countries where highly professionalized mutuals predated the SHP scheme. In some cases, the State entrusts the implementation of public insurance to different stakeholders, including mutuals, each covering different target groups of the population. |
France, Belgium, Morocco, Côte d’Ivoire, Uruguay, Colombia, Germany and Japan. |
|
Decentralization |
The SHP system was designed on the principle of setting up decentralized, participative bodies to manage local functions. The entities known as "mutuals" or CBHI are state or parastatal entities and operate as the branches of a national programme. They have only limited autonomy. |
United Republic of Tanzania, Senegal (under departmental health insurance units (UDAM)) and Ethiopia. |
|
Absorption |
When it was set up or reformed, the national SHP system absorbed the pre-existing mutuals or CBHI, thus benefiting from the tools and in some cases even qualified staff. |
Lao People’s Democratic Republic, Cambodia, Rwanda and Ghana after 2003. |
|
Non-involvement |
Mutuals provide base cover where there is not yet a national SHP system setting out the rights for the entire population. In these schemes, mutuals generally benefit from a legal status and framework for their regulation, and act as voluntary mechanisms responsible for all insurance functions. |
Burkina Faso, Senegal and Mali before the recent reforms. |
Delegation of management to autonomous mutuals
Delegation of management to professionalized mutuals that predate the national SHP system is another strategy observed in several countries, including Belgium, Colombia, Côte d'Ivoire, France, Mali, Morocco and Uruguay. In these systems, the State gives a national health insurance fund the task of implementing the insurance scheme and chooses to delegate certain tasks to a limited number of organizations such as mutuals or private insurers. The delegation of certain functions to mutuals is often the result of a process based on historical considerations and aimed at preserving a tradition of mutual organizations rooted in certain socio-professional groups.
The aim of delegating management is to transfer some or all of the responsibilities and tasks linked to management to a third party. This outsourcing is often accompanied by a delegation of the decision-making power associated with these responsibilities and tasks. Mutuals are required to meet certain conditions in order to become delegated managers of compulsory health insurance, particularly in terms of volume of beneficiaries and technical and financial capacity. They have little or no autonomy over the scheme’s parameters, and the tasks delegated are limited and highly regulated.
Box
This is the case in point in Belgium, where general health insurance administration is undertaken by the Institut national d’assurance-maladie-invalidité (National Institute for Health and Disability Insurance, INAMI), with management delegated to the unions of mutual benefit societies, which in turn delegate some of their functions to their member mutual benefit societies. In Morocco, the compulsory health insurance scheme for civil servants (assurance-maladie obligatoire, AMO-public) is managed by the CNOPS, which is a federation of eight mutuals that act as delegated managers. As a result of failings, the CNOPS is in the process of being replaced by the Caisse marocaine de l’assurance-maladie (Moroccan Health Insurance Fund, CMAM), with mutuals remaining delegated managers.
In Côte d'Ivoire, health insurance is managed by the Caisse nationale d’assurance-maladie (National Health Insurance Fund, CNAM), which was initially designed as a simple governance and regulatory structure for universal health cover. The CNAM delegates the functions of registration, collection and benefits to various stakeholders with previous experience, including the MUGEF-CI. The strategy for extending health cover to the informal economy is based on delegating management to mutuals, but the CNAM is developing at a slow pace. Côte d'Ivoire is therefore seeking to encourage the creation of mutuals, organized more by type of trade or sector of activity, which could act both as delegates of the CNAM and as complementary cover for insured persons.
The same trend can also be observed in Mali, where the State is seeking to bring its universal health insurance scheme into operation. The scheme is to be administered at the national level by the Caisse nationale d'assurance maladie (National Health Insurance Fund, CANAM), with management delegated to public funds for the formal sector and to the Union de la mutualité malienne (Malian Mutual Union) for informal sector households and the farming community. While waiting for this scheme to come into operation, cover for the latter will be provided by developing mutuals, including mutuals that in several respects (parameters defined as part of the National Strategy for the Extension of Health Coverage) are more akin to CBHI than to mutual insurance.
The system in place in Colombia is also part of this group. The State, through the Ministry of Health and Social Protection, has the role of steering the SHP system and defines its parameters. The collection of contributions and the purchase of benefits are delegated to health promotion entities (Entidades promotoras de salud - EPS); the contributions are paid and pooled at the level of the Entidad administradora de los recursos del sistema general de seguridad social en salud (ADRES), attached to the Ministry of Health and Social Protection, which redistributes them to the EPS according to the number of beneficiaries (capitation).
Some national schemes do not depend on the creation of a health insurance management organization centralizing the operation of the insurance scheme at the national level by choosing, or not, to delegate some functions to other actors. In these schemes, the management of the basic scheme is entrusted to different types of actors, including social security funds, company funds, trade guilds and mutuals, tasked with covering certain population groups. These actors enjoy a high degree of autonomy within a legal framework set by the State, which plays a regulatory role. This model allows the State to influence the development of the SHP system, while freeing itself from direct administration and relying on the expertise of the management organizations.
Germany illustrates this model with a public insurance system decentralized since its creation. The management of public health insurance is entrusted to a variety of decentralized insurance funds with complete management autonomy, a large proportion of which are governed by mutual societies. However, the system is now increasingly regulated by the federal government and the number of funds has fallen sharply (from 35,000 at the end of the nineteenth century to 105 in 2022). Similarly, in Japan, 85 mutual aid associations manage compulsory health insurance for national and local public employees, teachers and private school staff. These mutuals offer the same benefits as other compulsory health insurance schemes, but set their own contribution rates based on their yearly expenditure.
Some countries classified here in other categories are also part of this decentralization model, such as Rwanda, which illustrates the absorption of mutuals by the Rwandan Social Security Office. However, the latter does not cover the entire population, and other systems are in place for the military, students and private enterprises. Morocco is another example, with the various economic social groups managed by three major stakeholders: the CNOPS (public-sector employees and students), the Caisse nationale de sécurité Sociale (CNSS) (private-sector employees and the self-employed) and the Agence nationale de l’assurance-maladie (National Health Insurance Agency, ANAM) (poorest members of the population). However, Morocco is classified here under delegated management schemes providing cover for public-sector employees and retirees.
Mutuals as decentralized structures of an SHP system
The experience of community mutuals has inspired some countries to adopt this approach as part of national CBHI programmes. The aim of these programmes is to roll out a geographically close network of services to all communities throughout the country, such as in the Lao People’s Democratic Republic (where CBHI was set up by the government, with the support of external partners), Senegal's Décentralisation de l’assurance-maladie (Decentralization of Health Insurance, DECAM) programme and Ethiopia's Health Extension Programme (HEP). Other examples include Rwanda and Ghana, before the mutuals were absorbed and merged into the national health insurance system. This aim can be summed up in the slogan for the DECAM project: "One local community, at least one mutual". In this context, the term mutual or CBHI actually refers to decentralized administrative branches forming part of the state or parastatal sector, with a certain degree of community participation.
This scheme may include two levels of intervention by mutuals or CBHI:
-
Mutuals are simply branches limited to carrying out procedures defined at the national level.
-
Mutuals are able to offer complementary cover or other services to their members, thereby retaining a degree of autonomy.
Box
The aim of decentralizing health insurance by setting up community mutuals throughout the country is to reach all sections of the population through local structures. The experiences of countries such as Ethiopia, Ghana, the Lao People’s Democratic Republic and Senegal shows that this deployment is also the main weakness of this approach.
In the various countries concerned, these approaches have been built on promising initial experiences taking place on a small scale, but their success has been undermined as CBHI was rolled out and made more widespread. This led to the dispersal of community mutuals and the inability of the national promoter to ensure quality coordination, oversight and technical support, and to provide training in the skills needed as the system was extended. As a result, many challenges have arisen in CBHI. They are listed below.
-
lack of human resources and motivation of management committee members working on a voluntary basis in addition to their other professional duties
-
lack of budget and operating resources
-
lack of awareness-raising and communications campaigns
-
failings in the registration and renewal of memberships, the updating of information on policyholder cards, contribution deposits, and so on
-
inaccuracy or non-compliance with management procedures and national guidelines
-
poor governance in some CBHI, non-compliance with national guidelines and corrupt practices in the management of healthcare claims
-
inadequate implementation of fraud control measures, adverse selection and prevention of benefit cost overruns
-
lack of cooperation from healthcare providers (non-compliance with drug lists and tariffs, over-billing, fictitious, erroneous or overcharged services, excessively long deadlines for submitting claims, and so on)
These difficulties tend to discourage new memberships and renewals, or to encourage households to renew their membership only when there is a known need to use health services (elective surgery, an individual at high risk of illness in a household, and so on), which generates a risk of adverse selection and leads to financial problems for health insurance, exacerbated by poor risk pooling.
Absorption
One scenario observed in the case studies is the absorption of mutuals by the SHP system. This situation can be seen in Cambodia, the Lao People’s Democratic Republic and Rwanda after 2014, and Ghana after 2003, where the mutuals promoted under national programmes were dissolved and replaced by branches or other decentralized structures responsible for local services and governance. This approach is generally justified by the desire to improve the efficiency, rationalization and harmonization of population coverage.
In Rwanda, for example, the administration of CBHI was taken over and centralized by the Rwanda Social Security Board (RSSB) from 2015. Staff from community mutuals were integrated into the RSSB to represent insurance at branches set up in health facilities. Similarly, in Ghana, most of the 145 district mutuals that operated as independent schemes have been integrated into a single national health insurance system since 2012, becoming district offices under the technical and financial management of the National Health Insurance Authority (NHIA). In Cambodia, CBHI schemes, generally supported or even managed by an international or local NGO, were dissolved after 2018 and coverage integrated into the SHP schemes currently in operation managed by the National Social Security Fund (NSSF). This is also the case in the Lao People’s Democratic Republic, where the CBHI scheme has been replaced by a tax-based "national health insurance", with no prepayment required but payment of a reduced amount when health services are used; CBHI continues to exist in the capital, however. The pattern is more mixed in the United Republic of Tanzania, where the management of CBHI has been taken over by the NHIF, which is developing improved CBHI (improved Community Health Fund - iCHF) and continues to belong to the districts and regions, but with technical management provided by the NHIF.
In France, a return to the delegation of management to the historical mutual societies for students and civil servants has led to the closure of some mutuals. Others have stopped participating in the management of the compulsory scheme and are now focusing on complementary cover. The health insurance fund has also proposed new types of partnership to the civil service mutuals, based in particular on shared management and the use of the same information system.
Mutuals in the absence of a basic public insurance scheme
At the global level, the role of mutuals is limited in most countries to providing complementary or supplementary cover to the basic scheme, meaning that few countries are using mutuals in their SHP system for base cover (including the case study countries).
In other countries, the absence of SHP, which sets out the rights of the entire population in terms of a healthcare package and financial protection, has been at the root of the creation and development of mutual societies within the world of work, particularly in Europe. More recently, in countries such as Burkina Faso, Cambodia, Mali and Senegal, prior to recent reforms and the construction of national SHP schemes, this has led to the promotion of mutual societies by NGOs or external partners with a view to offering basic protection to communities, generally identified on the basis of geographical or administrative area (village, commune, district, and so on). Thus, these community mutuals are generally set up as a result of external initiatives and under a project approach, with no legislation guaranteeing beneficiaries a right to SHP, and so often developing in isolation. They are generally rolled out by replicating a successful initial experience, through a support structure that defines the technical parameters of the insurance and remains heavily involved in the management of the mutuals for the duration of the projects. An inventory of mutuals in Burkina Faso in 2020 showed that mutuals set up under projects undertaken by national NGOs and financed by donors and backers were no longer in operation after the projects ended, due to a lack of follow-up by the NGOs (Burkina Faso, 2022). The same situation can be observed in Cambodia, where CBHI systems were built on a similar organizational and operational model and were managed by NGOs with the support of development partners. These systems began to decrease in number from 2014 and then stopped in 2018, following the withdrawal of support projects.
In the various countries, any successes of the initial small-scale experiences were quickly eroded when they were rolled out nationwide, and a number of challenges were identified through the case studies, including in terms of governance, human, material and financial capacities, efficiency of procedures, and cooperation with service providers, in addition to the inability of the support structures to ensure quality coordination, oversight and technical support as the system was extended. These challenges are similar to those detailed in box 8 on decentralized structures.
Box
Latin American countries addressed the issue of extending social protection in the 1970s. In Africa, the issue began to be addressed through marginal projects in the early 1990s, with the development of community-based systems combining traditional mutual aid practices and insurance mechanisms to cover the risk of illness. These initiatives multiplied in the 2000s, promoted by a wide range of stakeholders, in order to meet the priority needs of populations excluded from formal social security schemes. The vision widely shared by all stakeholders at the time was that the proliferation of mutual health insurance projects should ultimately lead to cover for all.
A number of lessons can be drawn from this process of developing community mutuals. Various innovative approaches have been developed and some mutuals have demonstrated their ability to reach a significant proportion of individuals at community or organization level (for example, cotton producers in Benin and Burkina Faso), with good results in terms of the financial protection provided and the impact on the use of health services. These experiences have also made a major contribution to popularizing insurance mechanisms among people in the informal economy and rural areas.
However, despite locally successful experiences, the systems put in place cover only a small proportion of these populations overall, have weak management capacity and remain financially very fragile. Overall, the systems set up by support organizations and external funding under project approaches are not capable of instilling trust and mobilizing social capital or technical skills in social protection management (Sossa, 2010).
In addition, these experiences have generally promoted a vertical vision of social protection, with compartmentalized responses for each population group, separating systems for the poorest people, workers in the informal economy and rural areas, and those in the formal sector, with no cross-cutting solidarity mechanisms.
Type of functions performed
Some functions seem to be delegated more than others and/or with greater success. In particular, in all the delegation experiences the accredited mutuals were given local responsibilities, in other words, management of registration, sometimes the collection of contributions, management of beneficiaries, local governance, and management of reimbursements/payments to healthcare providers.
The brief summary compilation presented in the table below does not reflect all the variations observed in the case studies. It does, however, identify a general trend: the main advantage sought in the delegation of management is to make use of the proximity of mutuals to certain population groups. This is particularly so in situations where the vast majority of individuals are involved in the informal economy and agriculture, with all the attendant complexity in terms of identification, contributory capacity and collection. The role assigned to community mutuals in CBHI promotion programmes is significant in this respect. Community mutuals are developed as local and participatory management mechanisms, intended to serve as a gateway to SHP and as points of service for a highly heterogeneous and dispersed population. In other countries, where the formal economy is more widely developed and individuals are more easily identifiable through the employment relationship and tax framework, the choice of delegation is also based on the proximity of mutuals to certain target groups, but is justified more by a political will to preserve the historical role of pre-existing mutuals, or even the benefits acquired by the socio-professional groups at the root of these mutuals.
In contrast, the situations seem more varied for decision-making functions concerning the parameters of coverage, the pooling of resources, risk sharing, financing (including contribution rates, if applicable), and relations with healthcare providers at the national level (contracting, tariff negotiations). In several countries, these functions are centralized and seen as the prerogative and duty of public bodies
Table
|
|
Decision on coverage parameters |
Implementation |
||||||||||
|
|
Population coverage |
Healthcare package |
Level of financial protection |
Healthcare provider network |
Information and promotion |
Membership |
Contribution collection (if applicable) |
Contracts with healthcare providers |
Payment of benefits |
Provision of healthcare services |
Quality control |
Complaints mechanisms |
|
Belgium |
|
|
|
|
X |
X |
X |
X |
X |
X |
|
|
|
Burkina Faso |
|
|
|
|
X |
X |
|
X |
X |
|
|
|
|
Cambodia before 2018 |
|
|
|
|
X |
X |
X |
X |
X |
|
X |
|
|
Colombia |
|
|
|
X |
X |
X |
|
|
|
X |
|
|
|
Côte d’Ivoire (1) |
|
|
|
|
|
X |
X |
|
X |
|
|
|
|
Ethiopia |
|
|
|
|
X |
X |
X |
X |
X |
|
|
|
|
France |
|
|
|
|
X |
X |
|
|
X |
|
|
|
|
Germany |
X |
X |
X |
X |
X |
|||||||
|
Ghana |
|
|
|
|
X |
X |
X |
X |
X |
|
|
|
|
Japan |
|
|
|
|
|
X |
X |
|
|
|
|
X |
|
Lao People’s Democratic Republic |
|
|
|
|
X |
X |
X |
X |
X |
|
|
|
|
Mali (1) |
|
|
|
|
X |
|
X |
|
X |
|
|
|
|
Morocco |
|
|
|
|
X |
X |
X |
X |
X |
|
|
|
|
Rwanda |
|
|
|
|
X |
X |
X |
X |
X |
|
|
|
|
Senegal |
|
|
|
|
X |
X |
X |
X |
X |
|
|
|
|
United Republic of Tanzania |
|
X |
|
|
X |
X |
X |
X |
X |
|
|
|
|
Uruguay |
|
|
|
X |
X |
X |
|
|
|
X |
|
|
-
Functions delegated to DMOs, including mutuals
Thus, a division of functions between the public bodies responsible for SHP and the delegated mutuals can be observed:
-
The public bodies responsible for SHP retain a number of key “back office” functions:
-
In all countries, the coverage parameters (healthcare packages, reimbursement rates, contribution rates, and so on) are defined at the national level and are imposed on the delegated mutuals. As noted in the table, mutuals in some countries (Cambodia, Ethiopia and Ghana) can set or adjust contribution rates.
-
Healthcare providers are generally identified at the national level, as part of a concerted national accreditation and agreement process, with or without the participation of mutuals.
-
Except in the case of CBHI, risks and resources are pooled at regional or national levels.
-
The monitoring and steering of the SHP system and the performance of delegated tasks are carried out at the national level, by the delegator or by a public body designated for that purpose.
-
-
The activities delegated to mutuals primarily concern the insurance business directly linked to insured persons and healthcare providers, known as “front office” functions:
-
Registering and managing memberships, including poor households exempt from paying contributions, with the support of the administrative, traditional and religious authorities and sometimes door-to-door collection agents, in the case of CBHI.
-
Collection of contributions. France and Belgium stand out for having set up social security bodies dedicated to contribution collection.
-
The collection and handling of user complaints is often the responsibility of the delegated mutual, but some countries have set up a specific regional or national mechanism.
-
It should also be noted that some functions are carried out jointly. Table 3 summarizes examples of divisions of operations taken from the case studies.
Table
|
Education/Promotion |
|
|
Function of mutuals |
Function of the management organization |
|
In Belgium, mutuals are in close proximity to their members through their local mutual society branches and offices, and organize information and health promotion activities, to which they attach high importance. In Burkina Faso and Cambodia, the NGOs responsible for implementing the community mutuals work with them on promotion and education activities. In the United Republic of Tanzania and Senegal, mutuals carry out promotion activities with the national agencies that support them. In Colombia and Uruguay, mutuals are required to carry out promotion and prevention activities for members, such as information, education, training and communications. In the Cambodia example, some systems set up networks of agents who make door-to-door visits and organize village meetings. |
In most countries, insurance management organizations, ministries or other public agencies run national campaigns jointly with mutuals. |
|
Membership/renewal |
|
|
Function of mutuals |
Function of the management organization |
|
In all countries, delegated mutuals are in charge of the enrolment and membership of insured persons and beneficiaries. In Côte d'Ivoire, delegated structures are specifically designated for this function. In Uruguay, beneficiaries register with public or private healthcare providers. |
In Morocco, the CNOPS, in coordination with mutuals, handles employer enrolment, registration and membership and updates the administrative status of insured persons. In Mali and Côte d'Ivoire, the final registration of enrolments is undertaken by the national fund. In Côte d'Ivoire, the fund has deployed a computerized network of terminals and enrolment sites throughout the country, which handle registration, enrolment and the issuance of policyholder cards, to make up for the lack of delegated structures. |
|
Recovery/collection of contributions |
|
|
Function of mutuals |
Function of the management organization |
|
In most countries, contributions are collected by mutuals or dedicated delegated bodies, as in Côte d'Ivoire. In some countries, contributions are paid to the management organization. |
In Belgium and France, contributions are collected by administrative bodies responsible for social security funds. In Uruguay, contributions from worker and employer members of the contributory scheme are collected by the Social Security Bank. In Morocco, contributions for civil servants (employer and worker parts) are paid to the CNOPS. |
|
Pooling |
|
|
Function of mutuals |
Function of the management organization |
|
In Senegal and Rwanda (before 2015), member contributions are kept at the level of community mutuals (low level of pooling). State subsidies, which complement these contributions, are pooled at regional and national levels to cover secondary and tertiary care. In Japan, resources and risks are pooled at mutual society level. |
In all other countries, resources are pooled at the level of a public body or a federative structure to which the mutuals pay the contributions collected. These bodies redistribute resources and pool risks at regional or national level. |
|
Contracts |
|
|
Function of mutuals |
Function of the management organization |
|
In CBHI programmes, mutuals sign agreements with the (mainly public) healthcare providers in their area of intervention, often on the basis of a standard agreement provided by the national agency. In Colombia, Health Promotion Enterprises (EPS) have contracts with service providers. |
In other countries, agreements or approvals are signed by the insurance management organization or by the ministry responsible for health. |
|
Payment for services/purchases |
|
|
Function of mutuals |
Function of the management organization |
|
In CBHI programmes, mutuals act as purchasers, on a fee-for-service or capitation basis, as in the case of the EPS in Colombia. In Japan, providers' invoices are sent to the "Healthcare bill check and payment organization”, which pays them and then charges the mutuals concerned. |
In other countries, mutuals oversee benefits and arrange reimbursements to healthcare providers; payments are made by the national management body (or by the regional federations in Germany). In France, mutuals paid service providers and were then reimbursed by the health insurance fund. |
|
Service provision |
|
|
Mutuals providing health services |
No health services |
|
In Germany, France, Belgium and Japan, mutuals can provide health and support services through the health facilities they manage. In Morocco, the law prohibits mutuals from managing health services; some mutuals with medical units have created autonomous mutual society structures to manage them. |
Mutuals in other countries do not manage health services. |
|
Feedback/user complaints/quality assurance |
|
|
Mutuals |
Other |
|
In France, delegated mutuals were in charge of service quality, but with serious shortcomings. In Japan, there is no official harmonized complaint system, so users go through their mutual. Members of community mutuals can complain to their representatives on the management bodies (General Assembly and Governing Body). |
In Germany, a medical service is responsible in each region for overseeing the adequacy of healthcare and appeals by insured persons against fund decisions. The medical service is also involved in an internal certification and quality assurance process. In Colombia, organizations attached to the Ministry of Health receive complaints from users and oversee service quality. |
The last part of this working paper looks more closely specifically at the delegation of management as a model of interest in the context of SHP reforms in West Africa.
Two lessons emerge from the scoping review and the in-depth case studies. Where management delegation has taken place and has been (or still is) functioning effectively:
-
It mainly concerns front office functions, while back office functions (design of scheme parameters, pooling of funds and risks) remain a public function.
-
This has been made possible thanks to the professionalization of actors and the clear architecture of the SHP system, with public funding and compulsory membership.
The delegation of management: Lessons learned and prospects for constructing social health protection systems within the West African Economic and Monetary Union
Key messages:
-
Where they already exist and have management capacity, mutuals can be seen as a potential actor to be mobilized by national SHP systems.
-
This should be accompanied by the definition of a clear SHP architecture, adequate public funding and strengthened institutional capacity on the government/institutional side so as to be able to manage the pooling of funds and risks functions.
-
The delegation of management requires the delegated bodies to have management skills; it will therefore be necessary to understand the diversity of mutuals and to identify the organizations able to carry out the delegated functions.
-
It is important to consider the political economy and its challenges: (i) the role of technical and financial partners (TFPs); (ii) models as sources of inspiration; and (iii) issues of trust in public institutions and the democratic deficit in the governance of health and SHP.
3.1. Objectives and results
Delegation of management concept
The scoping review and research undertaken for this working paper identified that there was no single definition of delegation of management in the context of SHP. However, there are some common elements to the experiences identified. The delegation of management is a possible implementation strategy for the bodies responsible for SHP. The aim is to transfer some, or all, of the management responsibilities and tasks to a third party. This outsourcing is often accompanied by a delegation of the decision-making power associated with these responsibilities and tasks. It is very common in the private insurance sector (box 10), but also exists in the public sector.
Box
According to its technical definition (1), the delegation of insurance management consists of a health insurance management organization (health insurance fund, mutual benefit society, private insurance company, and so on), called the delegator, which entrusts implementation of all or part of the management functions of insurance operations to a third party, known as the delegated body, which will carry out its tasks autonomously using its own human, material and financial resources. The delegated body may, in particular, be another insurance organization (mutual, commercial insurance) or a specialist management arm for insurance accounts, or even a brokerage company, a management centre or an economic interest group. It must have the technological, information technology (IT) and logistical infrastructures, as well as specialized human resources, to guarantee quality of service for the functions entrusted to it. Furthermore, it is not just another service provider, because it acts on behalf of the delegator and must therefore be very familiar with the latter, as well as its objectives and methods of action.
It should also be noted that the delegation of management is distinct from two other concepts:
-
The delegation of functions, which involves the transfer of specific tasks or responsibilities to a person or department within an organization;
-
The delegation of public service, which is a contract by which a public legal entity entrusts the management of a public service (management of a health facility, waste collection, and so on) to a private or public legal entity. In this case, the delegated legal entity must take on the responsibilities and obligations associated with management of the public service, such as the obligation to ensure continuity of service, quality of service, transparency and public safety (2).
(1) This definition is taken from the online resources of consulting firms and companies specializing in the delegation of health contract management (notably Optimind and Hélium).
The delegation of management is a common practice in the field of private commercial insurance. It also occurs in the context of public health insurance systems; as highlighted above, it has been observed, at least at certain points in the evolution of SHP systems, in several of the countries covered in the case studies, including Belgium, Colombia, France, Japan, Morocco and Uruguay, as well as in some mutuals in Ghana.
In West Africa, this is also the case in Côte d'Ivoire and Mali, where public insurance functions are transferred to delegated bodies, including mutuals. Delegated management is also provided for in Law No. 060-2015/CNT on the universal health insurance scheme in Burkina Faso. Senegal, on the other hand, has opted for decentralized insurance management, entrusted to community health mutuals and their district and regional unions.
Against this background, where the potential for mobilizing community actors is scarcely being realized and where the implementation of UHC policies still remains the subject of much debate, delegated management experiences are recent and still poorly documented. The purpose of this paper is to examine the lessons that can be drawn from case studies of delegated management experiences with a view to fuelling the debate on the architectures leading to coverage of the entire population, including households dependent on the informal and rural economy, within the WAEMU.
Initial objectives
The expectations for outsourcing insurance management functions can be summarized in three main points, as identified in the case studies and available literature:
-
Whatever its construction process, the management of functions within a national SHP system is complex. It requires a wide range of expertise and skills to be put in place (legal, technical, commercial, soft, organizational, digital, and so on). An SHP management body may therefore choose to entrust certain operational or administrative tasks to specialist third parties with a comparative advantage (Tessi, 2022). However, these advantages may be outweighed by disadvantages, including the loss of certain expertise and a risk of the delegator becoming dependent on the delegated body or of failures by the latter.
-
The outsourcing of some functions provides greater flexibility in the face of the constant need to adapt to the many environmental changes (political, regulatory, societal, technological, demographic, economic, and so on) that are transforming the organization of business activities, trades and occupations, and skill profiles. This means, however, that the delegated bodies must also have the ability to adapt to these changes.
-
Public SHP systems should have distribution channels, as a national system needs to be adapted to the specificities of different population categories, which is often a challenge, especially in low-income countries. Some population groups may be further removed from the institutional and administrative environment deployed by the public sector, in particular people living in rural areas, workers in the informal economy and their families, migrant or displaced populations, or population groups suffering discrimination. This physical and/or legal distance between the public bodies in charge of SHP (and social protection and social services in general) may justify the use of private organizations (often not-for-profit) to create a link with the target populations, such as associations, cooperatives and mutuals. For example, by delegating the management of membership and collections to a network of mutuals or other community-based organizations, a national health insurance fund avoids having to make major efforts to reach people in the informal economy and rural areas where these organizations are already present. An example of this is the delegation contract between the CANAM and the Union technique de la mutualité malienne (Mutual Societies Technical Union of Mali, UTM) (box 11). Beyond these points, the main objective of a national system based on coordination between various mechanisms, through a delegation of management, should be to build a unified national system offering cover to all categories of the population, bearing in mind that achieving universal coverage depends on the ability of national stakeholders to coordinate different measures, including compulsory or automatic enrolment (or incentives for voluntary schemes), extended risk pooling, tax-based financing for the poorest households, proximity and simplification of procedures for the insured persons.
Box
The reform of the national SHP system launched in Mali in 2015 aims to bring together the mechanisms put in place in the 2000s, to offer the entire Malian population a universal health insurance scheme (Régime d’assurance-maladie universel (RAMU)) that will cover all social categories through the most appropriate mechanisms.
To achieve this objective, the reform entrusts the management of the RAMU to the CANAM. Under this new arrangement, the CANAM delegates some of its responsibilities to DMOs, including mutual benefit societies, through a contract with the UTM) or other mutual insurance umbrella organizations, for the agricultural and informal sectors, as well as beneficiaries of the Régime d’assistance médicale (Medical Assistance Programme, RAMED). The UTM has a network of rural community mutuals and inter-professional mutuals in urban and semi-urban areas.
As highlighted above, the inclusion of mutuals in national SHP systems, as delegated managers, is based on their a priori added value, including:
-
their social roots and their proximity to certain population groups. In countries where the major portion of the population makes up the informal economy and agricultural community and where the direct relationship between these groups and the government is hindered by a lack of trust, owing to the State’s poor performance in service provision in various areas, mutuals play a key intermediary role;
-
their ability to adapt and simplify often complex, tedious and time-consuming administrative procedures, which discourages people from joining social security schemes. For informal workers, the cost in terms of time due to inefficient systems and administrative obstacles is a barrier to accessing social protection systems;
-
that, in addition to trust, their proximity gives them a potentially major role in promotion and prevention. In France, this is reflected in health education and increased patient participation in health bodies, activities to combat smoking or obesity, or preventive activities on road safety, working conditions, screening and oral health. In Belgium, mutual societies also attach particular importance to health information and education. Efforts in that direction include the signing, with the Minister of Social Affairs and Public Health, of a pact in 2016 for the future with insurance organizations, which strengthens their role in informing insured persons about the healthcare system and health in general, empowering patients and promoting healthy lifestyles.
Available documents do not allow for an analysis of the cost-effectiveness or efficiency of the different approaches to organizing the insurance business between management functions. Similarly, it is not possible to measure the impact of the delegation of management on reducing financial barriers to access to care and additional funding for care providers, compared with situations where mutuals intervene without being delegated bodies in an SHP system. This analysis is made all the more complex by the fact that other mechanisms have a direct impact on the level of cover of the population, especially the application of compulsory membership and resource mobilization within the budget to fund cover for the poor, and so on.
Results are not always in line with the initial objectives
The case studies show that the a priori attributes identified above are not fully exploited in some countries, due to weaknesses related to how the delegation of management is actually organized or the actors involved:
-
At the legal and regulatory framework level, Burkina Faso's experience of delegating cover for the poorest people to mutual societies illustrates the need to establish the status of DMOs. As mutual societies are not formally recognized by the government under WAEMU regulations, the Caisse nationale d’assurance-maladie universelle (National Universal Health Insurance Fund, CNAMU) ultimately delegated the management of healthcare for the poorest households to NGOs, which provide technical support to the mutuals but do not have a management role. In addition, not enough prior discussion took place, particularly on the nature of the functions delegated, the healthcare package covered and the steering mechanisms. Overall, the outsourcing strategy does not seem to have been understood in the same way by all actors.
-
The experience of Morocco highlights potential weaknesses in the way health insurance is managed. The CNOPS found itself in difficulties, split between three laws governing its status as a mutual benefit society and the compulsory health insurance schemes (régimes d’assurance-maladie obligatoire, AMO) for which it is responsible: the law on AMO-public and the law on AMO-student. The CNOPS failed to put in place certain regulatory provisions, in particular establishing budgets for each scheme. It also suffered from gaps in administration and management, with failings observed during its governing body meetings.
-
Mali’s case illustrates a major weakness linked to the failure of the delegated bodies, the l’Institut National de Prévoyance Sociale (National Institute of Social Security, INPS) and the Caisse Malienne de Sécurité Sociale (Malian Social Security Fund, CMSS), to meet their obligations, resulting in:
-
low involvement in the collection of insured persons’ files for registration (pre-registration);
-
partial repayment of contributions collected to the CANAM and failure to meet deadlines;
-
the lack of justification to the CANAM for the amounts received by the DMOs as part of operating grants; and
-
failure to comply with CANAM directives on the processing of treatment forms, particularly with regard to checking that care providers comply with agreed tariffs.
-
In France, the failings and high costs of the delegated management of the civil servant and student schemes led to the end of the delegation and the integration of the insured persons into the general scheme. The weaknesses identified concerned fragmentation of the SHP system, with multiple mutuals for civil servants and students, management costs higher than those of the general scheme, and a quality of service judged to be highly questionable in the case of student mutual societies.
3.2. Key stages and processes in the delegation of management: Prerequisites for and key elements of a management delegation process
Given the divergence between expectations and results observed in the case studies, the latter can also reveal a number of key elements contributing to the success of management delegation processes.
Definition of a clear national architecture for the SHP system
A first prerequisite is the definition of a clear and consensus-based architecture for the national health insurance system, aimed at giving effect to the right to SHP for the entire population and specifying the nature of the various mechanisms that make up the SHP system as well as the operational links between them. As the experiences of the various countries observed show, this architecture is the result of an ongoing process requiring each stakeholder, including mutuals, to have the capacity to innovate and adapt to the reforms.
To define an appropriate regulatory framework for mutual benefit societies and the delegation of management, aligned with the SHP regulatory framework
The lack of a clear definition and legal status for mutuals may act as a brake on the transfer of functions within an SHP system. The experience of Burkina Faso shows the inability of mutuals to intervene when their status is not clearly defined. In Côte d'Ivoire, the MUGEF-CI had to restructure to comply with Directive No. 07/2009/CM/UEMOA on social mutual schemes in order to qualify as a DMO.
The reforms guiding the process of changing the architecture of SHP systems in the various countries are set out in legislation that defines, at least in broad terms, the relationships between the different stakeholders, as illustrated in the following section. In France, for example, delegated management is governed by the Social Security Code, the Insurance Code and the Code on Mutual Benefit Societies. These legislative texts specify the terms of delegation, the respective obligations of the parties, and the applicable financial management and accounting rules. The legal framework also sets out a series of provisions relating to the protection of insured persons, particularly with regard to information, data confidentiality, claims management and continuity of service. In addition, some countries or groups of countries have introduced prudential rules that impose regulations on delegated managers (box 12).
Box
Although it concerns insurance and reinsurance undertakings, the European Solvency II Directive 3 illustrates the construction of a regulatory framework that imposes clear principles on the transfer of functions within the countries of the European Union:
-
Insurance management bodies remain fully responsible for discharging all of their obligations when they outsource functions or any insurance activities.
-
Insurance management bodies should refrain from delegating activities or outsourcing critical or important operational functions in such a way as to lead to:
-
materially impairing the quality of the system of governance of the undertaking concerned;
-
unduly increasing the operational risk;
-
impairing the ability of the supervisory authorities to monitor the compliance of the undertaking with its obligations; and
-
undermining continuous and satisfactory service (EU, 2015; Krajeski, 2019).
Contractual framework
The regulatory framework sets out in particular the form and content of the agreements between the delegator and the delegated bodies. This framework for the relationship between SHP management and the mutuals acting as delegated bodies is essential and includes:
-
-
the drawing up and strict application of clear, comprehensive and well-defined delegation agreements, with specifications setting out the rules of governance and indicators for monitoring delegated activities;
-
the establishment of operational fluidity and transparent, ongoing communication between the stakeholders. Ongoing dialogue must be established to allow for any adjustments required to the delegation agreement;
-
the establishment of a regulatory authority to arbitrate relations between those involved in the delegation of functions; and
-
the implementation of an effective system for monitoring delegated managers, supported by the production of transparent information and monitoring reports, with operational recommendations where necessary.
-
The contractual framework, however, is not well documented and you have to look to the commercial insurance sector, where the practice of delegated management is common, to find the broad outlines of a delegated management agreement, which includes the following points:
-
the scope of intervention and the roles and responsibilities of the delegator and the delegated body
-
governance and the setting up of bodies to provide regular updates on the carrying out of activities, implementation of the action plan, any difficulties encountered, and so on. This aspect is particularly important during the operational start-up phase of outsourcing activities, which may require adjustments
-
communication between the two parties to promote transparent and fluid communication, without waiting for steering committees to report failings, and to build a relationship of trust
-
regular and transparent reports that the delegated body must provide to the health insurer
-
securing the agreement so that the delegator is able to audit its delegated body. The insurance administrator must be able to identify and anticipate any failure or interruption in the delegated functions that would have a negative, or even catastrophic, impact on the health insurance business, particularly in terms of managing insured persons or processing reimbursements within reasonable time scales
This type of agreement can be found, for example, in the experience of the Régime social des indépendants (Social Security Scheme for the Self-Employed, RSI) in France (before its integration into the general scheme). The national fund in charge of managing the RSI concluded delegation agreements specifying the geographical scope of intervention of the "accredited organizations" (AOs). These agreements also set out additional conditions for these AOs:
-
To belong to one of the categories listed in Article L611-79 of the French Social Security Code, in other words: a mutual benefit society, an insurance company, a grouping of insurance companies or organizations covered by the Social Security Code.
-
To provide guarantees of their ability to fulfil the scheme's management obligations.
-
To have analytical accounting to identify expenditure relating to the management of the RSI health insurance scheme.
-
To have financial guarantees.
-
To have a reception facility in each of the districts where the AO is authorized to operate.
In another example, the CANAM in Mali signs a management agreement with each DMO involved in the operationalization of the RAMU. This agreement specifies the functions that are delegated, where required. It is accompanied by a contract of obligation and management protocols concluded between the CANAM and the DMOs, which set out the detailed duties and obligations of each party. In return for their obligations, the DMOs receive an administrative grant to cover operating costs and a technical grant to pay for services. Decree No. 10-580/PR-M of 26 October 2010 approving the standard management delegation agreement for compulsory health insurance provides a standard agreement. Management delegation is being tested by the CANAM in partnership with the INPS and the CMSS, within the compulsory health insurance framework. This delegation is to be extended to two new DMOs, the UTM and the Agence nationale d’assistance médicale (National Medical Assistance Agency, ANAM).
In Côte d'Ivoire, the CNAM requires insurance companies, commercial health management companies and mutual societies to develop expertise in technical management, so as to perform effectively and guarantee a lasting contractual relationship as a DMO with the CNAM. This compliance is part of a set of requirements to be met by DMOs, which include the following:
-
compliance by the DMO with the management standards in its category (Code of the Inter-African Conference on Insurance Markets, WAEMU community directives on social mutual schemes, Organization for the Harmonization of Business Law in Africa, and so on);
-
maintenance of a minimum number of beneficiaries to avoid the proliferation of small DMOs, which would result in an excessive workload, linked to the proliferation of DMO agreements to handle membership that the CNAM would have to manage; and
-
technical upgrades and integration into IT platforms and information and monitoring systems.
These constraints have resulted in the exclusion of mutual societies, which operate on a small scale in the informal and agricultural sectors and suffer from weak technical management.
A last example is Morocco, where Decree-Law No. 2-18-781 authorizes the CMAM to delegate some of its tasks to public-sector mutuals and to any public or private legal entity, in accordance with the conditions set out in an agreement approved by the governing body and based on a set of specifications concerning:
-
the nature of the benefits and the procedure for managing the reimbursement of guaranteed benefits
-
repayment terms
-
administrative and financial organization, geographical division, management costs and information and statistics relating to activities
-
procedures for carrying out administrative checks and audits and the conditions for accessing data
-
procedures for carrying out medical checks
-
the quality of services provided to insured persons
-
the information system and arrangements for managing sickness record archives; and
-
administrative sanctions in the event of failure to comply with the provisions of the agreements or the conditions of the requirements
Table
|
Delegator |
Delegated body |
|
|
Source: Codes on insurance, France
Oversight
In most countries, the activities of mutuals and other delegated bodies are supervised and overseen by:
-
a public body, such as the Office de contrôle des mutualités et des unions nationales de mutualités (Office for the Supervision of Mutual Societies and National Mutual Unions, OCM) in Belgium. In Morocco, the Agence nationale de l’assurance-maladie (National health insurance agency, ANAM) is responsible for regulating and supervising the compulsory health insurance scheme. In Senegal, the Agence de la couverture maladie universelle (Universal Health Coverage Agency, ACMU) oversees community mutuals and is also responsible for promoting them;
-
the supervisory ministry in Cambodia, Colombia, the Lao People’s Democratic Republic and Rwanda (before 2015);
-
the delegating health insurance management organization, for example in Burkina Faso, Côte d'Ivoire, France, Ghana and the United Republic of Tanzania;I
-
several entities, such as in Germany, where oversight of the legality and activities of the funds is divided between the federal level, the Länder and the municipalities, or in Ethiopia, where the Agence éthiopienne de l’assurance-maladie (Ethiopian Health Insurance Agency, EHIA) and the Federal Ministry of Health act as supervisory units for the CBHI.
The institutional and management capacities within the mutuals and the public bodies responsible for SHP are, of course, important factors in the success of health insurance systems. However, this is one of the main weaknesses of CBHI programmes. They generally begin with small-scale pilot schemes, on which substantial technical and financial support can be focused. Subsequently, as they scale up, the same support cannot be given to each new community mutual, given the human and financial resources that need to be deployed. For example, in Cambodia, the Ministry of Health did not have the capacity to implement controls or monitor the results of the mutuals. In Senegal, the deployment of a large number of community mutuals (676 mutuals plus their unions) raises the question of the capacity to provide sufficient technical support and to manage a particularly large flow of information. The national strategy is therefore to merge these community mutuals into departmental and regional mutuals in order to concentrate the management of health insurance and focus technical support on a limited number of entities.
3.3. Roles and responsibilities
The role of the State
The majority of countries are committed to formulating and implementing national strategies to extend health insurance cover and promote health, with a view to achieving universal coverage. In this context, the State has a dual responsibility:
-
The State sets out the legal framework for SHP: National strategies are based on international SHP standards, which are not prescriptive in terms of institutional and administrative arrangements, and each State is free to choose its own options for implementing basic guarantees, while ensuring observance of certain guiding principles, in particular the overall responsibility of the State (ILO, 2020b). As a result, the SHP systems architectures vary from country to country, in order to be acceptable, fair and effective and to adapt to national circumstances.
Against this background, it is up to each State to conduct a national dialogue with all stakeholders in order to define, in a participatory and consensual approach, the priorities of the SHP system and the choices in terms of coverage, financing, organization and operation. The challenge for each State is to build a unified national system offering cover to all categories of the population. This calls for consistency in the various measures, such as compulsory or automatic membership (or incentives for voluntary schemes), extended risk pooling, tax-based financing for the poorest households, proximity and simplification of procedures for insured persons. The State must define the population covered, the package of benefits to which it is entitled, the level of financial protection against the costs of these benefits and the network of service providers who deliver them. It then designates the public body or bodies responsible for implementation. These bodies may entrust certain tasks to delegated managers as part of a public service remit.
-
The State is responsible for regulating operations and the relationship between the various national insurance schemes: during the operationalization and functioning phases, the State has a right of oversight over the schemes that have been authorized to operate, referring to the legislative and regulatory texts governing them. The scope of State oversight varies. At the very least, when granting approval to a scheme, the supervisory ministries verify a priori that the scheme's configuration and functioning comply with the texts (for example, with the provisions of the Directive on regulating social mutual schemes within the WAEMU – see box below), as well as its viability. Beyond this, the State can also verify a posteriori that the commitments made with respect to the population are being honoured and that the management of the scheme complies with legal standards, including through supervisory procedures.
The influence of supranational organizations should be noted here. In 2009, the European Union adopted the Solvency II Directive, which came into force in 2016 and sets out a series of rules designed to increase the solvency of insurance companies in Member States, including delegated mutuals, particularly with regard to the principles of delegated management. For several years now, the WAEMU has been engaged in a process of implementing political and institutional reforms aimed at improving the state of health of the community's people through better financial access to healthcare. With this in mind, in June 2009 the WAEMU adopted Directive No. 07/2009/CM/UEMOA on regulating social mutual schemes. It then launched programmes and projects, including the support project for the extension of health risk coverage in WAEMU member countries (Projet d'Appui à l'extension de la Couverture du Risque Maladie dans les États membres, PACRM), in partnership with the French Development Agency (Agence Française de Développement,(AFD), to support implementation of the Directive. One of the main aims of this Directive was to strengthen mutuals so that they could become strong actors of SHP systems. However, in the light of previous observations concerning the need to make a distinction between mutuals and CBHI, and after some 15 years of implementation, a review or revision of the 2009 Directive would be useful to "narrow down" the mutual insurance landscape. In other words, it would be useful to give CBHI another space so that it could develop its own definitions and characteristics, avoiding confusion with mutual benefit societies.
Box
The development of the mutual society movement, which has had particular significance since the 2000s, and its role in policies to ensure that people have access to healthcare, has attracted the attention of the WAEMU Commission. These mutuals were in fact developing outside of an appropriate legal framework; only two WAEMU member countries (Mali and Senegal)* had a law governing mutuals. In 2005, the WAEMU Commission, with the support of the ILO and French and Belgian mutual societies, began the process of drafting an appropriate directive. This process, aimed at consulting and involving the main stakeholders, culminated in the adoption on 26 June 2009 of Directive No. 07/2009/CM/UEMOA on regulating social mutual schemes within the WAEMU.
The key objective of this text, complemented by implementing regulations, is to put in place a uniform, transparent and effective directive to ensure the sound promotion of social mutual schemes (which includes mutuals) in the WAEMU zone. This legal framework allows for the codification of the procedures for the creation, organization and functioning of mutual insurance organizations and to ensure sound risk management, with a view to promoting access to basic social services for people in WAEMU member countries. It also provides for the establishment by each member country of an administrative body for social mutual schemes, a national register of mutual societies and a national guarantee fund to safeguard the rights of social mutual scheme members.
* The WAEMU member countries are: Benin, Burkina Faso, Côte d'Ivoire, Guinea Bissau, Niger, Mali, Senegal and Togo.
The role of SHP management organizations
The organizations responsible for managing a national SHP system are themselves responsible for a remit entrusted to them by the State. As highlighted above, given the diversity and complexity of the insurance and related businesses, the management organization may choose to delegate certain tasks to other actors in order to focus on some important or critical functions.
However, delegating does not mean offloading some responsibilities onto these actors, and the delegator remains responsible for the remit and objectives entrusted to it by the State. In this context, it must supervise and oversee the activities of the delegated body, to ensure that the objectives of the delegation are achieved and that the interests of insured persons are protected.
The case studies show that national health insurance funds undertake this supervision and oversight activity when agreements are signed with mutuals or other delegated managers. However, more general oversight is also undertaken at state level by the ministries responsible for the national SHP system or by public bodies (for example, in Belgium) or by several national and regional entities, for example in Germany or Colombia.
In addition to the functions described above, SHP management organizations are also developing tools, in particular information systems made available to delegated bodies in order to harmonize the production of information, as well as mechanisms such as the payment of contributions and/or benefits via mobile platforms.
Box
The experience of Burkina Faso illustrates the risks associated with starting up too quickly and with insufficient initial definition of the delegated functions. The aim of this experience was to test the capacity of mutuals to carry out the insurance functions delegated by the CNAMU, in order to cover the poorest people, as well as the relevance of the RAMU management tools in extending cover nationwide and to other categories of insured persons. However, not enough prior discussion took place, particularly on the nature of the functions delegated, the healthcare package covered and the steering mechanisms. The procedures for producing information and the mechanisms for monitoring and evaluating community mobilization, enrolment, and the provision and payment of benefits provided for in the agreements have not been implemented. Overall, the strategy to cover the poorest people does not seem to have been understood in the same way by all actors.
The role of national non-governmental organizations and external partners in low- and middle-income countries
The role of local non-governmental organizations (NGOs) is given scant attention in the documents used to produce the case studies accompanying this working paper. However, they have gradually positioned themselves as implementing agencies for local or national programmes to promote mutuals. Their action is particularly important in implementing promotion programmes for community mutuals, which often result in the replication of a generic model (care package, tools, governance, management mechanisms, and so on) from one commune (or other administrative entity) to another. It is also common for these NGOs to speak on behalf of the mutuals they support, which leads to a degree of confusion between the support structures and the mutual society organizations they support.
It should be noted that the community mutuals promoted in this way respond well to the need for rapid results from TFPs, which have time-limited programmes. The spread of community mutuals can quickly justify covering a significant number of communes and registering large numbers of people. They are also well suited to the capacities of NGOs, which are used to working with communities, but often have limited technical expertise in health insurance management. The poor technical results and viability problems of community mutuals are often the consequence of this limited support capacity, but this cause is often masked by other reasons generally put forward, such as the lack of understanding of insurance by local communities and their weak contributory capacity.
This is another argument in favour of having a clear distinction between the different types of organizations commonly referred to as mutuals or CBHI identified in section 1.2. In this respect, it would entail:
-
revisiting the approach while making the most of NGO expertise in community mobilization;
-
lobbying external partners for support for national SHP systems and for investment in mutuals if they fit into this framework, with support for workers' organizations and other associations so that they can delegate functions to mutual society structures with a solid social base and all the necessary skills. Above all, it is a question of external partners agreeing to invest in interventions where the qualitative aspect is paramount (skills training, efficient technical and financial management procedures, production of information, and so on) and where the quantitative results (number of beneficiaries, and so on) will not be immediately important;
-
ensuring, lastly, that external technical support does not overshadow the expertise and know-how acquired by mutuals within public administrations, as well as those implemented by professional or corporatist organizations. These constitute a pool of skills and expertise.
Prerequisites for mutuals
Professionalized mutuals are generally quickly identified and contracted as delegated managers, if they exist at the time national SHP systems are being created or extended. This is also the case for community mutuals, although they are often faced with a number of challenges, as highlighted above, which hinder their development and their role within SHP strategies:
-
The management of SHPs cannot be improvised; rather, it requires technical expertise, material resources and competent human resources. However, the management of community mutuals suffers from a lack of technical capacity, and how they are managed is the result of numerous disadvantages linked to their characteristics:
-
They operate in the informal and agricultural sectors, where it is difficult to mobilize the expertise needed and requires extensive training of management teams.
-
The advisory support received by mutuals is rare and generally inadequate. Many mutuals receive external support, but it is often not enough to overcome all the management and strategic direction challenges. The transfer of expertise and techniques in insurance and risk management remains partial and does not make up for the lack of human resources. As highlighted above, the support structures (NGOs, projects, and so on) do not always have the necessary skills themselves and are often limited to "copying and pasting" a predefined model, including any shortcomings it may have.
-
Almost all community mutuals are managed on a voluntary basis, which makes it even more difficult to mobilize the expertise needed. In West Africa, this is due to a misinterpretation of the WAEMU directive, which stipulates that the position of administrator is voluntary, but provides in chapter III for the delegation of functions to salaried staff.
-
-
The production of information by community mutuals is very weak and often unreliable due to limited monitoring and evaluation processes, which reduces the ability of mutuals to comply with delegation agreements that include performance indicators and require an internal capacity to monitor membership, financing, including contributions if applicable, and benefits.
-
Relations with healthcare providers require a framework and a shared desire to comply with the agreement. In some countries, faced with technical difficulties or dependent on state subsidies that are unpaid, or only partially paid, mutuals become bad payers. Some healthcare providers also see mutuals as disruptive and a drain on resources. The negotiating capacity of community mutuals and their fragmentation do not allow these difficulties to be resolved at their level.
-
Lastly, community mutuals, which are aimed at the informal economy and are based on voluntary membership, are not very attractive. This situation is generally associated with the level of poverty and reduced contributory capacity of the target populations. But this explanation often masks the target communities' lack of trust in organizations with weak technical management and a level of dysfunction that compromises the quality and continuity of services. The reluctance to join is also often linked to a lack of local ownership, a lack of autonomy in decision-making and, more generally, to a lack of confidence in development projects, when mutuals are deployed in this context.
Box
An inventory of health mutuals carried out in 2021 in Burkina Faso (Burkina Faso, 2022) shows that 6 per cent of community mutuals across the country are no longer in operation, but are still counted as part of the mutual society movement. The other mutuals are in operation, but only provide partial information, and only 15 per cent of the mutuals surveyed were able to complete the inventory questionnaire. This questionnaire was based on the basic information that must be produced in accordance with the WAEMU directive. This situation is not unique to Burkina Faso; in Senegal, only 55 per cent of community mutuals were considered functional in 2017 (ILO, 2021b).
One mechanism among others
Other possible alternatives should not be ruled out, particularly when it comes to extending cover to the informal economy. For example, Cabo Verde has launched communications campaigns specifically targeting self-employed informal workers and has opened social protection service centres in places where there are large numbers of informal workers (for example, in informal markets). These service centres provide a source of information for workers, enabling them to register and pay their contributions. Their IT systems allow staff to carry out 80 per cent of administrative procedures in situ. This has led to a reduction in the amount of time spent by workers in accessing the scheme (UNDP, 2021). In Rwanda, CBHI organizations have been absorbed into a centrally managed health insurance system, which have become local branches. The country has also put in place simple, effective mechanisms: the national identity card is used as a means of identification for insurance and calls for contributions are made via the Irembo internet platform, which communicates with a series of databases, including the Ubudehe databases, to identify insured persons and set their level of contribution. Contributions are paid online, at Irembo branches, credit unions or via mobile banking operators. The tasks entrusted to the CBHI have thus been transferred to other operators, while maintaining proximity to insured persons and simplifying procedures.
Another alternative is the one put in place in Uruguay, where workers in the formal public and private sectors, retirees and their dependants (68 per cent of the population) are covered by the contributory health insurance scheme. The rest of the population is covered by the State Health Services Administration, (Administración de los servicios de salud del Estado) which manages public health establishments with resources allocated by the State from the budget. Another special feature is that all insured persons must register with a healthcare provider in order to be enrolled in the national health insurance system. This same approach was adopted by the Lao People’s Democratic Republic after CBHI was discontinued in 2016.
Conclusion
Observation of the experiences of 17 countries in Africa, Asia, Europe and Latin America highlights the diversity in the organization of SHP systems and, within these, the various models for integrating mutuals. It also underlines the indiscriminate use of the term "mutual" for organizations as long as they include a participative dimension in their management. This is particularly true of CBHI, which has been the focus of major development efforts in a number of countries over the last two decades, with generally poor results today in terms of financial protection and access to healthcare. The disappointment resulting from the limited impact of community mutuals tends, by extension, to discourage general interest in mutuals today. However, mutuals developed by professional organizations and other organizations in the social economy have social capital and build close relationships with their members, as well as a flexibility in how they function, which make them potentially key players in an SHP system, especially when it comes to covering difficult-to-reach populations within the informal economy and the agricultural community. These mutuals have developed expertise enabling them to participate effectively in the administration of the basic schemes, the management functions of which they have been delegated wholly or in part.
What lessons can be drawn for future work?
-
Insurance is a complex tool, and each actor in the SHP system architecture must have the technical capabilities and the human and material resources required to carry out its remit.
-
The term mutual covers different circumstances and clarification is needed on concepts and legal frameworks to avoid underplaying mutual society insurance dynamics.
-
The previous point concerns in particular CBHI; of key importance would be to create a distinctive space for CBHI adapted to its characteristics, which are different to those of mutual society insurance. It would also be more appropriate to conduct a specific review of this approach, the upscaling of which is fast coming up against a number of limitations.
-
Mutuals originating from socio-professional organizations, generally inspired by the mutual society movement that emerged in Europe and which have spread to many countries, are an important pool of skills, expertise and know-how. In some countries, including those in the WAEMU zone, the experience acquired by these mutuals can usefully support the development of mutual society insurance by workers' organizations, producers' organizations and corporatist and professional associations.
-
Mutual societies are not the only possible option for extending social protection to people in the informal and agricultural sectors. Countries such as Cabo Verde and Rwanda have developed alternative mechanisms based on new communications technologies.
-
Finally, as these are complex mechanisms, national health insurance system documentation should focus on their technical aspects and use health insurance indicators to clearly identify their weaknesses, which are all too often obscured behind a lack of understanding and the limited capacity of target populations to contribute.
Annex – Case Studies
1. Belgium
1.1 Background
As in France and Germany, SHP in Belgium is the result of a long-standing process that has evolved through several stages. It is linked to the development of industrialization in the nineteenth century, which generated significant poverty among the working class and led to the creation of mutual aid funds, started by guilds in the case of the oldest funds, as well as by workers, middle-class philanthropists or employers with social concerns. The aim of these mutual benefit societies was to provide support to their members when they became impoverished or found themselves in economic difficulty due to illness. However, protection was precarious and relied solely on the goodwill of private actors, whose basic management and limited membership prevented them from developing serious guarantees.
Faced with the growing poverty of the working-class population, the State intervened to facilitate the creation and development of these organizations with the adoption of the law of 3 April 1851 on mutual societies. This law was amended by the law of 23 June 1894 4 which, under certain conditions, granted legal recognition to any mutual society organized to provide protection for its members in the event of illness, invalidity, birth, death or old age. Recognition is linked to the filing of legally compliant statutes and the submission of annual accounts. In addition, rather than promoting compulsory social insurance, the 1894 law adopted the principle of subsidized freedom by encouraging free membership of State-subsidized mutual funds. This option was bolstered by the 1898 law, 5 which made subsidies to mutual societies provided they were legally recognized.
The implementation of the 1894 law led to a proliferation of mutual societies, emerging from initiatives from different ideological backgrounds; those of the same persuasion began to form federations, particularly so as to be able to insure certain major risks. These federations then grouped together into national unions, which made a major contribution to the "pilarisation" 6 of Belgian society (CRISP, 2022), with the creation of:
-
Alliance nationale des mutualités chrétiennes (National Alliance of Christian Mutual Insurance Funds – ANMC), in 1906;
-
Union nationale des mutualités neutres (National Union of Non-denominational Mutual Insurance Funds – UNMN), in 1908;
-
Union nationale des mutualités socialistes (National Union of Socialist Mutual Insurance Funds –UNMS), in 1913;
-
Ligue Nationale des Mutualités libres de Belgique, in 1914, now the Union nationale des mutualités libérales (National Union of Liberal Mutual Insurance Funds – UNML ); and
-
Union nationale des Fédérations de Mutualités professionnelles des industries de la Belgique, in 1928, now the Union Nationale des Mutualités Libres (National Union of Occupational Mutual Insurance Funds – UML).
The Social Security Act adopted on 28 December 1944 7 laid the foundations for the first compulsory social security system for all employed workers, including the introduction of compulsory health insurance. Following this law, the health insurance system gradually evolved towards universal coverage extending to non-workers, vulnerable persons, self-employed persons and civil servants (CRISP, 1964). In 1963, for example, the Leburton Act 8 reformed compulsory health insurance with the aim of covering new population groups, such as the self-employed and students, and introducing a system of negotiated agreements (conventions) between healthcare providers and health insurance funds setting tariffs and reimbursement levels. This reform also established the National Institute for Health and Disability Insurance (INAMI) (De Troyer and Krzeslo, 2004).
Another important step was the redefining of the remits of mutual societies with the adoption of the law of 6 August 1990, 9 which sets out the conditions that these mutual societies and national unions of mutual benefit societies must meet to obtain legal personality, as well as the basic rules for their operation. It also organizes the supervision to which mutual societies are subject by creating the Office for the Supervision of Mutual Societies and National Mutual Unions (OCM). Under this law, only the national unions and federations are recognized for the management of compulsory health insurance. Local mutual societies disappeared, although some unions retained local branches in order to remain in close proximity to their members. The 1990 law also protects the term "mutualité", which was adopted by federal associations at the expense of the term "fédération" (Dresse, 2006).
1.2. The national social health protection system
Architecture and governance
The Belgian SHP system is based on compulsory social insurance, founded on the principle of solidarity between all Belgian residents and voluntary complementary insurance.
Compulsory insurance:
General health insurance administration is the responsibility of the INAMI, which was set up in 1944 and is now governed by the 1994 law. 10 The INAMI is a public body with legal personality responsible for managing, overseeing and coordinating the various stakeholders involved in health insurance (mutual societies, healthcare providers, trade unions and employers' organizations).
The INAMI is organized into a number of bodies, including a general management committee, which is responsible for the administrative and general management of the institute. It is a tripartite body composed of an equal number of representatives of employers' organizations and organizations representing self-employed workers, organizations representing employees and representatives of mutual societies and public auxiliary funds, plus three government representatives (De Troyer and Krzeslo, 2004). Other committees are responsible for insurance management, budgetary oversight, medical examinations and checks, and so on.
However, the INAMI does not pay benefits directly, as these are managed by the mutual societies and two public insurers: the Caisse Auxiliaire d'Assurance-maladie Invalidité (Health and Disability Insurance Auxiliary Fund – CAAMI) and the Caisse des Soins de Santé de la Société Nationale des Chemins de Fer Belges (Belgian National Railway Company Healthcare Fund, HR Rail CSS).
The CAAMI performs the same tasks and provides the same benefits as a mutual society for compulsory health insurance, but does not offer complementary insurance. As a result, insured persons do not have to pay any contributions other than the social security contributions collected by the Office National de Sécurité Sociale (National Social Security Office, ONSS), part of which is paid to the INAMI for compulsory health insurance. The CAAMI is a public institution run by a joint management committee representing employers' and employees' organizations.
The HR Rail CSS also acts as a mutual society for statutory employees of the Belgian Railways and their families, solely for compulsory insurance benefits. An internal social fund provides additional cover, and staff members can also choose to join a mutual society to benefit from additional cover.
The choice of insurer is free, except for statutory employees of the Belgian National Railway Company, who are required to register with the HR Rail Health Care Fund. The choice of insurer has no impact on compulsory insurance contributions and reimbursements: contributions are included in the social security contribution collected by the ONSS (or the Institut national d'assurances sociales pour travailleurs indépendants (National Social Insurance Institute for Self-employed Persons, INASTI) and the terms and level of reimbursement of healthcare expenses are set by the INAMI and are identical for all insurers. Individuals' choice of mutual insurer is often influenced by the religious or political affiliations that underpin the five major national mutual unions.
Mutual societies are subject to external oversight by the OCM, a non-profit organization under the supervision of the Minister for Social Affairs. The OCM ensures that the services and activities of the mutual societies and national unions comply with legal provisions, particularly administrative, accounting and financial rules. It also formulates opinions and proposals relating to their operation. The OCM is managed by a governing body, which is independent of the mutual societies, and by a technical committee.
In addition, the five mutual unions are allied with the CAAMI and the HR Rail Health Care Fund to form the Collège intermutualiste national (National Inter-Mutual College, CIN). This alliance represents all beneficiaries of compulsory health insurance, with a remit to:
-
set up collaboration between the various insurers on all matters of interest relating to compulsory and complementary health and disability insurance and to the mutual insurance sector in general;
-
take a stance on these matters, taking into account the interests of all insured persons; and
-
encourage joint action or cooperation in the management of insurers (https://www.cin-nic.be/).
Complementary insurance:
Under the provisions of the 2010 law 11 on complementary health insurance, the five mutual societies require their members to take out complementary insurance, which was previously optional. Individuals who do not wish to benefit from this complementary insurance can join the CAAMI, which is confined to compulsory insurance. Members of mutual societies must therefore pay a contribution, in addition to the social security contribution collected by the ONSS, the amount of which varies from one mutual society to another, for services which are also diverse and cover some expenses that are only partially reimbursed, or not reimbursed at all, by compulsory health insurance. To assert their identity and to project a more commercial image, mutual societies add benefits such as covering the cost of sports club subscriptions, holiday courses and camps, home childcare, vaccinations, crutch hire, osteopathy, cancer screening, birth grants, and so on.
To enable members who so wish to benefit from even more comprehensive cover, mutual societies also offer the opportunity of joining optional insurance schemes.
Population coverage
Compulsory health insurance covers around 99 per cent of the population. The remaining 1 per cent is primarily made up of people who do not have their administrative or financial obligations in order. Such uninsured people may, however, be covered by other systems, mainly through public social action centres, such as the emergency aid mechanisms available to people in an irregular situation or with no fixed address.
To be covered, individuals must join a mutual society or an auxiliary fund (membership of the HR Rail CSS is compulsory for Belgian National Railway Company employees).
As of 31 December 2021, membership breakdown was as follows:
Breakdown of membership in insurance companies
|
Insurer |
Number of individuals covered |
Percentage of individuals covered |
|
ANMC |
4 600 893 |
40.3% |
|
UNMS |
3 252 667 |
28.5% |
|
UML |
2 232 397 |
19.6% |
|
UNMN |
573 696 |
5.0% |
|
UNML |
539 577 |
4.7% |
|
CAAMI |
118 857 |
1.0% |
|
HR Rail CSS |
99 548 |
0.9% |
|
Total |
11 417 635 12 |
100.0% |
Source: INAMI statistics (https://www.inami.fgov.be/fr/programmes-web/Pages/programme-web-statistiques-personnes-affiliees-mutualite.aspx)
Insured persons include:
-
employees, civil servants and self-employed workers; and
-
workers who pause or cease their taxable activity: unemployed persons, persons recognized as unable to work, pensioners, and pregnant women from the fifth month of pregnancy.
The insured's dependants who may be recognized as beneficiaries:
-
legal spouse;
-
spouse who is not divorced but is separated;
-
children under the age of 25;
-
descendants; and
-
cohabitants (CLEISS, 2019).
Risks covered/healthcare package
Compulsory health insurance covers a range of preventive and curative treatments listed in the list of reimbursable services established by royal decree. This list specifies the official tariffs and co-payments, which are set by national agreements and conventions negotiated each year (or every two years) between representatives of the mutual societies and healthcare providers. The list includes:
-
visits and consultations by general practitioners and specialist doctors;
-
care provided by physiotherapists;
-
care provided by nurses and home nursing services;
-
dental care;
-
childbirth;
-
prosthetic devices, wheelchairs and buggies, dressings and implants;
-
hospital care;
-
care in nursing homes for the elderly; and
-
functional rehabilitation care.
The level of reimbursement varies essentially depending on the nature of the service, the status of the beneficiary and the quality of the healthcare provider. The co-payment to be borne by the patient generally amounts to 25 per cent of the cost of the service, be that for consultations, medications (the rates and conditions of reimbursement are not set by agreement, but by royal decree) and the number of hospitalization days, for which the insured person's co-payment depends on the choice of room and the period of hospitalization (Reman, 2015).
Basically, healthcare operates under a reimbursement system, with patients having to pay in advance. However, the third-party payment system, initially applied only to prescription drugs and hospital/residential care, tends to be extended to outpatient care (primarily for vulnerable social groups and the chronically ill). The lump-sum system is also used for some medical centres, with an amount paid by mutual societies in proportion to the number of patients registered.
Healthcare is provided by contracted providers (over 80 per cent of healthcare providers and organizations), which include public health services and private healthcare professionals for outpatient care, private pharmacists, public and private non-profit hospitals and special establishments for the elderly. Insured persons also have access to non-contracted service providers, for which they are covered only up to the tariffs set by the INAMI.
Insured persons are free to choose their healthcare providers and can access most specialist and hospital care without prior assessment by a general practitioner (Reman, 2015).
Insurers offer the same cover to all their members, although there are some exceptions through three specific mechanisms: the Higher Reimbursement Rate, the Maximum Invoice Payable, and the Special Solidarity Fund.
Higher Reimbursement Rate:
This mechanism is designed to facilitate access to healthcare, with enhanced reimbursement of services and medicines to:
-
people assisted by public welfare centres, elderly persons who benefit from the guaranteed income for the elderly and children with disabilities with a physical and mental disability of at least 66 per cent;
-
social welfare recipients: pensioners, the unemployed, persons with disabilities, public service employees on sick leave, and single-parent families whose gross income is below a certain level; and
-
all people whose household income is below a certain level.
Thanks to the automation of electronic data flows between the social security institutions and mutual societies, the latter automatically verify entitlement to the higher reimbursement rate for their beneficiaries, who do not have to take any steps themselves (BCSS, 2021).
Maximum Invoice Payable:
This second mechanism is designed to limit the annual healthcare expenditure of the most socially or medically vulnerable patients. The mechanism comes into play when the total amount of co-payments paid by a patient, calculated automatically by the insurers, reaches a certain ceiling during the year. When this ceiling is reached, the co-payments are paid by the insurer for the benefits that will be used during the rest of the year. There are four types of maximum invoice, each calculated differently to determine the maximum co-payment:
-
The maximum invoice payable according to income, which applies to all patients depending on their level of income.
-
The maximum social invoice payable, mainly granted to beneficiaries of the higher reimbursement rate and to persons with disabilities.
-
The maximum invoice payable for children under 19, which is not means tested.
-
The maximum invoice payable for chronic illnesses.
The Special Solidarity Fund:
This scheme is managed by the INAMI, with a limited annual budget. Its aim is to prevent a patient in a serious medical situation from having to forego an essential medical service that is particularly expensive and not reimbursed by compulsory health insurance. Intervention by this fund is subject to certain conditions, including the submission of a request in principle before a medical procedure or a request within three years of the procedure, to the medical officers of the insurers (CLEISS, 2019).
Financing
Compulsory health insurance is a branch of the social security system and as such forms part of the overall mechanism for financing and managing the system. The financing of compulsory health insurance involves a number of different stakeholders. A total of 66 per cent of revenue comes from contributions collected by the ONSS for the employees' scheme 13 and by the INASTI for the scheme for self-employed persons. These two bodies collect together contributions and allocate them as required to the management organizations of the various social security branches, including the INAMI for health insurance. The rest of the funding comes from the State budget (24 per cent of health insurance resources) and alternative funding (10 per cent, mainly revenue from value added tax (VAT)) (Moudhi, 2018).
INAMI allocates a projected budget to the insurers, taking account of each insurer's share of health insurance expenditure and the risk profile of its insured population. At the end of the year, the insurer's expenditure is compared with the budget received. If the insurer has spent less, it receives a bonus of 25 per cent of the difference, which is allocated to its special reserve fund. Where it has spent more, the insurer covers 25 per cent of the shortfall from its special reserve fund. All insurers are required to set up this special reserve fund.
1.3 Delegated management placing mutual societies at.the heart of compulsory health insurance
Mutuals
Article 2 of the Belgian law of 6 August 1990 on mutual societies and national mutual unions defines mutual societies as associations of natural persons which, in a spirit of providence, mutual assistance and solidarity, aim to promote physical, mental and social well-being. They operate on a non-profit basis (Law of 6 August 1990).
The 1990 law lays down certain conditions for obtaining recognition and for using the terms "mutual", "sickness fund", "mutuality" and "mutualist" in the names of mutual societies:
-
There should be a minimum number of members (this number is set by the King).
-
Establishment of at least one service with the aim of:
-
participation in the implementation of compulsory health care insurance and benefits;
-
providing financial assistance for members and their dependants towards the costs of preventing and treating illness and disability, or granting compensation for incapacity to work or when a situation arises in which physical, mental or social well-being can be promoted; and
-
the provision of help, information, guidance and assistance with a view to promoting physical, mental and social well-being, inter alia by carrying out its tasks.
The condition set for national unions is that they must have at least two member mutuals offering the above services.
This legal framework gives a special place to mutual societies, which can only obtain or maintain legal personality if they participate in compulsory healthcare insurance. They are thus closely involved in the management of compulsory health insurance and act as an interface between the INAMI and the citizen (CES, 2017).
Although they act as quasi-parastatal institutions – the National Bank of Belgium's accountants include mutuals in the public administration sector for their activities relating to compulsory health and disability insurance – they remain social economy organizations, distinct from the State, particularly in terms of the complementary insurance and very diverse social services, especially in home care, which they develop autonomously (CES, 2017).
As mentioned above, another distinctive feature of Belgian mutual societies is their philosophical and political basis, the three largest being the Christian mutual societies, the socialist mutual societies and the professional mutual societies. These mutual societies have retained traces of the different ideological worlds from which they originate, thus contributing to the "pilarisation" of Belgian society. However, these religious or ideological references have lost some of their importance over time in the distinctions between mutual societies (Reman, 2015).
Legal institutional framework
The national SHP system involves a number of stakeholders and institutions in the operation of compulsory health insurance, including social security funds, which collect contributions, the INAMI, which organizes and manages healthcare insurance, the implementation of which is entrusted to the insurers, and the OCM, which monitors the insurers' compliance with their financial and accounting obligations. The management of compulsory health insurance is also based on social dialogue, which involves healthcare providers and the social partners (SPF Sécurité sociale, 2012).
Within this system, the general principles of the administrative organization, financing and budget of compulsory health insurance are determined by the law of 14 July 1994, and in the royal decree implementing the law on compulsory health insurance and compensation, coordinated on 14 July 1994. This law gives the five national mutual unions and the two auxiliary funds (the CAAMI and the HR Rail CSS) a key position in the compulsory health insurance system. Within this framework, the national unions perform three main functions:
-
A technical function as the insurer responsible for providing compulsory insurance.
-
A social function with the implementation of indirect hospital initiatives and social services – mutual societies are social economy organizations.
-
Political functions as social partners and actors in health policy.
Distribution of functions
The term "delegated management" does not appear in legislation and documents relating to compulsory health insurance in Belgium. However, broadly speaking, the INAMI is responsible for the general administration of the insurance, with implementation delegated to the insurers. Among the latter, the unions of mutual benefit societies in turn delegate some of their functions to their member mutual societies.
More broadly, the system is based on a division of functions between several actors:
-
The social security bodies, the ONSS and the INASTI are responsible for the overall collection of contributions for the various branches of social security and their distribution between the bodies managing these branches, including the INAMI.
The INAMI is responsible for the administrative and financial management of compulsory health insurance and benefits. Its healthcare department is responsible for a range of functions, including:
-
pooling of resources from social security contributions and State transfers;
-
preparing the budget and organizing appropriate funding for the activities of insurers and healthcare providers;
-
organizing reimbursement of medical expenses;
-
monitoring trends in healthcare expenditure;
-
information for healthcare providers, insurers and insured persons;
-
monitoring compliance with legislation and regulations;
-
organizing negotiations between the various actors in compulsory health insurance; and
-
drafting legislation and regulations.
-
The mutual unions are the insurers responsible for implementing health insurance and providing benefits to beneficiaries:
-
they monitor healthcare expenditure and ensure that it complies with legal requirements;
-
they collectively organize negotiations with healthcare providers: every two years, representatives of the mutual societies meet with the healthcare providers to set the level of tariffs that the latter are invited to charge for the following two years, with the aim of guaranteeing tariff security for patients and keeping the healthcare insurance budget under control; and
-
they generally oversee the smooth running of member mutuals, including complementary insurance.
-
-
The unions delegate to the mutual societies part of their remit to provide compulsory insurance. Within this framework, the mutual societies:
-
reimburse all or part of healthcare costs;
-
ensure close proximity to their members through their local mutual society branches and offices, and organize health information and promotion campaigns;
-
defend the interests of their members; and
-
report to their national union.
-
Mutual societies also offer reimbursements, services and benefits in addition to compulsory insurance. They also act as healthcare providers by managing hospitals and paying doctors and a large medical staff. The mutual sector is therefore part of the non-commercial hospital sector alongside other private non-commercial hospitals.
Distribution of functions
|
Functions |
Distribution |
|||
|
ONSS and INASTI |
INAMI |
National unions |
Mutual societies |
|
|
Definition of the healthcare package |
X |
|||
|
Agreements |
X |
X |
||
|
Education and promotion |
X |
X |
X |
|
|
Enrolment, membership and renewal |
X |
|||
|
Contribution collection |
X |
|||
|
Mobilizing resources |
X |
X |
||
|
Pooling of risks covered |
X |
X |
||
|
Payment of benefits |
X |
|||
|
Healthcare services |
X |
|||
|
Follow-up and steering |
X |
X |
||
1.4 Impact and lessons learned
Since its creation in 1944, compulsory health insurance has undergone a gradual evolution, passing through a number of changes, to become a universal coverage that today offers broad protection to more than 99 per cent of the Belgian population against the financial risks associated with illness.
Mutual societies are at the root of the current architecture of compulsory insurance, in which they play a key role. This role has sometimes been contested, notably when the 1963 law introduced the requirement for healthcare providers to sign agreements with the mutual societies, leading to a nationwide doctors' strike. There have also been periods of vagueness and debate, particularly in the late 1980s, over the role of the mutual societies and control of the resources collected as part of the social security system. Against this backdrop, the laws of 1990 and 1994 were a key step in reforming the world of mutual societies and providing them with an appropriate framework for action, with a view to ensuring transparency. Until then, mutual societies were governed by the 1894 regulations, which no longer corresponded to the realities and rules of governance and oversight in the context of compulsory health insurance.
As mentioned above, compared with other European Union countries where mutual societies are mainly active in complementary health insurance, the legal framework in Belgium gives a special place to mutual societies, which are the primary insurers of compulsory insurance and whose legal personality is conditional on their participation in compulsory insurance.
However, it is important to stress that mutual societies are not reduced to the role of reimbursement branch offices. They are social economy organizations and, particularly in the case of the largest socialist and Christian mutual societies, they retain their social and activist roots. They play an active role in improving access to healthcare through their social medical services (healthcare services, home help, and so on) and their leading role in debates on national health policy. Mutual societies also attach particular importance to health information and education. In 2016, for example, the mutual societies signed the "pact for the future with insurers" with the Minister for Social Affairs and Public Health, which strengthens their role in informing members about the healthcare system and health in general, empowering patients and promoting healthy lifestyles.
References
BCSS (Banque-carrefour de la sécurité sociale). 2021. "Intervention majorée de l'assurance soins de santé". https://www.ksz-bcss.fgov.be/fr/project/intervention-majoree-de-l-assurance-soins-de-sante.
CES (Centre d’économie sociale). 2017. "Mutualities". CES, December 2017. http://www.ces.uliege.be/mutualites/.
CLEISS (Centre des liaisons européennes et internationales de sécurité sociale). 2019. "La protection sociale en Belgique”. https://www.cleiss.fr/docs/regimes/regime_belgique.html.
CRISP (Centre de recherche et d’information socio-politiques). 1964. "Les mutualités en Belgique". Courrier hebdomadaire du CRISP 258, nᵒ 33: 1–15. https://doi.org/10.3917/cris.258.0001.
— 2022. "Mutualité". https://www.vocabulairepolitique.be/mutualite/.
De Troyer, M. and Krzeslo, E. 2004. "Belgique – Assurance-maladie, soins de santé et sécurité sociale: trois éléments indissociables". Chronique Internationale de l'IRES: 91 (Special edition, November 2004). http://www.ires.fr/index.php/publications/chronique-internationale-de-l-ires/item/3909-belgique-assurance-maladie-soins-de-sante-et-securite-sociale-trois-elements-indissociables.
Dresse, R. 2006. "100 ans de la Mutualité chrétienne – La mutualité : une histoire plus que centenaire". En Marche, 2006. https://archives.enmarche.be/Mutualite_chretienne/La_mutualite_histoire_centenaire.htm#1
Mouhdi, H. 2018. "L'apport d'un système d'information intégré à la couverture médicale de base, cas du Maroc". Doctoral thesis, Faculty of Medicine and Pharmacy, Mohammed V University, 2018.
Reman, P. 2015. “La protection sociale en Belgique”. CEPSE (Europa, Centre d’Étude sur la Protection Sociale en Europe). https://www.europaong.org/wp-content/uploads/2015/09/EUROPA-CEPSE-BELGIQUE.pdf
SPF (Service public fédéral) Sécurité sociale. 2012. "Aperçu de la sécurité sociale en Belgique". https://socialsecurity.belgium.be/fr/publications/apercu-de-la-securite-sociale-en-belgique.
Other documents consulted:
Gerkens S. and Merkur S. 2020. "Belgium: Health system review 2020". Health Systems in Transition 22(5), 31 December 2020. WHO, European Observatory on Health Systems and Policies. https://eurohealthobservatory.who.int/publications/i/belgium-health-system-review-2020.
INAMI (Institut national d'assurance-maladie-invalidité). 2014. L'assurance soins de santé et indemnités belge : Repères du passé, balise pour le futur. https://www.inami.fgov.be/SiteCollectionDocuments/brochure-50-inami.pdf.
INAMI website: https://www.inami.fgov.be/fr [accessed on 15 October 2023].
OCM (Office de contrôle des mutualités. 2022. Rapport annuel 2021. June 2022. https://www.inami.fgov.be/SiteCollectionDocuments/brochure-50-inami.pdf.
2. Burkina Faso
2.1 Background
The construction of a national universal health insurance system is one of the objectives of pillar II on developing human capital of Burkina Faso's National Economic and Social Development Plan (PNDES 2016–2020) and is included in PNDES II (2021–2025). It is also a key objective of the National Social Protection Policy (PNPS 2013–2022) and the Sectoral Labour, Employment and Social Protection Policy (PS/TEPS 2018–2027). The Régime d’assurance-maladie universelle (Universal Health Insurance Scheme, RAMU) was introduced in 2015 14 with the aim of promoting access to healthcare for the entire population residing in Burkina Faso and protecting them against financial hardship in the event of illness, through compulsory contributions, and ensuring cover for the poorest people without the financial means to pay the contributions. In 2018, the Caisse nationale d'Assurance-maladie universelle (National Universal Health Insurance Fund, CNAMU) was created 15 to manage the RAMU for the civilian population (PSD-CNAMU, 2022).
The path towards bringing the RAMU into operation is somewhat gradual, with many challenges to overcome. Burkina Faso is a low-income country with a poorly diversified economy that is structurally vulnerable to external shocks. In particular, the country is highly exposed to the effects of Sahelian instability and since 2016 has experienced repeated armed violence, triggering a serious humanitarian crisis with more than 1.7 million persons displaced. The country is also vulnerable to the adverse impact of global warming, particularly in the Sahel region, and an estimated 3 million people are suffering from food insecurity.
Based on its Strategic Development Plan (PSD-RAMU) 2019–2023, the process of bringing the RAMU into operation was still ongoing in 2022. The CNAMU does not provide any benefits, except for cover for the poorest people as part of a pilot project undertaken in 2020, in partnership with mutuals and national NGOs.
2.2 The national social health protection system
Architecture and governance
The aim of the RAMU is to implement a basic compulsory scheme for all and thus to decompartmentalize the current mechanisms in order to organize the pooling of risks on a national scale. The field of SHP is currently fragmented, with several mechanisms in place:
-
The universal health insurance scheme, which aims to gradually extend UHC to the entire population, with two management structures (see below).
-
The CNAMU, which manages the RAMU for civilians and their families, including workers and their dependants in the formal, informal and agricultural sectors, as well as poor households, by combining a contributory and non-contributory scheme.
-
The Caisse d'assurance-maladie des armées (Armed Forces Health Insurance Fund, CAMA), 16 which manages the RAMU for members of the national armed forces and their families.
-
Voluntary private insurance systems. Pending the RAMU coming into operation, private insurance is currently the only active coverage system, with several mechanisms (described below).
-
Community mutuals are open to all population categories. They are the result of local community initiatives and are generally organized on a territorial basis (for example, communal mutuals) or by groups of workers in the informal or agricultural sectors (for example, mutuals for cotton producers). These social mutuals have not developed any other form of activity alongside health expense cover.
-
Professional mutuals are found mainly in public administrations and in certain large enterprises or trades within the formal economy. These professional mutuals also offer a variety of services to their members in addition to health insurance, including mutual aid (particularly for social events) and solidarity activities, microfinance (education loans, loans for social events and loans to provide life’s essentials) and assistance with financing income-generating activities.
-
Commercial insurance and private enterprise schemes. As part of their internal social policy, some enterprises have set up medical schemes managed internally by the enterprise or in partnership with a commercial insurance company. These schemes are poorly documented and cover only a small proportion of Burkina Faso's private-sector workers and expatriates. The National Assembly also takes out insurance policies for its members.
-
Free healthcare programmes include free healthcare for women and children under the age of five, as well as the development of measures for the elderly and persons with disabilities. There is also the provision of treatment for certain diseases such as HIV/AIDS, leprosy and tuberculosis.
-
Subsidies to public institutions and municipalities. The government provides direct funding to promote access to healthcare in the form of:
-
assigned funds, which include subsidies granted to public establishments to guarantee access to healthcare services for the entire population; and
-
transferred credits, granted to municipalities to improve the infrastructure and facilities of public establishments under their jurisdiction.
The formal social protection system covers less than 10 per cent of the population. In 2012, the Institut national de la statistique et de la démographie (National Institute for Statistics and Demographics, INSD) estimated that only 2 per cent of the population was covered by health insurance (excluding free programmes). This estimate continues to be used today in the absence of more recent data. An inventory of social mutuals carried out in 2020 estimates that 0.15 per cent of the total population of Burkina Faso is effectively covered by a SHP mechanism managed by these mutuals (Burkina Faso, Ministry of the Civil Service, Labour and Social Protection 2022; CNAMU, 2021).
Target populations and healthcare packages
Risk pooling varies greatly according to the different coverage systems. Overall, risk pooling is limited in the existing systems: community mutuals are small, with an average of 350 beneficiaries. Professional mutuals have an average of 1,280 beneficiaries but remain limited to the size of the administrations or enterprises in which they were set up.
The CNAMU's long-term objective is to harmonize this cover by offering a basic scheme for all, including by integrating current free programmes. A decree to be adopted by the Council of Ministers sets out the content of this healthcare package, which includes general medical procedures and medical and surgical specialities, nursing procedures, antenatal care, childbirth and postnatal care, procedures and care linked to hospitalization and surgical interventions, emergency oral and dental treatment, laboratory medical tests, radiology and medical imaging procedures, and functional explorations.
The 2020 inventory of social mutuals shows that professional mutuals offer extended cover to all levels of the health pyramid and to public, denominational and private for-profit healthcare providers. Community mutuals are mainly confined to the primary and, in the case of urban mutuals, secondary levels; two regional unions (out of the existing 11) also offer secondary and tertiary level cover for the beneficiaries of their member mutuals. In all cases, community mutuals essentially cover public and denominational health services, as well as private laboratories and medical imaging centres, in order to compensate for the deficiencies in public services.
Financing
Social mutuals are financed by lump-sum contributions from their members, with contributions ranging from an average of 3,550 CFA francs per year per person for community mutuals to an average of 24,125 CFA francs per year per person for professional mutuals. One-off programmes cover contributions, or even co-payments, for certain beneficiaries, such as a pilot project run by the World Bank in 2014 in two provinces and the inclusion of urban refugees in mutual insurance schemes by the Office of the United Nations High Commissioner for Refugees (UNHCR).
The free healthcare programmes are financed by the national budget, based on tax resources and budgetary support from external partners. With regard to the policy of free healthcare for pregnant women and children from birth to four years of age, launched in 2016, the government has been experiencing difficulties in distributing the amounts needed since 2018.
Despite these free insurance mechanisms, user charges remain high, representing 31.7 per cent (in 2017) of health sector funding (PHCPI, 2022).
2.3 Mutuals
The inventory carried out in 2020 by the Ministry of the Civil Service, Labour and Social Protection, with ILO support, showed that there were 233 social mutuals in 2020, 17 divided into two main groups:
-
A total of 62 professional mutuals set up by workers in public institutions, enterprises or from the same trade guild within the formal economy. Ten of these mututals provide health insurance for 8,971 beneficiaries. These mutuals are grouped into three unions, which are themselves members of the Fédération des mutuelles professionnelles et caisses de solidarité du Burkina Faso (Federation of Professional Mutuals and Solidarity Funds in Burkina Faso, FMP/BF).
-
Some 171 community mutuals, emerging from local community initiatives and generally organized on a territorial basis (for example, communal mutuals) or by groups of workers in the informal or agricultural sectors (for example, mutuals for cotton producers). These mutuals were set up with the support of national NGOs, generally as part of programmes funded by external partners. In 2020, they had a total of 35,922 registered beneficiaries, including 29,844 in receipt of benefits. Since the 2010s, community mutuals have become more structured, with the creation of regional unions and the Fédération des mutuelles sociales communautaires (Federation of Community Social Mutuals, FEMUSCO) at the national level.
The growth of this mutual movement is slow. A comparison with a previous inventory carried out in 2011 even shows a decrease in the number of beneficiaries in the 171 community mutuals, resulting from an operation to clean up the membership registers, undertaken at the instigation of the NGOs supporting the mutuals, with the removal of insured persons who were no longer contributing.
The professional social mutuals on the one hand, and the community social mutuals in association with their regional unions on the other, theoretically offer extensive coverage at all levels of the health pyramid. However, only two unions offer complementary cover to the community mutuals, and these cover only a fifth of the total number of beneficiaries recorded. Overall, the coverage provided by community mutuals is therefore concentrated on small risks (local level of the health pyramid). This cover is further limited by weaknesses in technical management, which have an impact on the continuity and quality of the cover offered by the community mutuals and reduce their attractiveness to the target populations (Burkina Faso, Ministry of the Civil Service, Labour and Social Protection, 2022).
2.4 Experimenting with delegated services for the poorest people
The CNAMU is experimenting with a system of delegated management to mutuals through an initial four-year pilot phase, starting in 2019, for coverage of the poorest people in four regions of the country. This pilot phase will pave the way for the roll-out of the RAMU and is the only delegated mechanism currently in existence in Burkina Faso.
Legal framework
The CNAMU, the management organization of the RAMU, may delegate some of its technical functions, as provided for in the following articles of Law No. 060-2015/CNT:
-
Article 40 – The management organizations referred to in article 38 above [the CNAMU and the CAMA] may delegate some of their technical functions to so-called delegated management organizations, in particular other social welfare institutions, social mutuals, private insurers and private health management companies. The delegation of functions is recorded in a delegated management agreement. Article 41 prohibits the simultaneous management of functions delegated by the CNAMU and the management of health establishments.
-
Article 42 – A regulatory body for universal health insurance oversees relations between the management organizations, delegated management organizations and healthcare providers or any other providers in relations with the said management organizations. The regulatory body is created by decree issued by the Council of Ministers.
However, the experiment with delegated management for coverage of the poorest people was immediately confronted with the absence of a clear legal framework for mutuals. They are governed by Directive No. 07/2009/CM/UEMOA, but this has not yet been transposed in Burkina Faso. To date, social mutuals have only been formally recognized by the public administration as associations, in accordance with the law on freedom of association.
Against this background, the pilot phase of coverage for the poorest people was implemented through an agreement between the CNAMU and NGOs supporting mutuals, in October 2019. The CNAMU has thus signed delegated management agreements with the NGOs ASMADE, RAMS and APIL Burkina to ensure coverage for the poorest people in four regions of the country: Boucle du Mouhoun, Centre, Hauts Bassins and Nord. The term delegated management organization (DMO) therefore refers to these NGOs in this experiment, which rely on community mutuals to carry out the various delegated functions.
Target group
The status of the poorest population (indigence status) is defined by the decree setting out the criteria for identifying the poorest persons, adopted in September 2019. However, this decree is not very precise and defines the poorest as "a person who cumulatively meets the following criteria: being in a situation of absence or insufficiency of income; being in a situation of absence or insufficiency of aid". The initial target was to cover 70,000 of the poorest people in the four regions selected. The agreement signed with the NGOs stipulates that the poorest people covered by the RAMU must be on a list provided by the CNAMU.
In practice, the CNAMU used the social register developed by the permanent secretariat of the National Council for Social Protection (SP/CNPS), which was based on an agreed methodology for targeting vulnerable people developed in 2015 with national stakeholders and external partners, as part of transfer programmes for poor households. This register identifies 67,000 of the poorest people in the four regions involved in the pilot phase, and their coverage target was adjusted accordingly.
Since the end of 2021, the development of a Single Social Register (RSU) has been entrusted to the Ministry of Social Action. A technical secretariat (ST-RSU) has been set up with the immediate aim of redefining a methodology for targeting poor households. As a result, the list provided by the SP-CNPS will soon be obsolete, requiring a new registration process for the new persons identified in the poorest category, as well as to remove those who are no longer registered on the new RSU.
Definition of the healthcare package
As the basic RAMU scheme has yet to be adopted, cover for the poorest people is based on a healthcare package designed for that purpose and which provides for 100 per cent coverage of the fees for consultations, hospitalization, medical examinations, surgery, medicines, and so on, charged at primary and secondary public health facilities (health and social promotion centres (CSPS), medical centres/medical centres with surgical units (CM/CMA) and regional hospital centres (CHR)).
This coverage is based on the national pricing grid for professional healthcare procedures in public facilities. At the beginning of 2022, the CNAMU and the Ministry of Health undertook to draw up a list of professional procedures carried out by health professionals and a list of health products eligible for reimbursement by the RAMU. These lists should enable the content of the RAMU healthcare package to be refined and to set tariffs for health services and products, thereby determining the scheme's contribution to health funding, alongside other sources such as national and local subsidies, direct payments from households not covered and external partners.
Level and frequency of contributions
Pursuant to article 48 of Law No. 060-2015 of 5 September 2015, which provides that the State is financially responsible for ensuring cover for the poorest people, the CNAMU was allocated a budget envelope which it paid to partner NGOs based on the lists of the poorest people enrolled.
This is in fact a capitation payment, the amount of which has been set at 7,500 CFA francs per person per year, and which is intended to cover management costs and expenditure on DMO services. The agreement provides for payment of the budget by the CNAMU when the DMO sends the list of the poorest people enrolled, and the DMO must justify the resources received using a reporting template provided by the CNAMU. Coverage of healthcare expenses begins with the issue of policyholder cards, for a period of 12 months.
The CNAMU is responsible for funding the updating of the list of the poorest people or the creation of new targets. The list is updated by mutual agreement between the CNAMU and the DMO.
Delegated functions provided for in agreements
The agreement with the NGOs entrusted them with the following delegated functions on behalf of the CNAMU:
-
social mobilization of people in need
-
enrolment of the poorest people
-
purchase of healthcare services for the poorest people (Traoré, 2022)
The partnership between the CNAMU and NGOs thus distributes the overall various functions:
At the CNAMU level
-
The Fund decides on a healthcare package for the pilot phase.
-
It mobilizes the resources that it pays to the DMOs based on the lists of the poorest people enrolled.
-
The CNAMU provides or develops, jointly with the DMOs, management tools for enrolment and the technical management of memberships and benefits. The agreement stipulates that the DMOs undertake to test certain RAMU management tools if the CNAMU so requests. The CNAMU will bear the costs of the various tool tests.
-
The CNAMU is responsible for carrying out medical and administrative checks to ensure that insured persons receive effective, high-quality healthcare. However, the CNAMU may either call on the support of other bodies to carry out these checks, or delegate them entirely. In all cases, the DMO is required to undergo the various checks.
-
The CNAMU is responsible for following up the agreement. To this end, it is required to meet with the DMO at least once a month to assess the implementation of the agreement. The CNAMU may hold direct discussions with the social mutuals and their unions supported by the DMO, after receiving information from the latter.
At the delegated NGO level
-
The DMO is responsible for informing and raising the awareness of local authorities, opinion leaders and the poorest people in the locations concerned, during enrolment operations and when policyholder cards are issued. The DMO is also responsible for informing the poorest people of their rights and duties as insured persons and informing them of the different types of checks and the conditions and procedures for their medical care.
-
The DMO is responsible for enrolling the poorest people and for producing policyholder cards for each beneficiary. The form and information to be included on the card are validated by the CNAMU. The DMO is responsible for distributing the policyholder cards. It informs the CNAMU in advance of its strategy for distributing the cards and submits a detailed report on the distribution of policyholder cards to the CNAMU each month, or whenever the CNAMU so requests. The agreement requires the DMO to issue cards to insured persons within thirty (30) days of the transfer to its bank account of the funds set aside for coverage of the targeted poorest persons.
-
The DMO is responsible for signing and monitoring compliance with the clauses of the agreements with the healthcare providers, a list of which must be sent to the CNAMU and brought to the attention of the beneficiaries. It must also take all necessary steps to facilitate beneficiaries' access to healthcare services, in particular the reception and identification of beneficiaries by healthcare staff, and ensure the availability and quality of services provided by healthcare providers.
-
The initial plan provided for risks to be pooled at the CNAMU level, which was to be responsible for paying healthcare providers. However, with the CNAMU not in operation, the agreement signed in 2019 entrusted the DMO with the function of purchasing services and the risks are pooled at community mutual level.
-
The DMO is required to produce a consolidated monthly activity report for the social mutuals using a template provided by the CNAMU.
Distribution of functions under the agreement between the CNAMU and the DMOs
|
Functions |
Distribution |
|
|
CNAMU |
DMO |
|
|
Definition of the healthcare package |
X |
|
|
Agreements |
X |
|
|
Education and promotion |
X |
|
|
Enrolment, membership and renewal |
X |
|
|
Contribution collection |
Non-contributory scheme |
|
|
Resource mobilization |
X |
|
|
Pooling of risks covered |
X |
|
|
Payment of benefits |
X |
|
|
Healthcare services |
The 2015 law on the RAMU prohibits the simultaneous management of functions delegated by the CNAMU and the management of health establishments. |
|
|
Follow-up and steering |
X |
X |
2.5 Impact and lessons learned
Pending an evaluation of this pilot phase, scheduled for 2022, the CNAMU does not have reliable lists of the poorest people enrolled, nor precise data on the coverage and benefits provided by mutuals. The table below shows the status of the enrolment of the poorest people at the end of the first quarter of 2021, with only 16 per cent of those targeted receiving their policyholder card; by the end of 2021, this coverage rate was estimated at 23 per cent.
Status of enrolment and card production (First quarter 2021)
|
REGIONS |
Number of people targeted |
Number of people enrolled |
Enrolment rate |
Number of cards produced |
Number of cards distributed |
|
Boucle de Mouhoun |
44 084 |
11 146 |
25.28% |
1 835 |
814 |
|
Hauts Basins |
4 977 |
2 965 |
59.57% |
1 382 |
1 359 |
|
Centre |
15 227 |
13 491 |
88.60% |
8 859 |
8 779 |
|
Nord |
2 857 |
2 228 |
77.98% |
0 |
0 |
|
Total |
67 145 |
29 830 |
44.43% |
12 076 |
10 952 |
Source: CNAMU, 2021
The aim of this pilot phase was to test the capacity of mutuals to carry out the insurance functions delegated by the CNAMU and the relevance of the RAMU management tools, with a view to extending them nationwide and to other categories of insured persons. However, as highlighted above, this experience was hampered from the outset by the absence of a clear legal framework for mutuals, forcing the CNAMU to enter into agreements with the NGOs that support them, even though the 2015 law does not explicitly provide for the latter as delegated management structures. In addition, a number of weaknesses were noted (see below).
-
Not enough prior discussions took place, particularly on the nature of the functions delegated, the healthcare package covered and the steering mechanisms. Overall, the strategy to cover the poorest people does not seem to have been understood in the same way by all actors.
-
Mutuals are obliged to use the lists of the poorest people provided by the CNAMU and are not involved in identifying the poorest persons. However, the mutuals were quick to point out targeting errors and the fact that the lists drawn up in 2016 were obsolete. Numerous cases of death, disappearance and changes in social situation, as well as rejection of indigence status or of a person no longer being considered as being in the poorest category, were noted and influenced the enrolment results.
-
Although the agreement defines a healthcare package for the poorest people, in practice they are covered up to the limit of the services provided by the community mutuals in which they are members. The majority of these community mutuals only cover primary health care; some extend this cover to medical centres and medical centres with surgical units when such health facilities are present within their geographical area of operation. Only some mutuals located in urban centres sign agreements with secondary or tertiary institutions. In other words, cover for the poorest people has been determined based on the different mutual healthcare packages and there has been no development of a common guarantee for this group of beneficiaries.
-
The delay in the availability of policyholder cards, with some beneficiaries waiting more than a year, has led to conflicts between beneficiaries and NGOs, resulting in a loss of credibility for the latter.
-
The procedures for producing information and the mechanisms for monitoring and evaluating social mobilization, enrolment, provision and payment of benefits provided for in the agreements have not been applied. Similarly, the CNAMU has failed to carry out the medical checks provided for. In practice, the poorest people who are members of mutuals have been integrated into the pool of beneficiaries of these mutuals, without any distinction or specific oversight of benefits.
-
The production of information and the accountability of NGOs are weak, mainly due to the absence of financial and technical report templates for monitoring the agreement.
In the end, this experiment in delegated management was limited to financing the cover for the poorest people by community health mutuals, via the CNAMU, whose role was limited to that of financial backer. The mutuals have confined themselves to integrating the poorest people into their pool of beneficiaries, with no arrangements for registering and managing specific services, thus limiting their ability to monitor this specific group. Finally, the involvement of national NGOs, even though they are not among the delegated management bodies provided for in law, has helped to distort the mechanisms provided for. This intervention is also symptomatic of the weakness of the technical management of the community mutuals and their dependence on the NGOs providing support for their operation.
References
Burkina Faso, Ministry of the Civil Service, Labour and Social Protection. 2022. “Inventaire des mutuelles sociales du Burkina Faso – 2020”. ILO, Ouagadougou, March 2022.
CNAMU (Caisse nationale d'assurance-maladie universelle). 2021. "Analyse diagnostic de la mise en œuvre du RAMU". CNAMU, Ouagadougou, July 2021.
— 2022. "Plan stratégique de développement de la caisse nationale d'assurance-maladie universelle (PSD-CNAMU) 2022–2026, Version provisoire", February 2022.
PHCPI (Primary Health Care Performance Initiative). 2022. "Burkina Faso," 28 August, 2015. https://improvingphc.org/sub-saharan-africa/burkina-faso.
Solidaris. Unpublished. "Diagnostic contextualisé de la CNAMU et formulation de pistes d’opérationnalisation holistiques et multi-acteurs du RAMU". Solidaris, ILO, April 2022.
Traoré C. 2022. "Appui à la réalisation de l'étude organisationnelle de la Caisse nationale d'assurance-maladie, Rapport provisoire". ILO, Ouagadougou, March 2022.
3. Cambodia
Many countries have adopted strategies to extend social health protection to their entire population, with the objective of achieving Universal Health Coverage. However, the operability of such policies is still widely discussed and the debate on financing and operational mechanisms to cover the entire population, including households dependent on the informal and rural economy, remains open. In the early 2000s, community-based mechanisms emerged as the chosen strategy to expand health coverage in low- and middle-income countries, particularly in sub-Saharan Africa. While this approach remains widely discussed, the exact role of community-based mechanisms, their outcomes on coverage and how they may have contributed to the historical processes of developing national health insurance schemes are less known.
3.1 Overview of the national social health protection system
In tandem with economic growth, the health profile of the Cambodian population has rapidly improved since the beginning of the 21st century, as shown by several key indicators, among which include life expectancy at birth and the share of deaths caused by communicable diseases. However, the population is not yet fully protected against health risks. Out-of-pocket expenditure on health remains high at about 60 per cent of current health expenditure in 2017. Over the years, the Government has expressed a commitment to addressing this issue and engaged in the development of a social health protection system towards the achievement of Universal Health Coverage. Financial protection, as well as comprehensive, safe and effective access to health services are the two first strategic objectives of the Health Sector Plan (2016-2020).18
The National Social Protection Policy Framework 2016-2025 is the overarching policy governing social assistance and social security in Cambodia. In accordance with the 2019 Law on Social Security Schemes, the National Social Protection Council plays a leading role in the coordination, monitoring and orientation of the operation of all social security schemes.
Presently, the Cambodian social health protection landscape includes both contributory and non-contributory schemes. Under the Ministry of Labour and Social Welfare, the National Social Security Fund (NSSF) implements the social health insurance schemes for civil servants (NSSF-C) and formally employed workers in the private sector (NSSF-F). A voluntary scheme for the self-employed is planned but has not yet been operationalized. The design and operations of the NSSF health insurance schemes are guided by the new Law on Social Security Schemes adopted in October 2019. In addition, the Health Equity Fund (HEF) provides health coverage for eligible poor households and children. The Ministry of Health administers the tax-funded HEF scheme, with claims and payment verification placed under the responsibility of a semi-autonomous Payment Certification Agency (PCA). HEF has been implemented nationwide since 2015. As of 2021, 26.1 per cent of the population of Cambodia is covered by one of these schemes.19
Table 1 below summarises key information on the social health protection schemes.
|
Schemes |
Institution |
Year Established |
Target population |
Financing mechanism |
Population covered |
|
Health care for private formal employees (NSSF-F) |
Ministry of Labour and Vocational Training/ National Social security Fund |
2017 |
Employees (Persons defined as such by the provisions of the Labour Law) |
Mandatory contribution20 |
1,241,035 (2021)21 |
|
Health care for civil servants and dependents (NSSF-C) |
Ministry of Labour and Vocational Training/ National Social security Fund |
2017 |
Persons employed in the public sector |
Mandatory contribution |
292,295 (2021)22 |
|
Health insurance (HEF) for the poor and Children |
Ministry of Health |
2007 |
The poor, persons with disabilities, the elderly, children < 5 |
Exempt from user fees at health facilities; funded by Government and with support from Development partners |
Approx. 2.8 million (2021) |
Overall, there has been remarkable progress in the development of the social health protection system with regard to achieving set goals. Despite this progress, more than 70 per cent of the population have no access to social health protection in Cambodia. One of the main challenges is extending coverage in the context of widespread informal employment and limited government resources. The diversity of employment relationships, income levels and patterns of workers in informal employment, compounded by the lack of sectorial data and research are the current obstacles to designing possible strategies faced by policy makers. The Government is currently working on the development of strategies to address coverage gaps and is particularly focused on a Universal Health Coverage roadmap as well as an integrated strategy for formalization.
Moreover, options to extend coverage to workers in informal employment are being tested. In 2017 the Ministry of Economy and Finance (MEF), the Ministry of Health (MoH), and the Ministry of Labour and Vocational Training (MoLVT) issued the inter-ministerial Prakas 404 on the “Implementation of the health care scheme through Health Equity Fund system for informal workers […].” This joint legal directive extended coverage, through the HEF, to a relatively small number of informal workers defined as part-time, seasonal, and casual workers. In addition, the NSSF is currently implementing the first phase of piloting the extension of coverage to domestic workers (under the mandatory scheme) and to Tuk Tuk drivers under a voluntary pilot scheme, with the support of French NGO, GRET (Professionals for Fair Development).
Prior to this, from the 2000s to 2018, Cambodia implemented CBHI in an attempt to pilot financial protection mechanisms addressing immediate needs for coverage, while informing broader decision making regarding the architecture of the national social health protection system. This mechanism provided financial health protection to low-income households in selected provinces. There were up to 19 CBHI schemes in the country, the details of which are provided in Section 2. These schemes were run by non-governmental organisations and supported by development partners. An analysis of the CBHI experience in Cambodia, particularly regarding how it has contributed to building the current social health protection system, and its successes and failures, can provide useful insights for designing policy options to extend coverage to workers in informal employment.
3.2 Community Based Health Insurance (CBHI)
History
CBHI schemes were established as pilot mechanisms for risk pooling for health care, based on pre-payment. CBHI schemes were private non-profit insurance schemes and were all operated as local or international NGO projects, in the absence of a legal framework.
CBHI was first piloted in 1998 by GRET through an experimental rural health insurance project in two Cambodian provinces, namely Kandal and Takeo. The project was known as SKY, which is an acronym for “Health for our Families” or Sokhapheap Kruousa Yeoung in the Khmer language. The idea of offering low-cost health insurance emerged from the observation that non-repayment of micro-finance loans was often caused by catastrophic health spending. Therefore, the objective was to protect low-income rural households against severe health expenses.23
In the late 1990s, Cambodia remained one of the poorest countries of East Asia, with 35 per cent of the population living below the poverty line. The country was predominantly rural but faced a rapidly growing urban sector, and a widening disparity of incomes. The informal sector represented around 90 per cent of the labour force. To finance their health costs, 80 per cent of Cambodians used savings, got into debt or sold assets.24 In the year 2000, health costs were mainly financed by out-of-pocket payments, which accounted for 68.7 per cent of health expenditure.25
Beyond the initial two provinces, the GRET-SKY scheme extended its coverage to additional districts. Later on, more CBHI schemes were introduced in various parts of the country by local NGOs. These local NGOs, such as Buddhism for Health (BFH), Reproductive and Child Health Alliance (RACHA), Cambodian Health and Human Rights Alliance (CHHRA) and the Cambodian Association for Assistance to Families and Widows (CAAFW), were contracted by MoH, following a bidding process, to operate CBHI in specific districts and provinces, alongside HEF in most cases.
In 2008, MoH reported that 12 CBHI schemes were operational in seven provinces and one municipality, with 11 Operational Districts and 81 Health Centers, and with membership of over 80,000 (See Annex 1). In the same year, the percentage of CBHI coverage of Operational District (OD) population ranged from the 0.49 per cent in Kirivong OD to 19 per cent in Thmar Pouk OD by 2013, at its peak, providing insurance coverage to 455,000 persons in 27 ODs in 11 provinces, representing slightly more than 3 per cent of the total population of Cambodia.26
Design
Building on the GRET-SKY pilot and due to an increase of CBHI schemes in Cambodia, MoH acknowledged a need to regulate these schemes and thereby adopted and operationalized guidelines for Implementing CBHI in 2006.27 MoH provided guidance on the scheme design, arrangements and operations, and set harmonized rules with regard to the administrative and technical requirements and common benefits, aiming at future portability between different CBHI schemes. With the implementation of the guidelines, all CBHI schemes followed a very similar design and operational modalities.
Governance model
Under the contracting model, local NGOs were in charge of all the management and operational functions inherent to CBHI schemes and reported on their activities and achievements to MoH.
According to the guidelines, CBHI involved several key stakeholders:
-
MoH and its subsidiary departments and units (Department of Planning and Health Information, and Bureau of Health Economics and Financing
-
Social health insurance committee
-
Provincial health departments and operational districts
-
Health care providers, including national hospitals, referral hospitals and health centres
-
CBHI consultative committee, including consumer and patient associations and population representatives
-
CBHI Steering Committee
-
CBHI implementer
-
CBHI scheme supporter/funder
Eligibility and Registration
Registration was open to everyone, without restrictions based on pre-existing disease or age. Coverage was conditioned by payment of premiums, paid in advance on a monthly, quarterly or annual basis. Most members were low-income individuals, as the poor could not afford contributions and the better off were more interested in private insurance covering private facilities.
Enrolment to CBHI was voluntary but household based, to mitigate pitfalls associated with voluntary enrolment and to cover a larger share of the population, as well as to limit the risk of discrimination within households and reduce adverse selection.
Through the SKY pilot scheme, registration was open throughout the year and promotion was conducted every first week of the month in all districts where SKY was operating. The insurance policy was subscribed to for a 6-month cycle. Households paid their premium on a monthly basis, before the 20th of each month to be covered from the 1st of the following month. For new families registering, an additional two months of premium were required as reserves, which could be used in the cycle in case of payment difficulties.28
Within the objective of the Health Strategic Plan 2008-2015 to improve health outcomes for the entire population and reduce out-of-pocket spending, MoH encouraged combining SHI, HEF and CBHI schemes, with the ultimate objective to bring all schemes under a common social health insurance umbrella.29 30 31 Contributions of HEF members were covered by government subsidies and donor support.
Revenue of CBHI
CBHI revenues originated from members’ contributions (premium payment) and donor support. According to the CBHI guidelines, premiums were calculated taking into account the following elements:
-
official user fees schedule
-
capacity of target population to pay
-
operational cost of CBHI scheme
The guidelines set out that premiums should be set at an affordable level, particularly for large families and that these rates should be adapted to the family’s location (different rates for urban and rural areas to be calculated) and the economic environment. In practice, several design features were tested to improve financial accessibility. These included degressive premium rates for longer registration duration, a lucky draw for free months of coverage, a higher subsidy level at first registration with decreasing subsidy levels over time and so on. Degressive per capita rates were also applied for large families to facilitate their enrolment. When extension was tested in formally registered enterprises, such as hotels, employers paid at least 50 per cent of the premium, with the remaining 50 per cent being paid for by the insured members. Revenues from contributions were not sufficient to finance medical and operational costs, and the financial support of development partners remained essential to ensure the implementation of the CBHI schemes.
Benefit package
The CBHI benefit package was defined in the guidelines in accordance with the health systems service delivery. As such, a Minimum Package of Activities (MPA) at health centre level and a Complementary Package of Activities (CPA) at referral hospital level (CPA1, CPA2 or CPA3 depending on the level of the referral hospital) provided the basis for the benefit package. Within the MPA and CPA definitions, all insured family members were entitled to medical care, pharmaceuticals and medical supplies, health education and prevention and non-medical benefits. The benefits are summarized in the table below.
Table 2. Summary of Medical care, Pharmaceuticals and medical supplies, Health education and prevention and Non-medical benefits
|
Medical care |
Pharmaceuticals and Medical Supplies |
Health education and prevention services |
Non-medical benefits |
|
|
range of services as agreed between CBHI implementers and health care providers and adapted to specific needs of the target populations |
Inclusion of transport between health facilities or residences, grants for funerals or maternity cash allowance as defined by MoH |
The guidelines also specified conditions excluded from the benefit package, which usually comprised advanced procedures and operations such as organ transplants, infertility treatment or non-essential interventions such as cosmetic and aesthetic treatments.
Below is an example of the SKY Benefits package.32
-
Access to primary health care at health centre level including prescribed drugs;
-
Access to specialized out-patient consultation and para-clinic tests (laboratory, ultrasound, X ray and so on) at district and provincial level, after referral;
-
Hospitalization stays with drugs and all related para-clinic tests, after referral;
-
All ante and post-natal care, including simple and complicated deliveries after a waiting period of six months;
-
Grant for member funeral expenses (ranging from US$12 to US$24 in rural areas and US$60 in urban areas), and body transportation costs;
-
Emergency transportation grant of US$5;
-
No ceilings applied and pre-existing diseases were covered by the scheme.
Provider network, contracting and payments
Members could access these services, without co-payment at the point of service, at contracted health facilities, usually including all public facilities in their catchment area, from health centres to provincial hospitals. Compliance with the public referral system was a condition for health care services to be covered at a higher level of care.
MoH’s CBHI guidelines set out that the CBHI Implementer shall pay the main contractor to cover the health care costs of all insured members in the contracted network of health care providers, based on mutually agreed contracts, witnessed by the CBHI Steering Committee.
As shown in Annex 1, payments to health centres and first referral hospitals contracted for CBHI were mostly capitation based, whereas payments to secondary hospitals (with more comprehensive services such as CPA2 or 3) were case based. Payments to facilities were prospective, and paid a quarter in advance to health facilities. Potential financial risks, defined as the difference between the capitation paid and the amount the facility would have received if paid on a fee-for-service basis, were covered by the CBHI scheme for a period of time agreed in the contract. This third-party payment facilitated the provision of better financial protection to members, as they no longer had to borrow money or sell their assets to pre pay for health care.
Details of CBHI regulations as per the 2006 MoH guideline for the implementation of CBHI, are summarized in the table below:
Table 3. Details of CBHI regulations
|
Function |
Details of delegated function |
|
|
Population coverage |
In principle, CBHI could cover anyone recorded in the Cambodian Family book. Importantly, as the NSSF was being developed in parallel, CBHI was mostly targeting households relying on the informal economy. |
|
|
Design |
Benefits package definition and levels |
Benefit package was defined as per guidelines, including health services as well as non-medical benefits (transportation cost upon referral or from home to health centre as well as funeral grant, maternity grant or other forms of grants). Guidelines introduced a gatekeeping mechanism at primary care level. |
|
Provider networks |
CBHIs had to establish their own contracts with providers within their networks, according to a pre-defined model for contracting proposed in MoH guidelines. |
|
|
Implementations |
Education / Promotion |
CBHI was responsible for organizing health promotion and prevention activities in collaboration with health care provider. |
|
Enrolment / Renewal |
Enrolment was household-based and conducted by the CBHI. Dependents of a CBHI member were those listed in the Cambodian Family book. |
|
|
Revenue collection (if applicable) |
Revenue collection was undertaken at CBHI level. The main source of revenue was the contribution from members. Alternative sources of revenues could be: Donations from individuals or local organizations Funds from international agencies Special activities organised by the scheme Contributions by social assistance schemes organised by the government, by donors or by organisations (e.g. Equity Funds) |
|
|
Pooling |
Pooling of the various revenue sources was implemented at CBHI level. |
|
|
Purchasing |
Provider payment was defined at CBHI level, with guidelines authorizing a mix of the following payment mechanisms: Capitation Reimbursement of fees for service Case based payment Use of the capitation system for paying primary and secondary health facilities was strongly advised. |
|
|
Provision |
CBHIs did not own providers. |
|
|
Claim management and reimbursement |
Members could access these services, without co-payment at the point of service. In case of genuine emergency, insured family members could use nearby public hospitals services, but had to report to the hospital they were affiliated to, through the CBHI Implementer, within 48 hours. |
|
|
Feedback mechanisms (quality assurance) |
CBHIs had to develop a quality assurance framework, using the existing MoH standards for health providers as minimum criteria. The MoH guidelines formulated a procedure for grievances and appeals for all CBHI beneficiaries. The MoH guidelines proposed a framework for performance measurement (Key Performance Indicators). However, the CBHI schemes were responsible for developing their own monitoring formats. Some schemes carried out patient exit surveys as well as member satisfaction surveys to measure satisfaction, and to provide knowledge on insured benefits and procedures. Results were used to adapt communication messages as well as possible revision of the benefit package. |
|
From CBHI to mandatory contributory social health protection
Discussions on social health insurance began in 2005, with the creation of the inter-ministerial committee on Health Insurance known as the Social Health Insurance Group, which was chaired by an MoH secretary of state. A technical subcommittee of the group comprising ILO, WHO, GTZ and GRET met regularly to discuss SKY CBHI experiences and the global approach to social health insurance. 33
Experiences from CBHI, as well as regulation efforts such as the MoH guidelines, provided a prototype for the design and operationalization of the NSSF health insurance scheme. Practices and lessons learned during the implementation of CBHI on the definition of the benefit packages, provider payment mechanisms, contracting with health facilities, claim verification and payment, in addition to management tools such as the development of information system and complaint management systems, were foundational to the development of the health insurance scheme of the NSSF.
A pilot Health Insurance Project (HIP) for garment sector workers was launched after a feasibility study in 2007 under the initiative of the Garment Manufacturers’ Association of Cambodia (GMAC) and GRET in collaboration with NSSF and the MoLVT.34 The transfer of the HIP project from GRET to NSSF under the MoLVT started in 2013. The HIP team contributed its expertise, acquired through the SKY CBHI scheme, to the establishment of the national scheme for formal sector workers. The experience and insights were essential to the design and arrangements of social health insurance schemes. In particular, the pilot phase was useful for fine tuning operational processes, health care provider payment mechanisms, client centred complaints management and a computerized monitoring and information system (MIS), and to build evidence on the cost of the system based on health care consumption analysis. For instance, the MIS was designed and developed with a modular approach, allowing each scheme (CBHI, HEF and SHI for workers in formal employment) to monitor membership, contributions and claims payment. As the CBHI scheme was piloting several design features on contribution, the MIS was adapted to cater for these characteristics. For instance, the premium could be recorded based on various options of periodicity of payment, with or without various premium discounts policies, and so on. The MIS was built with several functionalities aimed at facilitating data management and daily management of the schemes. For instance, some functions included automatic generation of frequently needed reports, KPI reports, automatic flags detecting unusual data patterns, and so on. The SHI module is still being used by the NSSF, alongside the further development of the system.
In January 2016, the Prime Minister of Cambodia issued a sub decree launching the mandatory SHI scheme for formally employed workers. The sub decree sought to implement the health insurance branch of the 2002 Social Security Law.
Prakas No. 109 of 2016 defined the benefit package to be provided by the NSSF, which included preventive services, with exclusions According to the Prakas, the 16 excluded medical services are: 1) free medical treatment stipulated in public health policy; 2) dental care (cleaning, filling, crown or bridge); 3) treatment and sex transsexual surgery; 4) organs transplantation (bone marrow, kidney, liver, and pancreas); 5) artificial insemination in case of infertility; 6) self-treatment; 7) cosmetic surgery and medical implants; 8) contact lens and eye-laser treatment; 9) treatment of alcoholism or drug abuse; 10) infertility treatment; 11) artificial globe ocular operation; 12) cardio vascular surgery; 13) chronic diseases; 14) haemodialysis; 15) thalassemia; and 16) chemo therapy for cancer treatment. Prakas No. 220 of 2016 specifies the contribution rates for the SHI scheme, set at 1.3 per cent of the employee’s salary for both employers and employees.
3.3 Impact of the CBHI
This section aims to document impacts and results of the CBHI experience in Cambodia as documented by various sources and development partners. Although CBHI schemes ceased to exist after 2018, and NSSF schemes have replaced them in in Cambodia to provide health insurance for workers in formal employment, the legacies of CBHI schemes remains, which have been essential in designing and operating NSSF schemes. The successes and failures of the CBHI experience are important to guide future decisions and for developing policies on the extension of coverage to those currently uncovered.
CBHI impacts in terms of population protected
One main lesson of the CBHI scheme experience in Cambodia is that a voluntary enrolment model with limited subsidies does not allow for the achievement of significant population coverage. Enrolment rates remained low, with CBHI schemes reaching a peak in 2013 when the total membership reached 455,600 from 19 schemes (in 11 provinces, contracting with 240 health centres and 27 referral hospitals). This amounted to slightly over 3 per cent of the whole population in the country.35
From 2014, the membership started to drop drastically, partly due to decreased subsidies by CBHI donors and several other factors presented below. By the end of 2015, all CBHI schemes had a total of 148,418 members, representing less than 1 per cent of the total population of Cambodia, and by 2017, membership dropped further to just over 22,000.
Table 4. CBHI scheme basic overview
|
Scheme |
Institution |
Year established |
Population eligible |
Financing mechanism |
Population covered |
|
CBHI* |
NGOs |
2008 |
Open to all, but mainly near-poor households |
Voluntary (pre-payment) + donors support |
455,000 (2013); 66,487 (2016); 22,013 (2017) |
* Source: Cambodia Ministry of Health, 2018. Report on Achievements of 2017 and Plans for 2018.
It is important to note that population coverage remained low despite significant efforts to implement a dynamic and proactive outreach system. For instance, GRET-SKY had a large network of agents in the field. Organized through a private not- for- profit structure, the project implementation relied on task sharing between the head office and field teams. While technical functions related to insurance were centralized in the head office, the field team facilitated a high level of proximity with members and a close relationship with health providers. Therefore, a large network of agents was in charge of promotion, premium collection and enrolment of new members. Premium collection took place through door-to-door visits and village awareness meetings, and various marketing strategies were implemented to boost enrolment. Community participation was achieved through the insurance consultative group.36
The voluntary nature of the scheme, together with the irregular and unpredictable income that most workers in the informal economy faced, led to high monthly drop out rates, exceeding 5 per cent.37 This was compounded by the limited quality of health care provided by public health facilities in Cambodia, limiting the attractiveness of the schemes.
CBHI impacts in terms of financial protection
An impact evaluation of SKY CBHI indicated that the scheme had a positive economic impact in terms of savings, care expenditures, asset retainment and indebtedness. The impact assessment showed that the insured members were 10.8 percentage points less likely to experience a large economic impact such as taking on new debt due to a health shock.38
As part of the same impact evaluation, a study by Domrei Research and Consulting reported savings of US$665 (median) in terms of gold, cash and liquid assets (rice, poultry and so on) among households enrolled in the SKY CBHI scheme.39 However, it was not clear if there was a significant difference in terms of the amount of savings between scheme members and non-members.
An impact study commissioned by GTZ in Kampot40 found that scheme members overall spent less on health care than non-members, and they were less likely to have health expenditures greater than US$250, and experienced lower costs when they did seek private care. Members were also less likely to pay for the costs associated with health shocks through the sale of assets and taking out loans with interest. Micro health insurance coverage also had a positive impact on debt; on average, scheme members had US$70 less debt, and a lower total value of all health-related loans.
CBHI impacts in terms of access to health care
The impact assessment mentioned above also analysed the effects of the SKY CBHI scheme and found that it changed health-seeking behaviours, increasing the use of covered public facilities and decreasing the use of uncovered private care for major illnesses. It also showed that SKY reduced rates of forgone care due to lack of funds: insured households were 4.1 percentage points less likely to forgo care compared to the control mean of 5.2 per cent.
Additional evidence pointed at an increased utilization of health care services for members covered by CBHI. In Ang Roka and Khampong Thom Districts, utilization rates at contracted health care centres were much higher for insured members than the general population, at 3.6 visits per person per year in 2006, 3.2 in 2007, and 2.1 in 2008. This demonstrates a much higher attendance than the national contact rate of less than one visit per person per year, and a decrease of over-consumption over time. The same study shows that CBHI contracting public facilities contributed to channelling patient flows towards these structures and away from self-medication and private practitioners. Indeed, in these two districts, the use of public health care was higher for CBHI SKY members than the national average of 21 per cent. 41
GIZ’s report42 on the evaluation of SKY CBHI in Kampot OD, also citing the impact evaluation carried out by Domrei Consulting with US Berkeley, indicates that scheme members had a higher rate of utilization of contracted health facilities than private clinics or drug sellers.43 This was partly due to monitoring of health service provision which was more or less affected by providers’ behaviours. In addition, linkages between CBHI and HEF enabled a much higher utilization of services from HEF, compared to the HEF traditional model. The impact study could not show that membership had a detectable effect in terms of health outcomes,44 as expected, due to low statistical power.
Financial viability of the scheme
Most CBHI schemes could finance health facility claims and payment of other benefits from the revenues generated by the premiums collected. However, they remained highly dependent on grants paid by development partners for financing schemes’ operating costs. For instance, SKY charged a premium of US$5 per person per year in rural areas and had reached an initial level of sustainability, in that all medical costs and additional benefits paid to its members were fully covered by the premium collected, thanks to risk pooling across the different regions covered. However, operation costs were only partially covered. In 2009, the total annual costs for providing SKY insurance to one member stood at roughly US$14.7. One third of the costs came from claims, and two thirds consisted of operational costs. The contribution collected only allowed coverage of one third of the total costs.45
Despite financial performance steadily improving, achieving overall financial equilibrium was still out of reach and would have required a significant scale up to reach economies of scale.
CBHI schemes in Cambodia faced a host of challenges in ensuring their financial viability, due to the following reasons:
-
Limited revenues and limited risk sharing. The initial actuarial calculation of the premium for the SKY CBHI scheme did not fully include operational costs, as they were assumed by externally funded sources, creating a virtual subsidy to support the overall functionality of the system. Scheme premiums were kept low so as to be affordable to low income rural households. Most members were from such households, relying on jobs in informal employment for their living, often in the agriculture sector, where income is irregular, and unpredictable. This was compounded by voluntary enrolment, which is not conducive to the continuation of membership in a context of low income and competing priorities, such as food and schooling. This translated into low revenues for the scheme, limited risk pooling and a lack of redistribution mechanisms within the schemes.
-
Costs exceeding revenues. The benefit package was designed to be quite comprehensive, with a mix of preventive and curative services, from primary to tertiary level and an absence of co-payments at the point of service, so as to maximize financial protection of households. In addition, the operational costs were high compared to the premium collected, due to a proactive promotion and contribution collection model, with a large network of agents in the communities, so as to increase coverage.
-
Limited attractiveness of public facilities. Provision of benefits from public health facilities was not attractive to the well-off and to some extent to near-poor households due to the perceived low quality of, and lack of trust in public health services. Some initiatives to improve care quality required additional resources, as reported in the case of the Angkor Chum Scheme in Siem Reap province.46
-
Poor health and awareness of financial risk key motivating factor for enrolment among near-poor households. Although no clear adverse selection among most of the scheme members was observed, in the case of the SKY CBHI scheme, near-poor households with knowledge of potential needs for health care, the cost involved and fear of indebtedness, were likely to enrol in schemes, and poor health in the family was among the primary motivators for joining a scheme.47
The 2017 MoH report indicates that CBHI based solely on the collected premiums and without extra financial support was not sustainable in the intermediate and long term. Ultimately, the end of external funding created a resource gap that necessitated a premium increase. The increase exceeded enrollees’ willingness to pay, which undermined the solvency of the scheme. This occurred at a time when most of the schemes had limited membership and had not reached a level enabling economy of scale.
3.4 Conclusion
Historically in Cambodia, CBHI schemes played a role in improving financial health protection for their members in the absence of any other social health protection mechanisms available. However, the experience illustrates that voluntary CBHI is not conducive to the coverage of a significant share of the population, even when the premium is partially subsidised (through donors’ funds and the provision side in this case). Operationalized in a fragmented manner (several operators), and targeting low income households only, it prevented effective risk pooling.
After a few years of operation, the guideline developed by the MoH translated the State’s attempt to start regulating and harmonizing the offer of CBHI schemes throughout the national territory. While most of the social health protection and insurance functions were left for the CBHI to ensure independently, the guidelines set a defined, harmonized benefit package and created common tools for contracting providers and monitoring. Despite these harmonization efforts, and due to design limitations highlighted above, CBHI could not replace a government-steered, national social health protection system based on mandatory enrolment.
Therefore, in Cambodia, the CBHI experience served as a learning opportunity on the design of social health protection in terms of population coverage, adequate benefits and financial protection. It also allowed for the testing of a range of pragmatic approaches to operationalize the schemes, and address the particular needs of low income households, mostly dependent on the informal economy for their livelihoods. The community approach allowed for the development of the necessary knowledge on the needs and characteristics of members, particularly income level and patterns, and facilitated the development of registration and contribution collection strategies accordingly. It contributed to testing and developing management tools, which are still in use today under adapted forms, such as the MIS, complaints management system, provider contracts with bonuses for performance, and so on. Today, the achievements of the NSSF still partly rely on the legacy of CBHI, among other schemes.
References
Both, N., Evans M., Thewissen S. et Ramírez López B. (2017). Policy Brief. Extending social protection to informal workers in Cambodia. Genève: OIT.
Cambodge, ministère de la Santé, direction de la planification et de l’information sanitaires (2006). Guideline for the implementation of community-based health insurance (CBHI).
Cambodge, ministère de la Santé (2008). Health Strategic Plan 2008-2015.
— (2008). MOH Health Financing Report.
— (2008). Strategic Framework for Health Financing 2008-2015.
— (2014). MOH Report on Achievements in 2013 and Plan for 2014.
— (2018). MOH Report on Achievements of 2017 and Plans for 2018.
— (2020). MOH Report on Achievements 2019 and Plan for 2020.
Cambodge, ministère du Travail et de la Formation professionnelle (2018). NSSF Report on Achievements 2008-2017 and Action Plan 2018.
Cambodge, ministère du Travail et de la Formation professionnelle, ministère de l’Économie et des Finances et ministère de la Santé (2017). Inter-ministrial Prakas on implementation of healthcare scheme through health equity fund system for informal workers and provision of additional allowance for female workers when delivery.
GIZ (2011). Impact of an integrated social health protection scheme in Kampot, Cambodia, 2008 to 2010, 2011.
Japan International Cooperation Agency, JICA (2016). «Survey on the social health protection system in Cambodia».
Levine, D., Polimeni R. et Ramage I. (2011). «Insuring health or insuring wealth? An experimental evaluation of health insurance in rural Cambodia», Journal of Development Economics 119, mars 2016.
Levine, D., Polimeni R., Ramage I. et Searles P. (2010). Who buys SKY health insurance? AFD, Université de Californie à Berkeley, Domrei Research and Consulting.
Levine, D. (2009). Innovations in insuring the poor. Health insurance for the rural poor: Evidence from Cambodia. 2020 Vision Focus. Washington: International Food Policy Research Institute (IFPRI)
Organisation internationale du Travail, OIT (2008). Cambodia: SKY Health Insurance Scheme. ILO Series: Social Security Extension in East Asia Initiative. Bangkok: Bureau sous-régional de l’OIT pour l’Asie de l’Est.
— (2018). Extending National Social Security Fund coverage to informal workers in Cambodia (the cases of domestic workers and Tuk-Tuk drivers).
Organisation mondiale de la Santé, OMS. (2015). «The Kingdom of Cambodia: Health System Review», Health Systems in Transition 5, no 2.
Por I., Men C.H. et Sour I. (2011). Impact evaluation of community-based health cooperative in Bakan Operational District. Phnom Penh: Reproductive and Child Health Alliance.
Parliamentary Institute of Cambodia (2019). «National Social Security Fund in Cambodia: Background for Field Mission to Prey Veng, Svay Rieng, Tboung Khmum and Kampong Cham Provinces». Briefing note.
Sachiko O. et Walker D. G. (2009). «Trust in the context of community-based health insurance schemes in Cambodia: Villagers’ trust in health insurers», Advances in Health Economics and Health Services Research, 132(21), 107-132.
4. Colombia
4.1 Background
Colombia radically reformed its SHP system in 1993. Law No. 100, enacted that year, created the General System of Social Security in Health and made it possible to achieve UHC. The General System of Social Security in Health has a contributory scheme, covering formal workers and retirees, and a subsidized scheme, covering the poor and vulnerable. There are also special schemes.
The aim of this reform was to correct the failings of a health system that was suffering from problems of access and quality - only 24 per cent of the population was covered – and which was also unjust, as it covered 47 per cent of the population in the richest quintile, but only 4 per cent of the population in the poorest quintile. The system's lack of fairness was also reflected in the proportion of healthcare expenditure borne by households, which was higher for the least well-off families: in 1993, households bore 44 per cent of current healthcare expenditure
Before Law No. 100, the public health insurance system was administered by the Social Security Institute for private-sector employees, and by provident funds for civil servants. The Ministry of Health provided healthcare for the population not covered by social security. The private health insurance system covered the population with the financial means to pay. Law No. 100 made health insurance compulsory for the entire population and delegated the enrolment of users to insurance bodies called "health promotion entities" (EPS) and the provision of healthcare to "healthcare provider institutions" (IPS), with the EPS and IPS often being part of the same economic units. These entities have different legal statuses, some of which are mutual in nature.
The current SHP system depends on the following stakeholders: (a) the Ministry of Health and Social Protection, which is responsible for coordination, management and oversight; (b) the EPS, which act as insurers and collect contributions; and (c) the IPS, which are healthcare establishments such as public or private hospitals, clinics, doctors' surgeries and laboratories.
Other bodies are involved in the governance and administration of the system. The Entidad administradora de los recursos del sistema general de seguridad social en salud (ADRES), which is attached to the Ministry of Health and Social Protection and has administrative and financial autonomy, is responsible for administering the resources of the general health social security system. It is responsible for paying "capitation payment units" (UPC) to the EPS. It is also responsible for administering the single database of members (BDUA).
The National Health Authority is responsible for inspecting, monitoring and overseeing the general social security health system and for protecting users' rights. Lastly, local authorities (municipalities, districts and departments) play an important role in identifying and enrolling poor or vulnerable households, in financing insurance for these people and in monitoring and overseeing effective access to healthcare.
4.2 The national social health protection system
The EPS are responsible for enrolling insured persons under the contributory and subsidized schemes, for which they provide a healthcare package imposed by the State. The contributions collected under the contributory scheme are transferred to the ADRES, which pools them with other tax resources earmarked for health insurance. The ADRES then redistributes to the EPS an amount per insured person (capitation), in other words the UPC. The UPC is adjusted according to age, gender and geographical area. It is an advance payment from which the EPS must cover all the costs of healthcare for insured persons included in the healthcare package. Since 2012, the healthcare package for the subsidized and contributory schemes have been harmonized, although the UPC is not the same for the two schemes. In addition to this payment, an amount is paid for the provision of services and the dispensing of drugs excluded from the healthcare package
Membership of the General System of Social Security in Health is compulsory for all inhabitants in Colombia
The contributory scheme is funded by contributions from employers (8.5 per cent of salary), employees and retirees (4 to 12 per cent, depending on the level of salary or old-age pension) and the self-employed (12.5 per cent of declared monthly income). Since the 2019 tax reform, the contribution rate on retirement pensions has been reduced from 12 to 4 per cent for income up to one minimum wage and to 10 per cent for income up to two minimum wages to make way for greater state funding
The subsidized scheme is funded by the tax revenue transfers from the State, departments, districts and municipalities 48 and by a 1.5 per cent levy on contributions to the contributory scheme. The subsidized scheme also receives a solidarity contribution from people who are neither poor nor vulnerable 49 and who are members of the subsidized scheme if they do not meet the conditions for membership of the contributory scheme. The solidarity contribution rate is determined according to socio-economic level and varies between 2.5 per cent and 11 per cent of the primary capitation unit of the subsidized scheme. The scheme is also financed by taxes on tobacco, alcohol and lottery games; these taxes were increased substantially in 2010 to finance the harmonization of the benefits package, the universalization of health insurance and other sector needs
The government steers the SHP system through the Ministry of Health and Social Protection and pools funds via the ADRES. It delegates the management of front-office insurance functions to the EPS and healthcare services to the IPS.
The Plan de beneficios en salud (formerly the Plan obligatorio de salud) is the healthcare package available to people insured under the General System of Social Security in Health and financed by the capitation payment unit
The healthcare package is now identical for members of the contributory scheme and the subsidized scheme. However, not everyone has access to the same quality of service, which varies depending on where they live and the skills and facilities of the IPS belonging to the healthcare network of the EPS of which they are a member
The contributory scheme provides for out-of-pocket expenses and co-payments, the values of which were revised by Decree No. 1652 of 2022. The amount of these co-payments varies depending on the insured person's income. The co-payment represents between 11.5 and 23 per cent of the amount of the benefit, for example. Out-of-pocket expenses and co-payments are mutually exclusive, in other words they cannot be combined for the same benefit. Out-of-pocket expenses or co-payments are not applied to health promotion, initial consultations, maternal and perinatal health, health education and the treatment of notifiable communicable diseases such as dengue fever, hepatitis and sexually transmitted diseases.
Beneficiaries of the subsidized scheme do not pay out-of-pocket expenses, but must make a co-payment set in 2023 at 10 per cent of the treatment cost. In both schemes, the insured person's contribution is subject to a ceiling per episode of care and an annual ceiling.
As far as cash benefits are concerned, only members of the contributory scheme are entitled to daily sickness or maternity allowances.
Care is provided through healthcare networks organized by the EPS. The EPS sign contracts with the IPS (hospitals, health centres, laboratories, independent health professionals and health transport services) and medical technology providers, and pay for them.
In order to receive healthcare, insured persons must join an EPS, which they are free to choose
The EPS enter into contracts with healthcare providers (IPS), which they pay through a range of methods: payment per case, advance general allocation, payment by capitation or per episode of care. They are also responsible for designing the referral and counter-referral system and are required to set up a network of providers who guarantee the availability and adequacy of services at all levels of care.
In June 2022, a total of 11,466 IPS were State-approved nationwide. Some EPS have their own IPS, but cannot allow them to undertake more than 30 per cent of the services.
4.3 Delegation features
Solidarity based health companies and their role as health promotion entities in the SHP system
The Colombian social security system offers users the possibility of grouping together to manage health insurance collectively via mutuals or cooperatives known as "solidarity-based health companies" (ESS), approved associations or even entities promoting the health of indigenous communities (EPSI). Each of these entities plays a different role in the SHP system.
Solidarity-based health companies (ESS) were created in 1993 as a form of community health risk management designed to facilitate access to healthcare for the poorest and most vulnerable sections of the population
With the implementation of the General System of Social Security in Health, the solidarity-based health companies became management organizations for the subsidized scheme, acting as insurers and care provision organizers. The ESS had increased their market share in the early days of the reform and had come to insure 30 per cent of insured persons under the subsidized scheme, before their numbers dwindled as a result of regulatory constraints and stricter supervision of their operations. Of the 183 ESS authorized to operate in 1998, only 80 remained the following year
The ESS currently operate in the same way as other EPS under the subsidized scheme and are monitored by the National Health Authority. Their funding is governed by the rules set out for the EPS in the subsidized scheme. They receive UPC.
Health promotion entities of indigenous communities and their role as EPS in the national SHP system
The EPSI, set up by indigenous organizations, have a remit to cover indigenous peoples and other beneficiaries of the subsidized scheme
Group membership of health insurance via cooperatives and other entities grouping self-employed workers
In addition, self-employed workers have the option of joining health insurance collectively as members of an association, professional organization or religious congregation approved by the Ministry of Health and Social Protection
Approved associations are not insurers. They are intermediaries who take responsibility for the collective membership of self-employed workers of an EPS under the contributory scheme. This type of membership is governed by Decree No. 3615 of 10 October 2005 and Decree No. 2313 of 12 July 2006. Associations must guarantee their members a free choice of EPS
Delegated functions
|
Function |
Delegation |
|
Design |
|
|
Population coverage |
The entire population is covered by the law, which was decided centrally by the State. Mutual benefit societies are delegated to manage the scheme, not to design it. |
|
Definition of services |
All EPS, including ESS and EPSI, are required to provide the package of benefits determined by the Ministry of Health, which includes emergency care, consultations, hospitalization, specialist care, medications, dental care, mental health care and palliative care, provided that they are not on the list of exclusions updated every two years |
|
Network of service providers |
The network of providers is decided by each EPS, which must select its network from among public and private healthcare providers (IPS) recognized by the Ministry of Health and Social Protection and the National Health Authority. EPSI also provide services through indigenous IPS, which have an intercultural approach to care |
|
Implementation |
|
|
Education/Promotion |
Pursuant to article 162 of Law No. 100, the protection offered by the compulsory healthcare package begins with health promotion and prevention. Thus, all EPS, including ESS and indigenous EPS, are required to implement health promotion measures Among the services offered by EPS are programmes designed to encourage self-management and disease prevention. |
|
Membership |
The role of EPS is essentially that of insurers, while that of ESS and EPSI is more specifically to enrol the poorest and most vulnerable people in the subsidized scheme. |
|
Collection of contributions (or other resources) |
The role of EPS is to collect contributions and pay them to the ADRES, which is responsible for pooling them with other tax resources. |
|
Pooling of funds and risks |
The ADRES pools the funds at the national level. It pays a lump sum (the UPC) per policyholder adjusted to the risk profile (age, gender, location) to the EPS, which must then manage the risk at the level of their portfolio of policyholders. |
|
Payment of service providers (contracts, reimbursements) |
EPS contract and make reimbursements to IPS using different methods. |
|
Healthcare services |
Care is provided by public or private IPS with which EPS have established agreements. Each EPS must contract its care network and may include IPS that it possesses up to a certain limit. The IPS apply out-of-pocket charges and co-payments, the amount or rate of which is regulated by the Ministry of Health and Social Protection. They also charge for services excluded from the compulsory healthcare package. |
|
Dispute settlement |
The Ministry of Health and Social Protection is responsible for receiving complaints, claims and suggestions from users. Healthcare users have a right to complain to the National Health Authority when an insurer or healthcare provider fails to meet its obligations or refuses to provide care. |
|
Quality assurance |
Quality control of services is the responsibility of the Ministry of Health and Social Protection, through its quality unit, which manages the compulsory health quality assurance system (SOGCS). The Ministry of Health has also set up a health quality observatory, which collects and disseminates information on the quality of care. |
4.4 Impact and lessons learned
Colombia currently has five health mutuals (ESS), two of which manage both schemes and the other three only the subsidized scheme. At the end of 2022, these mutuals had a total of 10.2 million insured persons, or 19.9 per cent of all insured persons in the country. Ninety-one per cent of persons insured by the mutuals were covered by the subsidized scheme, and 36.4 per cent of those covered by the subsidized scheme were insured by a mutual (figure 1).
Entities promoting the health of indigenous communities (EPSI) have 1.6 million members, representing just 3.1 per cent of all insured persons. Almost all their beneficiaries (96 per cent) are covered by the subsidized scheme.
Figure
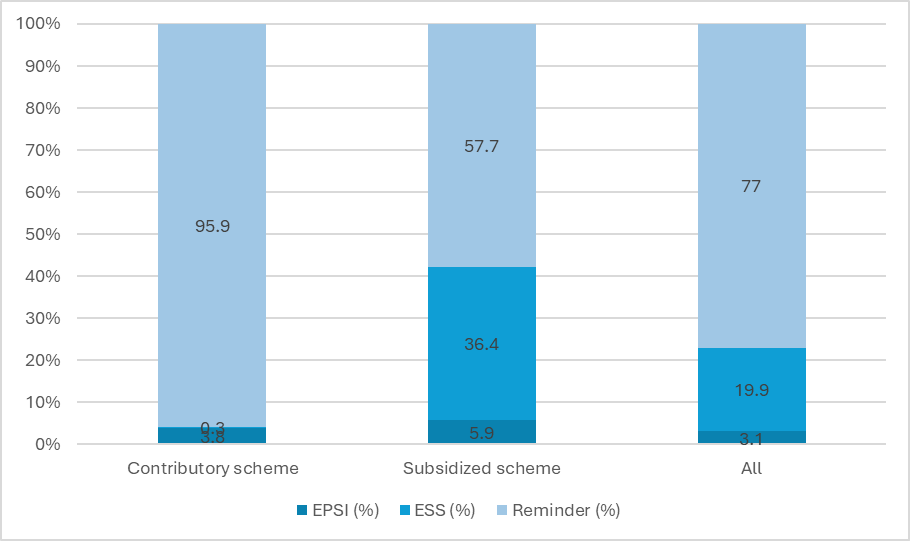
Note: EPSI: Entities promoting the health of indigenous communities. ESS: Mutuals
Source: Author's calculations based on data from
ESS have always been based on community organizations, with varying degrees of involvement. By their very nature, they promote user participation and encourage ongoing dialogue, which in turn benefits the work of the organizations. However, successive changes to the regulatory framework and new requirements regarding the minimum number of insured persons have weakened the participation processes
Indigenous EPS, which are deeply rooted in their communities, have played a role in investing in services tailored to their communities. For example, midwives and community health workers have been introduced
References
Colombia, Ministry of Health and Social Protection. 2014. Aseguramiento al Sistema General de Seguridad Social en Salud. https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VP/DOA/RL/cartillas-de-aseguramiento-al-sistema-general-de-seguridad-social-en-salud.pdf.
— 2021. Guía del usuario. Paso a paso sobre el acceso a los servicios de salud. https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/SG/SAB/AT/guia-usuario-minsalud.pdf.
— 2022a. "Cifras de afiliación en salud con corte a noviembre 2023". Tableau Software. https://public.tableau.com/views/CifrasAseguramientoenSalud_16166927767750/Aseguramiento?:embed=y&:showVizHome=no&:host_url=https%3A%2F%2Fpublic.tableau.com%2F&:embed_code_version=3&:tabs=no&:toolbar=yes&:animate_transition=yes&:display_static_image=no&:display_spinner=no&:display_overlay=yes&:display_count=yes&:language=es&:loadOrderID=0.
— 2022b. "Afiliación colectiva". Social Protection Unit. https://www.minsalud.gov.co/proteccionsocial/Paginas/Afiliaci%C3%B3nColectiva.aspx.
Decree No. 2313. 2006.
https://www.minsalud.gov.co/Normatividad_Nuevo/DECRETO%202313%20DE%202006.pdf
Espinal-Piedrahita, J. J. and Restrepo-Zea, J. H. 2022. "Financiamiento del sistema de salud colombiano: Tendencias y desafíos". Revista de Salud Pública, 24(1): 1–8. https://www.researchgate.net/publication/361261766_Financiamiento_del_sistema_de_salud_colombiano_tendencias_y_desafios.
GESTARSALUD (Asociación de Empresas Gestoras del Aseguramiento de la Salud). 2006. “Evolución de la participación social en las Empresas Solidarias de Salud”. https://www.social-protection.org/gimi/gess/RessourcePDF.action;jsessionid=V_QiCqpzMBQxy384rpX7ITC-3BSrcsmpUIunbphfqiCrmTFRNMz0!-2033066120?id=9512.
Law No. 100. 1993. https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/ley-100-de-1993.pdf.
Law No. 691. 2001. https://www.refworld.org/es/leg/legis/acnur/2001/es/130433
Mendieta, D. and Jaramillo C. E. 2019. "El sistema general de seguridad social en salud de Colombia. Universal, pero ineficiente: a propósito de los veinticinco años de su creación". Revista latinoamericana de derecho social, 29.
Mignone, J. and Gómez Vargas J. H. 2014. "Anas Wayuu, el éxito de una organización indígena de salud colombiana en medio de un sistema en crisis", Voces en el Fenix. No. 41. 01/12/2024. https://vocesenelfenix.economicas.uba.ar/anas-wayuu-el-exito-de-una-organizacion-indigena-de-salud-colombiana-en-medio-de-un-sistema-en-crisis/.
5. Côte d’Ivoire
5.1 Background
Health is a priority of the Côte d'Ivoire government's social policy, championed by President Alassane Ouattara when he was elected in 2011 and then reinforced as a flagship programme of his second term in office in 2015. The main aims were the construction and renovation of public health infrastructure and the creation of a universal medical coverage (CMU) scheme. The latter draws on the lessons learned from the failure to implement the universal health insurance (AMU) launched in 2001 and aims to enable everyone to take out immediate basic health insurance, covering the most important treatments and services and maternity costs.
The CMU scheme is based on Article 9 of the 2016 Constitution, which states that "Everyone has the right to access to health services". Its implementation is one of the social protection priorities in pillar II "Accelerating the development of human capital and promoting social well-being" of the 2016–2020 National Development Plan. Pillar IV "Strengthening inclusion, national solidarity and social action" of the 2021–2025 National Development Plan focuses on speeding up the process of enrolling people in the CMU scheme and covering the poorest people. The measures to achieve these objectives are set out in the Stratégie nationale de protection sociale (National Social Protection Strategy, SNPS) adopted in March 2014 and then in the 2018–2020 National Social Protection Strategy.
The process to implement the CMU scheme began in 2011 with the establishment of a permanent technical secretariat for the scheme and the development of an initial strategy for implementing a universal health insurance system. This document, which was officially approved in January 2012, gives an overview of the programme, with a focus on issues around the institutional architecture. The CMU scheme was established through Law No. 2014-131 of 24 March 2014. 50 Article 2 of this law stipulates that "This law establishes a compulsory system of health risk coverage for the benefit of populations residing in Côte d'Ivoire, known as universal health coverage". In April 2017, a pilot phase was launched to provide cover for students and finished at the end of December 2018; since 1 January 2019, students pay contributions to continue to benefit from CMU healthcare services. Following this pilot phase, the CMU scheme entered its operational phase, with contribution deductions beginning on 1 July 2019 and benefits on 1 October 2019 (Mian, 2022). With the launch of the CMU's operational phase and the first few months of implementation marked by a number of difficulties, a coordination and monitoring committee for implementing the CMU scheme 51 was set up in 2020, reporting to the Prime Minister, and a series of measures were taken to streamline the enrolment process and improve communication with other coverage systems.
5.2 The national social health protection system
Architecture and governance
The CMU scheme groups together two schemes covering the same healthcare package:
-
A contributory scheme, known as the Régime général de base (General Basic Scheme, RGB), financed by contributions from insured persons and covering the majority of the population living in Côte d'Ivoire.
-
A non-contributory scheme, known as the Régime d’assistance médicale (Medical Assistance Scheme, RAM), which is aimed at the poorest people and the State pays the insured persons’ contributions (STP/CMU, 2015).
The State has entrusted management of these schemes to an institution de prévoyance sociale (social welfare institution, IPS) known as the Caisse nationale d’assurance-maladie (National Health Insurance Fund, CNAM), created by decree in 2014 52 and placed under the dual supervision of the Ministry of Employment and Social Protection and the Ministry of the Economy and Finance. The CNAM's remit is to ensure:
-
management of schemes set up under the law establishing universal health coverage;
-
management of all special programmes, including on behalf of third parties, the purpose of which is to improve the management of health risks;
-
collection of contributions and provision of benefits under the various schemes;
-
management of the funds collected under the universal health coverage schemes;
-
regulation of universal health coverage.
The CNAM was initially designed as a simple governance and regulatory structure for the CMU scheme, based on existing coverage mechanisms and involving all stakeholders with experience in identifying populations, collecting contributions and managing healthcare benefits. Article 36 of Law No. 2014-131 gives the CNAM the option of transferring some of its powers, using a delegation agreement approved by the supervisory authority, to these stakeholders, who become DMOs; they may also develop complementary insurance schemes.
These stakeholders are public or private legal entities with the status of a social welfare institution, insurance company, social mutual or commercial health management company and with proven expertise in the technical management of health risks. Two types of DMO are identified in the CMU architecture:
-
DMOs performing functions relating to the identification of individuals and contributions. These DMOs are responsible for identifying insured persons and employers, collecting contributions and paying the contributions collected to the CNAM. This group includes the Caisse nationale de prévoyance sociale (National Social Welfare Fund, CNPS) and the Caisse générale de retraite des agents de l'Etat (General Retirement Fund for Civil servants, CGRAE), as well as the Solde civile (civilian payroll office) and the Solde militaire (military payroll office).
-
DMOs performing functions relating to benefit management. This group potentially includes the Mutuelle générale des fonctionnaires et agents de l'État de Côte d’Ivoire (General Mutual Fund of Civil Servants and State Agents of Côte d’Ivoire MUGEF-CI), insurers and social mutuals. These DMOs are responsible for carrying out medical checks and settling invoices, scheduling and managing online payments to healthcare providers.
Alongside the CMU scheme, the government has been running targeted free healthcare programmes since 2012, 53 aimed at:
-
pregnant women: free antenatal appointments, complementary checks, provision for normal childbirth and complications in childbirth, and caesarean sections;
-
children from birth to four years of age: Free medical and surgical treatment for the most common illnesses;
-
the general public:
-
the first 48 hours of medical and surgical emergencies;
-
treatment of malaria once a diagnosis is confirmed; and
-
in addition, a 30 per cent discount on the cost of all treatments over 1,000 CFA francs; in other words, that adult patients will have to pay 70 per cent of the cost of services.
These exemption measures are covered by the general budget, through the funding of medicine supplies and reimbursement to the health facilities concerned of the amounts owing for the targeted free services. At the end of each month, the health facilities record the charges billed and not collected for the targeted free services and send their statements to the Ministry of Health's financial affairs department for payment after checking usage.
Population coverage
Universal health coverage is designed as a compulsory health insurance scheme in which all Côte d'Ivoire residents are required to register. In practice, however, this requirement provided for in the 2014 law could not be implemented immediately for the entire population, and the country has opted for a gradual approach with a coverage target of 45 per cent of the population by 2025.
In 2013, the population covered by health insurance in Côte d'Ivoire was estimated at around 1.2 million people. Coverage was provided by the MUGEF-CI, social mutuals, commercial insurers (COLINA, ALLIANZ, AXA, NSIA, LMAI, and so on) and technical managers (MCI, ASCOMA and GRASSAVOYE). However, this figure was probably overestimated, as some insurers, and even some mutuals, entrust the management of health risks to a technical manager, each of whom reports the same number of insured persons (MEASFP, 2013).
CMU coverage targets
|
2014 |
2015 |
2016 |
2017 |
2018 |
2019 |
2020 |
|
|
Total population (million) |
24.44 |
25.06 |
25.69 |
26.33 |
26.97 |
27.61 |
28.25 |
|
Number of people in the poorest category included in the above figure (million) |
1.83 |
1.88 |
1.93 |
1.97 |
2.02 |
2.07 |
2.12 |
|
Insured population (million) |
4.07 |
5.36 |
7.36 |
8.50 |
9.66 |
10.34 |
11.03 |
|
Number of the poorest insured persons included in the above figure (million) |
- |
0.25 |
1.00 |
1.50 |
3.02 |
2.07 |
2.12 |
|
Insured population (%) |
16.67 |
21.39 |
28.66 |
32.29 |
35.82 |
37.46 |
39.03 |
|
Of which insured indigents (%) |
0 |
13 |
52 |
76 |
100 |
100 |
100 |
Source: MEASFP, 2013
Based on the figures announced by the CNAM and the government, actual coverage has increased much less rapidly than expected. It should also be noted that these figures indicate the number of people enrolled and the number of policyholder cards distributed, but not the number of people who are up to date with their contributions and actually insured. The policyholder card is in fact issued for life, but entitlement to benefits is conditional on regular payment of contributions; connected biometric card readers can be used to check the identity and entitlement to benefits (up-to-date contribution account) of each insured person when they use the health services.
CMU enrolment situation
|
2019 |
2021 |
|
|
Number of people enrolled (million) |
3.19 |
3.24 |
|
Number of policyholder cards distributed (million) |
2.11 |
2.07 |
|
Number of people in the poorest category included in the above figure (million) |
0.20 |
0.21 |
Sources: 2019 – CNAM; 2021 – (https://www.gouv.ci/, 2022)
The gap between forecasts and the number of policyholder cards distributed to the poorest people is particularly wide. However, a process of targeting the poorest households has been under way since 2017 and is due to be extended to the whole country by 2025. This operation should lead to 2.5 million people being enrolled in the RAM (Ouedraogo, 2022)
Risks covered/healthcare package
The CMU healthcare package is defined by Decree No. 2017-149 54 and is the same for the RGB and the RAM. Treatments covered have been the subject of negotiations between the CNAM and the Ministry of Health in order to offer preferential rates to CMU policyholders, which are set by interministerial decree. 55
With this package, the CMU covers a wide range of medical services, including hospitalization and medicine supply. Childbirth and caesarean sections are also covered under the current free-of-charge policy.
Guaranteed services are only covered by the CMU scheme at the level of public, religious or private service providers, at all levels of the health pyramid, who have signed or acceded to an agreement with the CNAM. All medicines are generic and are available at the same price in both public hospital pharmacies and private pharmacies throughout the country.
Expenses for healthcare package services, including medicines, are covered at a single rate of 70 per cent, subject to compliance with a referral scheme and care pathway. 56 The remaining 30 per cent of costs are borne by the insured person in the form of a co-payment, which may be covered by complementary insurance offered by private insurers and mutuals.
Bringing the CMU into operation is accompanied by key measures to redevelop and equip first-contact health facilities forming part of the healthcare network, as well as to recruit CMU-specific reception staff in hospitals, improve medicine distribution and raise awareness and inform the population about operating procedures and the quality and accessibility of CMU medications.
The government has invested 833 billion CFA francs in the construction of health infrastructure and in the recruitment of suitable human resources during the period 2018–2020. This investment will continue over the period 2020–2024, to the tune of more than 1,650 billion CFA francs, as part of a vast programme to build, redevelop and modernize university hospitals, regional and general hospitals, and health centres (Mieu, 2020).
Financing of the CMU scheme
The RGB is financed by a single lump-sum contribution of 1,000 CFA francs per month per person over the age of five (children aged from birth to five years of age are covered by a free programme financed by the State). Children between the ages of five and 21 are paid for by their parents, as are adults with disabilities. Employers pay 50 per cent (500 CFA francs/month per person) of employee contributions in the private sector and similar sectors or civil servants, their spouses and up to six children up to the age of 21; beyond six children, the employee must pay all contributions. Several collection mechanisms are in place:
-
Contributions for civil servants and retired civil servants are deducted by the CGRAE, the civilian payroll office (Solde Civile) and the military payroll office (Solde Militaire).
-
Contributions from employees in the formal private sector are collected via the online portal and the e-CNPS application by the CNPS.
-
Contributions from self-employed workers are collected by the CNAM through payment mechanisms set up via the CNAM's online site, mobile phone operators, commercial banks and microfinance organizations.
-
Contributions from small traders and craft workers liable for the lump-sum payment provided for in the General Tax Code are collected when the tax is paid.
-
Contributions payable by students aged 21 and over are collected by higher education institutions and recovered in one or more instalments.
-
The collection of contributions payable by persons engaged in agriculture is adapted to the seasonal nature of agricultural producer income in accordance with the procedures set out in interministerial orders. Thus for:
-
the cotton sector, collection is made annually by cotton companies based on cotton seed purchases made in their exclusive area of activity; and
-
the oil palm and sugar cane sectors, contributions are deducted based on production sales of oil palm mills and village sugar cane cooperatives (MEPS, 2021).
The RAM is a non-contributory scheme in which the State undertakes to pay the contributions of eligible persons. The CNAM estimated the RAM budget for 2022 at 12 billion CFA francs (Gouvernement
5.3 A system based on delegated management but minority mutuals
Mutuals
In 2012, the government established the Agence Ivoirienne de régulation de la mutualité sociale (Ivorian Regulatory Agency for Social Mutual Insurance, AIRMS), 57 which is the administrative body for social mutual insurance in Côte d'Ivoire, with the following main tasks:
-
examining applications for approval of social mutuals
-
maintaining the national register of social mutuals
-
monitoring and oversight of approved social mutual
In 2018, AIRMS listed 61 social mutuals:
|
Registered |
Not registered |
Total |
|
|
Corporate mutuals |
12 |
10 |
22 |
|
Private-sector mutuals |
10 |
17 |
27 |
|
Public-sector mutuals |
7 |
3 |
10 |
|
Umbrella organizations |
1 |
1 |
2 |
|
Total |
30 |
31 |
61 |
Source: AIRMS, 2018 (Abinan, 2019)
In May 2021, the AIRMS register included 45 social mutuals, duly constituted in accordance with Directive No. 07/2009/CM/UEMOA on regulating social mutual schemes within the UEMOA and registered. These mutuals cover an estimated 1.5 million beneficiaries, or 6.25 per cent of the Ivorian population (Kamgate, 2020). However, the bulk of this population is covered by the MUGEF-CI, which in 2018 had 263,942 contributing members and 739,506 beneficiaries.
Apart from the MUGEF-CI, social mutuals mainly cover workers in the formal private sector. These mutuals are commonly known as "employer-sponsored mutual insurance" and provide health insurance for company employees and their families. On the other hand, mutual health insurance is underdeveloped in the informal and agricultural sectors.
All these mutuals offer a wide range of healthcare packages, providing partial or total cover for health expenses.
Institutional framework
As emphasized above, the CMU scheme was designed with the support of actors already present and experienced in the field of health insurance. Among these, social mutuals were identified as potentially key actors in CMU, particularly because of their presence and involvement in the formal and informal economies. They were therefore integrated into the CMU scheme, with an expected involvement in raising awareness among the population and an intervention as DMOs in terms of contributions and benefits.
The status of DMO in CMU puts social mutuals on an equal footing with insurance companies and commercial health management companies. For the former, this means putting themselves on the same footing as the latter and strengthening their technical management capacities, in order to perform effectively and guarantee a lasting contractual relationship as a DMO with the CNAM. Similarly, this status requires mutuals to comply with Directive No. 07/2009/CM/UEMOA on social mutuals, which was notably the case for MUGEF-CI, which had to restructure as a result.
This compliance is part of a set of specifications to be met by DMOs, drawn up when the CMU scheme was designed. These include:
-
compliance by the DMO with the management standards of its category (including the Code of the Inter-African Conference on Insurance Markets, WAEMU community directives on social mutual schemes, Organization for the Harmonization of Business Law in Africa, and so on);
-
maintenance of a minimum number of beneficiaries to avoid the proliferation of small DMOs, which would result in an excessive workload, linked to the proliferation of DMO agreements to handle membership that the CNAM would have to manage; and
-
technical upgrades and integration into IT platforms and information and monitoring systems (MEASFP, 2013).
Faced with these constraints, social mutuals in the informal and agricultural sectors have been greatly hampered by a series of challenges, including their small-scale intervention, a limited number of beneficiaries and weak technical management (MEPS, 2021). DMOs are not used in services whose functions have been entrusted solely to MUGEF-CI and health portfolio managers (ASCOMA and MCI-Care Côte d'Ivoire).
Delegated functions
The CNAM was designed as simple structure reliant on DMOs. The CNAM's remit is to ensure:
-
the roll-out, promotion and communication to institutions of the CMU scheme;
-
the management of schemes set up under the law on establishing universal health coverage;
-
agreements with healthcare providers;
-
the management of all special programmes designed to improve health risk management; 58
-
the pooling and management of funds collected under the schemes;
-
the management of resources and associated benefits under the various schemes; and
-
the steering and regulation of CMU (Koné, 2021).
There are two distinct categories of DMO in the CMU scheme:
-
DMOs dealing with contributions, which deduct contributions at source from employees and retirees in the public and private sectors. Three major stakeholders are involved here, the CNPS, the CGRAE and the civilian and military payroll offices (Solde civile and Solde militaire), with a remit to:
-
collect contributions from the insured persons in their charge; and
-
pay the contributions collected to the CNAM.
It should be noted that in April 2022 the CNAM signed a partnership agreement with the Mutuelle des familles des diasporas ivoiriennes (Mutual for Ivorian diaspora families, MFDI) to collect contributions from the families of the Ivorian diaspora. The MFDI is the only social mutual that has signed a DMO contribution management agreement with the CNAM (FAAPA, 2022).
-
DMOs dealing with benefits (mutuals, private insurers, health portfolio managers) have a remit to:
-
check compliance of treatment forms sent by healthcare providers;
-
carry out medical checks and settle invoices/providers; and
-
schedule payments to healthcare providers.
A third stakeholder is involved in this scheme, in the specific context of biometric enrolment and identification of CMU populations. In 2014, the State signed a public-private partnership contract with the Société nationale d'édition de documents administratifs et d'identification (National Company for the Publication of Administrative and Identification Documents, SNEDAI). The SNEDAI set up a subsidiary, SNEDAI-CMU, which is responsible for biometric enrolment through open offices and mobile teams deployed in all districts, as well as supplying a unique identification card and introducing a business application to manage the scheme. This partnership is justified in part by the importance of the registration number assigned to each insured person, which has become the sole identifier for the social security system in Côte d'Ivoire, replacing all other systems for identifying insured persons.
Distribution of functions within the CMU scheme
|
Functions |
Distribution |
|||
|
CNAM |
DMO Contributions |
DMO Services |
SNEDAI |
|
|
Definition of the healthcare basket |
X |
|||
|
Agreements |
X |
|||
|
Education and promotion |
X |
|||
|
Enrolment, membership and renewal |
X |
X |
X |
|
|
Contribution collection |
X |
|||
|
Pooling of risks covered |
X |
|||
|
Payment of benefits |
X |
X |
||
|
Healthcare services |
||||
|
Medical checks |
X |
|||
|
Follow-up and steering |
X |
|||
5.4 Impact and lessons learned
With the exception of the specific case of the MUGEF-CI and, recently, the MFDI, social mutuals are not very visible within the CMU scheme, although they were initially identified as potentially the most important actors in the roll-out of CMU in the informal economy. They are local actors who can provide information and raise awareness among the population in order to promote adoption of the CMU project and support for the principle of health insurance. Their actual role in this area is poorly documented, and promotional campaigns are mainly run by the CNAM and national stakeholders such as workers' organizations, the Comité intersyndicale pour la transition vers l'économie formelle (Inter-union Committee for the Transition to the Formal Economy, CITEF) and external partners such as the ILO.
However, the lack of a community base is one of the weak points of the CMU scheme. The CMU scheme's national roll-out currently relies solely on the decentralized structures of the CNPS and the CGRAE, which only have branches in major towns. It is therefore not integrated into community structures and has no connections with local communities and actors in the informal and agricultural sectors. This absence partly explains the slow expansion of the CMU. Faced with this situation, the report on the 2018–2020 SPNS in 2021 identified the following measures to be implemented as part of the 2021–2025 PNPS:
-
The development of innovative and incentive measures to boost the enrolment of as many workers as possible in the informal and rural economy and to make their contributions ongoing, so as to ensure the scheme’s sustainability.
-
Mobilizing social mutuals to identify and enrol people and collect CMU contributions, particularly from workers in the informal economy.
References
Abinan, P. K. 2019. Statement by Mr. Pascal Kouakou Abinan, Minister of Employment and Social Protection, AIM International Conference on Mutual Benefit Societies, entitled "Le pari de la mutualité pour le XXIe siècle". PowerPoint presentation. Lomé, 22 January 2019.
FAAPA (Fédération atlantique des agences de presse africaines). 2022. "La CNAM signe un partenariat avec la mutuelle des familles des diasporas ivoiriennes". FAAPA, 15 April 2022. http://www.faapa.info/blog/la-cnam-signe-un-partenariat-avec-la-mutuelle-des-familles-des-diasporas-ivoiriennes/.
Gouvernement de Côte d'Ivoire. 2022. "Couverture maladie universelle (CMU) : 3 244 503 personnes enrôlées en Côte d’Ivoire à fin décembre 2021". Official portal of the Government of Côte d'Ivoire, February 2022. https://www.gouv.ci/_actualite-article.php?d=4&recordID=13125&p=118.
— 2022b. "Couverture maladie universelle : 2,5 millions de personnes vont bénéficier du régime d'assistance médicale". Official portal of the Government of Côte d'Ivoire. https://www.gouv.ci/_actualite-article.php?recordID=13112.
Kamgate, I. 2020. "Côte d'Ivoire : Avec des réserves de 24,854 milliards Fcfa, l'AIRMS veut transférer ses valeurs mobilières à la CDC-CI". Financial Afrik (blog), 31 May 2020. https://www.financialafrik.com/2020/05/31/cote-divoire-avec-des-reserves-de-24854-milliards-fcfa-lairms-veut-transferer-ses-valeurs-mobilieres-a-la-cdc-ci/.
Koné, O. 2021. "La couverture maladie universelle". PowerPoint presentation. CNAMU, 2021.
Mian, J.P. 2002. "Analyse des cadres institutionnels et opérationnels des programmes et mécanismes existants (CMU et RSTI) de protection sociale pour une meilleure couverture des travailleurs et entrepreneurs de l'économie informelle". Ministry of Employment and Social Protection, European Union and ILO, March 2022. https://socialprotection-pfm.org/wp-content/uploads/2022/03/RAPPORT-FINAL-Analyse-Cadre-IO-PS.pdf.
Mieu, B. 2020. "Côte d'Ivoire: la couverture maladie universelle, un immense défi pour le gouvernement – Jeune Afrique". JeuneAfrique.com. https://www.jeuneafrique.com/mag/902959/societe/cote-divoire-la-couverture-maladie-universelle-un-immense-defi-pour-le-gouvernement/.
MEASFP (Ministry of State and Ministry of Employment, Social Affairs and Vocational Training). 2013. "Note de présentation de la Couverture Maladie Universelle (CMU)". October 2013.
MEPS (Ministry of Employment and Social Protection). 2021. "Rapport bilan, Mise en œuvre de la stratégie nationale de protection sociale 2018–2020", February 2021. https://emploi.gouv.ci/wp-content/uploads/2021/09/RAPPORT-BILAN-SNPS-2018-2020-DGPS.pdf.
Ouedraogo, P. 2022. "Côte d'Ivoire: 2.5 million people to benefit from RAM2. P4H Network, 7 February 2022. https://p4h.world/en/news/cote-divoire-2-5-million-people-to-benefit-from-ram/.
STP/CMU (Secrétariat technique permanent de la CMU). 2015. Architecture de la couverture maladie universelle en Côte d'Ivoire, PowerPoint presentation, STP/CMU, 19 January 2015.
6. Ethiopia
6.1 Background
The 1994 Ethiopian Constitution states that "the State has the obligation to allocate ever increasing resources to provide to the public health, education and other social services" (Article 41.4) and that "to the extent the country's resources permit, policies shall aim to provide all Ethiopians access to public health and education, clean water, housing, food and social security" (Article 90.1) (Schwettmann, 2022). In this context, Ethiopia launched a Health Extension Programme (HEP) in 2003, initially in the country's four main agricultural regions, then adapted and scaled up for the country's pastoral and urban communities. The aim of this programme was to achieve primary healthcare universal coverage, in order to combat poor access to health services for the population, particularly in the poorest rural areas, healthcare staff shortages, and the lack of institutional synergies.
The HEP was accompanied by a CBHI pilot project in 13 woredas (districts) in these four regions in 2011. This pilot project was preceded by a health insurance proclamation, 59 approved in 2010, which introduced two types of system:
-
community-based health insurance (CBHI) for the informal and agricultural sectors
-
social health insurance (AMS) for employees in the formal sector
This proclamation also established the Ethiopian Health Insurance Agency (EHIA) to manage these two insurance systems.
Social health insurance for employees in the formal sector is still not up and running. On the other hand, CBHI has grown significantly since it was launched on an experimental basis in July 2011. This development has been supported since 2015 by the Health Sector Transformation Plan (HSTP) 2015/16–2019/20 launched by the Federal Ministry of Health as part of the country's Growth and Transformation Plan. The HSTP is the first phase of a 20-year strategy "Envisioning Ethiopia's Path towards Universal Health Care through Strengthening Primary Health Care (2015–2035)". This programme aims to increase the use of health services by creating links between communities and healthcare provision, introducing free programmes and increasing the proportion of people covered by CBHI, in order to achieve the objectives of UHC (UHC, 2022).
CBHI was inspired by the experiences of other countries, notably Rwanda and Ghana in the 2000s and in 2010. Based on the encouraging results of the pilot project launched in 2011 in the first 13 woredas, the scheme was extended from 2013 to cover 350 woredas in 2017 and then 827 rural and urban woredas in 2020 (out of the 1,100 existing Ethiopian districts), with coverage of 14.5 million and 32 million people respectively (Mulat et al., 2022). According to the EHIA, CBHI coverage has been extended to 78 per cent of the country's districts, covering 43 million people in 2021.
6.2 The national social health protection system
Architecture and governance
The United States Agency for International Development (USAID), which was the main CBHI partner in Ethiopia, defines CBHI as "any scheme managed and operated by an organization, other than a government or private for-profit company, that provides risk pooling to cover all or part of the costs of health care services" (Zelelew, 2015). However, actual implementation of CBHI in Ethiopia is primarily managed by the government, with community involvement in its design, management and oversight. In fact, an important feature of this programme is that guidance is given at the national level but within an architecture that ensures coordinated decision-making with community members as well as risk pooling and management at the district level.
The system is organized on three main levels:
-
CBHI has a branch in each kebele 60 whose residents collectively decide whether to join the insurance scheme. Following an awareness-raising campaign, a kebele joins the scheme if a majority (based on a simple majority vote) of its residents support the idea and show an interest. When the decision is taken collectively to participate in the programme, each household has the individual choice of whether or not to join the health insurance scheme (Feleke et al., 2015).
-
The association of kebele branches forms the CBHI scheme at woreda (district) level. 61 The woreda CBHI is the heart of the community-based health insurance system. It is responsible for registering beneficiaries, collecting, pooling and managing CBHI funds, concluding agreements with healthcare providers and processing reimbursements for health services. The woreda CBHI is governed by a general assembly composed of three to five representatives, appointed by member households, from each kebele participating in the system and representatives of the woreda administration. It has a governing body that manages the day-to-day running of the scheme. The government funds three employees (a coordinator, an accountant and an information specialist). It should be noted that local government staff at kebele level are also used for mobilizing resources and organizing meetings (Feleke et al., 2015). Benefits, registration fees, contributions and collection methods are set out at the national level but woreda CBHI are able to amend and adapt these to their specific circumstances.
-
The 2010 proclamation created the EHIA to jointly manage the CBHI and AMS programmes. The EHIA was created as an autonomous body of the federal government through Regulation No. 191/2010 62 with a remit to implement and directly manage social health insurance for workers in the formal economy and their dependants, and to support the roll-out and management of CBHI, together with various development partners. The Agency has regional branches to implement the health insurance system countrywide.
Population coverage
Membership of CBHI is by household to reduce the risk of adverse selection. Once the inhabitants of a kebele have chosen to participate in the programme, each household's membership is voluntary. There are two categories of household:
-
Households with the ability to pay: registration with CBHI comes into effect when a household decides to pay its membership contribution, which must be renewed each year;
-
Poor households: the government subsidizes the contributions of 10 per cent of the individuals in each kebele, identified by local officials and the community as being the poorest. These individuals are then registered by CBHI officials at the woreda level to benefit from this subsidy programme.
Of the country's 115 million inhabitants in 2020, CBHI covered 31.9 million people of the country's 115 million inhabitants in 2020, or 28 per cent of the population, spread across 6.9 million households in Ethiopia's informal sector (Schwettmann, 2022). This rate of population coverage varies significantly from one region and district to another, depending in particular on the socio-economic situation and the commitment of the local administration to promoting insurance (Merga et al., 2022).
Among these scheme members, poor and vulnerable households covered by the State's subsidy for the poorest people account for a fifth (21 per cent) of member households, far more than the CBHI guidelines, which limit this coverage to only 10 per cent of beneficiaries (SP&PFM, 2020).
The population coverage rate is still well below the target of 80 per cent of the population covered by 2020, set by the HSTP adopted in 2015 (Mulat et al., 2022), which is nevertheless high for a voluntary scheme in Africa. The fact that the design of CBHI was inspired by a traditional Ethiopian practice of mutual aid and solidarity, known as idir, is often put forward as one of the factors explaining high membership (Participedia, 2020). In addition, membership is by household, to avoid the risk of adverse selection. It should be noted, however, that all the studies refer to households and individuals enrolled, but do not specify whether these are actual policyholders making regular contributions. The membership renewal rate was only 54 per cent in 2015, but rose sharply to 80 per cent in 2020 (Schwettmann, 2022).
Healthcare package
CBHI offers a broad and comprehensive coverage of benefits set out under the pilot project. This coverage includes outpatient services, gynaecological and obstetric services and hospital and surgical services, as well as diagnostic tests and generic drugs in health centres and public hospitals. Private health facilities are not covered by the insurance, unless a particular service or medication is not available in a public facility.
Coverage excludes spectacles, cosmetic treatments such as artificial teeth and plastic surgery, and organ transplants, chronic kidney dialysis, treatment with non-generic medicines or treatment abroad.
Expenses are 100 per cent covered when beneficiaries adhere to the referral scheme, first using health centres before, if necessary, being referred to district or regional hospitals. In this regard, each woreda CBHI is paired with a health centre, which is the gateway to the referral scheme. Beneficiaries who do not follow this route are only covered for 50 per cent of costs (Yilma et al., 2015).
Financing
CBHI is funded by household contributions and general subsidies from central government and targeted subsidies from the regions and districts:
-
Contributions are paid once a year, during two–three month period in rural areas, chosen by the woreda according to the harvest season. They are collected by kebele representatives, following procedures set out at the national level but which can be adapted by the woreda CBHI. Once collected, these contributions are paid directly to the woreda insurance headquarters. The contribution is a lump sum per household per year; adult children can be covered by a household for an additional contribution. During the pilot phase, which began in 2011, contributions ranged from US$7.31 to US$10.45 per household per year, depending on the CBHI's rural or urban area of operation. Some woreda CBHI have gradually taken the liberty of adapting the amount of contributions to suit local conditions, and even of varying the contributions according to household size (Hussein et al., 2022). In 2020, the average annual contribution per household was US$6.9 (Schwettmann, 2022). General subsidies from central government finance 25 per cent of household contributions to reduce the burden on households and make insurance more accessible.
-
The targeted subsidies for regions and districts are intended to cover the full cost of contributions for the 10 per cent of the population identified as being the poorest and most vulnerable; this quota is lower than the average poverty rate of 23.8 per cent.
-
In addition, the regional and district governments fund three employees per woreda CBHI as well as some operational costs. When a new woreda CBHI is set up, the central government provides resources to the health facilities under contract with it in order to improve the quality of the health services that will be offered to beneficiaries (EHIA, 2015).
Household contributions and government subsidies are the main source of funding for CBHI. During the period of the first Health Sector Transformation Plan (2015–2019), the CBHI schemes mobilized around US$146.7 million, including US$102.9 million in household contributions, US$28.9 million in targeted subsidies and US$14.6 million in general subsidies (ILO, 2021).
The following table summarizes changes in CBHI overall resources from household contributions since the pilot years. These resources have risen sharply as CBHI schemes were extended across the country and membership increased.
Total amount of contributions collected by CBHI
|
Years |
ETB (millions) |
US$ (millions) |
|
2010/11 |
42 |
2.9 |
|
2014/15 |
148.4 |
7.35 |
|
2019/20 |
1 640 |
51.1 |
|
2020/21 |
2 020 |
101 |
Source: ILO, 2022
6.3 A system based on partnership between the State, the woreda and the kebele
Legal framework
The 2010 Federal Proclamation on Social Health Insurance provides the legal framework for CBHI and sets out its main policy directions, including the creation of the EHIA as the regulatory body and oversight mechanism for CBHI, and the responsibility given to woreda CBHI to cover the health expenses of households in the informal economy. The proclamation also sets out the appropriate proportion of poorest people and the mechanisms for the centralized pooling of contributions and national and regional subsidies (SP&PFM, 2020).
The general assemblies of each woreda CBHI adopt their statutes and approve the insurance regulations, which set out in particular membership fee and annual contribution amounts, as well as the collection schedule. These statutes and regulations constitute the legal framework of each CBHI, approved by the EHIA.
The architecture put in place responds to the State's desire to empower local communities by involving them in the configuration, governance and management of the insurance, while strengthening the transparency of the system:
-
The EHIA and the Federal Ministry of Health act as supervisory and implementing units for the project. They have regional coordination units to oversee the operations of the woreda CBHI. This national coordination has developed a set of financial and administrative management tools that are used by the woreda CBHI, as well as information and training materials for the various stakeholders, such as health workers and local government staff.
-
Kebele committees and woreda general assemblies and governing bodies are "participatory decision-making and management structures" responsible for setting up and managing health insurance. The communities also participate in community monitoring of the effectiveness and quality of the health services covered, through member and non-member surveys.
The CBHI system is also supported by a number of external partners, including USAID, CARE Ethiopia and Abt Associates, 63 which play a major support role in terms of designing, steering and extending the system.
Distribution of functions within community-based health insurance
The governance of woreda CBHI is comparable to that of mutuals, although they are not entirely autonomous entities. They are community-based structures integrated into a national health insurance scheme, implemented and coordinated by the EHIA, within which there is no delegation of management but rather a distribution of functions between the different levels of the scheme.
At the central and regional level:
The EHIA is the federal body responsible for implementing, expanding, coordinating and monitoring the CBHI system.
The EHIA sets out the CBHI's operational procedures and designs and prints management media such as policyholder cards, voucher books and other documents for distribution to the woreda CBHI.
Similarly, the agency has developed a model agreement with health facilities that woreda CBHI adapt when entering into agreements with healthcare providers in their coverage area.
At the local level:
-
The kebele are responsible for raising awareness, mobilizing communities and registering members.
-
Contributions are also collected by the kebele, whose committee members collect them on a voluntary basis. All contributions are paid to the woreda CBHI, which has a bank account in a microfinance institution or a commercial bank, depending on the region.
-
The pooling of resources and risks is a function shared between the EHIA at regional and national level and the woreda CBHI. The latter retain 70 per cent of the contributions and pay 20 per cent to the regional EHIA representations, which cover care in the local and regional hospitals, and 10 per cent to the central EHIA, which covers the tertiary level of the health pyramid and is a reserve fund.
-
Each CBHI adapts a prototype agreement drawn up by the EHIA for its own use and enters into agreements with district health facilities. Local, regional and specialist hospitals have agreements with the EHIA.
-
The woreda CBHI are responsible for purchasing services from the district's primary and secondary health facilities.
Distribution of functions in the community-based health insurance system
|
Functions |
Distribution |
|||
|
EHIA |
Woreda CBHI |
Kebele committees |
||
|
Definition of the healthcare package |
X |
|||
|
Agreements |
X |
X |
||
|
Education and promotion |
X |
X |
X |
|
|
Enrolment, membership and renewal |
X |
X |
||
|
Contribution collection |
X |
|||
|
Pooling of risks covered |
X |
X |
||
|
Payment of benefits |
X |
X |
||
|
Healthcare services |
||||
|
Follow-up and steering |
X |
X |
||
6.4 Impact and lessons learned
Implementation of the CBHI has been underpinned by strong political commitment at the highest levels of the Ministry of Finance, the Ministry of Health and the EHIA. It has also benefited from the involvement and support of a range of stakeholders, including regional governments, development partners, the private sector, international and local NGOs and civil society organizations, as well as academic institutions (Mulat et al., 2022).
Among the system’s other strengths, CBHI design is based on lessons learned from other countries, notably Rwanda, Senegal and Ghana. It also draws on traditional practices, such as mutual aid funds (idir) that help community members in emergencies (funerals, and so on).
In addition, evaluations carried out following the pilot phase launched in 2011 and regularly thereafter helped to refine the design of the system for its extension phase. In particular, these evaluations have shown the impact of CBHI on the use of health services, which stands at 0.7 visits per insurance beneficiary per year compared with a national average of 0.3, and on the mobilization of resources for the health sector, with a funding pool combining household contributions and State subsidies (Mulat et al., 2022). The population coverage rate was 28 per cent in 2020, although with regional variations, compared with sub-Saharan African countries where the average is generally less than 10 per cent. Similarly, annual membership renewal rates are high and rising, from 54 per cent in 2015 to over 80 per cent in 2020, indicating a high level of satisfaction with the health insurance scheme (Schwettmann, 2022).
However, a number of challenges are also highlighted:
-
In terms of system governance and management:
-
An evaluation carried out in 2015 highlighted weaknesses in the kebele committees, mainly linked to the fact that activities are carried out on a voluntary basis by members who also have other work responsibilities and lack the motivation to carry out their CBHI-related duties. These committees also have no operating budget, particularly to cover travel expenses. The result is delays in raising awareness and renewing memberships, updating information on policyholder cards and depositing contributions at the district level. The consequences of these weaknesses in some districts have been to discourage membership renewal or to encourage households to renew their membership only when health services are needed immediately, leading to financial difficulties for the scheme (EHIA, 2015).
-
The woreda CBHI schemes are responsible for the implementation, extension and management of health insurance in the districts; they are the largest component of the national CBHI system. These entities generally come under the umbrella of the woreda administration, providing the scheme with free office space, utilities, transport and communication services, and stationery supplies. The woreda administration pays the salaries of the three civil servants assigned to the CBHI, who also have an operational budget, albeit too small. Each woreda CBHI is governed by a general assembly and a governing body. The 2015 evaluation found that these bodies meet infrequently or not at all in most districts, with delayed or no decision-making (EHIA, 2015).
-
The EHIA was established at national level to lead the overall development of the CBHI, with branches at the regional level. However, there is little coordination between the Agency and the woreda CBHI schemes, and this gap is worsening as the system extends across the country (EHIA, 2015).
-
In terms of funding, the operating costs of the woreda CBHI and the general and targeted subsidies represent an increasing burden for the State and the regions as the system extends. The ability to mobilize sufficient resources is a particularly important challenge in order to maintain the same level of human resources, administrative support and contribution subsidies, particularly for the poorest households.
-
Non-compliance with procedures by contracted healthcare providers sometimes prevents care from being provided, particularly when it comes to writing prescriptions and recording them in beneficiary reimbursement files. CBHI are also confronted with over-prescription of services and medicines, as well as erroneous referral of patients to private health services not covered by the agreement (ILO, 2022).
-
As noted above, the level of CBHI membership is high compared to other experiences in the region, but with varying penetration rates and membership renewal rates from region to region. Depending on the region, these variations are partly related to:
-
the level of commitment from local government;
-
the weaknesses observed in the kebele committees and the woreda CBHI;
-
the quality of health services, with shortages of human resources, medicines and medical equipment in some public facilities; and
-
difficulties for some households not eligible for targeted subsidies to pay enrolment fees and contributions (Mulat et al., 2022).
Ethiopia's experience is comparable with that of Senegal. Both countries were largely inspired by the CBHI scheme set up in Rwanda, before it was switched to a centralized system managed by the National Social Security Fund. As in the other two countries, CBHI in Ethiopia is a hybrid system that aims to promote strong community involvement, with the need for centralized steering and guidance. The challenges are also the same: at the operational level, with the gradual expansion of the system across the country, the EHIA will need to have significant resources at its disposal to support the insurance administration, which should eventually extend to 1,100 woreda. The Agency will need to be in a position to coordinate and standardize rules and procedures, and to develop the technical capacity to promote high-quality technical management at all levels of the insurance system. As far as funding is concerned, scaling up the system requires the State and the EHIA to mobilize an increasing level of resources needed to maintain the same level of subsidization of contributions and operations. In addition, fragmented organization at the woreda level and voluntary membership mean that the financial viability of CBHI in the most financially disadvantaged districts is fragile, and there is a need to increase risk pooling and build an equalization system at national level.
References
EHIA (Ethiopian Health Insurance Agency). 2015. "Evaluation of Community-Based Health Insurance Pilot Schemes in Ethiopia: Final Report". Addis Ababa, May 2015. https://www.hfgproject.org/evaluation-cbhi-pilots-ethiopia-final-report/.
Feleke S., Mitiku W., Zelelew H. and Ashagari T.D. 2015. "Ethiopia's Community-Based Health Insurance: A Step on the Road to Universal Health Coverage". Health finance & governance, USAID, January 2015. https://www.hfgproject.org/ethiopias-community-based-health-insurance-step-road-universal-health-coverage/.
Hussein M., Muluken A. and Bayou N.B. 2022. "Continued adherence to community-based health insurance scheme in two districts of northeast Ethiopia: application of accelerated failure time shared frailty models". In International Journal for Equity in Health 21(1), No. 16. https://doi.org/10.1186/s12939-022-01620-9.
ILO (International Labour Organization). 2021. ILO Prospect. "Mapping of the National Social Protection System in Ethiopia, Including Social Health Protection: Final Report. Geneva, ILO, 2021. https://www.ilo.org/global/programmes-and-projects/prospects/countries/ethiopia/WCMS_821183/lang--en/index.htm.
— Unpublished. "Feasibility Study on the Enrolment of Urban Refugees and Asylum Seekers in the Community Based Health Insurance Scheme in Ethiopia". ILO, 2022.
Merga B.T., Balis B., Bekele H. and Fekadu G. 2022. "Health insurance coverage in Ethiopia: financial protection in the Era of sustainable development goals (SDGs)". In Health Economics Review 12(1), No. 43. https://doi.org/10.1186/s13561-022-00389-5.
Mulat A.K. Mao W., Bharali I., Balkew R.B. and Yamey G. 2022. "Scaling up community-based health insurance in Ethiopia: a qualitative study of the benefits and challenges". In BMC Health Services Research 22, No. 473. https://doi.org/10.1186/s12913-022-07889-4.
Participedia. 2020. "Community Based Health Insurance in Ethiopia". Participedia, 2020. https://participedia.net/case/4958.
Schwettmann J. 2022. "Vers une couverture sanitaire universelle : Les cas du Bénin, de la Côte d'Ivoire, de l'Éthiopie, du Kenya, du Sénégal et de la Zambie". Friedrich Ebert Stiftung. January 2022. https://library.fes.de/pdf-files/iez/18889.pdf
SP&PFM (Social Protection & Public Finance Management). 2020. "Improving Synergies between Social Protection and Public Finance Management for Ethiopia: A Fact-Finding Report based on ILO Social Security Inquiry (SSI) Assessment for Ethiopia". PowerPoint, December 2020. https://socialprotection-pfm.org/wp-content/uploads/2021/04/SSI-presentation-final-March-2021_Final.pdf.
UHC (Universal Health Coverage Partnership). 2022. "Ethiopia”. https://extranet.who.int/uhcpartnership/country-profile/ethiopia.
Yilma Z., Mebratie A., Sparrow R., Dekker M., Alemu G. and Bedi A.S. 2015. "Impact of Ethiopia's Community Based Health Insurance on Household Economic Welfare". In The World Bank Economic Review 29(suppl_1): S164–S173. https://doi.org/10.1093/wber/lhv009.
Zelelew H. 2015. "L’assurance-maladie communautaire comme voie vers la couverture maladie universelle: les leçons de l’Éthiopie". Presented at the International Conference on Health Financing in Haiti: Challenges and Perspectives for its Financing. April 28–29 2015 Haiti, Port au Prince, 28 April 2015. https://fr.slideshare.net/HFGProject/cbhi-lessons-from-ethiopia-final-fr
7. France
7.1 Background
The preamble to the French Constitution (1946) states that the Nation "shall guarantee to all, notably to children, mothers and elderly workers, protection of their health". Today, health insurance is the organizational model for the health system in France, where it is one of the five branches of social security. It was first introduced in 1928 and has evolved with social security and health insurance reforms, in particular the creation of social security in 1945, to gradually extend to the entire population regardless of age, state of health, level of income, education or place of residence. The current configuration of health insurance stems from the 2016 Social Security Financing Act and the implementation on 1 January 2016 of Protection universelle maladie (Universal Health Protection, PUMA).
PUMA aims to strengthen equal access to healthcare and enable anyone working or residing in France on a continuous and legal basis, with no break in entitlement, to benefit from cover for their healthcare costs personally and continuously throughout their lives. This means that anyone who works or resides in France on a continuous and legal basis is covered by health insurance:
All adults (aged 18 and over) have their own insurance cover, in two main categories:
-
Those who pay contributions on earned income or replacement income; cover is made on the basis of professional criteria.
-
Those who have a stable residence; cover is made on the basis of residence.
Minors continue to have right-holder status and are attached to one of their parents. However, it is possible to apply for PUMA benefits on a personal basis from the age of 16.
PUMA aims to reduce administrative formalities to the bare essentials, simplify the lives of insured persons, ensure continuity of rights and guarantee greater autonomy and confidentiality for all insured persons in covering their healthcare costs (Nezosi, 2021).
The 2016 Social Security Financing Act abolished the basic UHC scheme, which was aimed at people excluded from compulsory health insurance, and replaced it with a scheme covering healthcare costs on the basis of residence. In addition, the implementation of the law was accompanied from 2018 by the withdrawal of the schemes for the self-employed and students, and the replacement of the Caisse nationale d'assurance-maladie des travailleurs salariés (National Health Insurance Fund for Employed Persons) by the Caisse nationale de l'assurance-maladie (National Health Insurance Fund, CNAM).
7.2 The national social health protection system
Architecture and governance
The French system for covering medical expenses is organized in two stages (described below).
-
The first tier is made up of the basic compulsory health insurance schemes:
-
The general scheme for employees, pensioners, jobseekers and, since 2018, the self-employed, students and beneficiaries of universal health protection based on residence. The general scheme is managed by a network of organizations:
-
At the national level, the CNAM is a national public administrative body operating under the dual authority of the Ministry of Health and Solidarity and the Ministry of the Economy and Finance, with risk management as its primary mission. As part of this role, the CNAM is responsible for implementing “collective” agreements between the Union des caisses d’assurance-maladie (National Union of Health Insurance Funds, UNCAM) and the unions representing the various healthcare professions. It develops medical control of healthcare expenses and promotes the prevention of illness, industrial accidents and occupational diseases. It determines and steers the activities of the network's organizations and manages the health insurance information system.
-
At the regional level, the main remit of the 16 Caisses d'assurance retraite et de la santé au travail (Pension and Occupational Health Funds, CARSAT), which replaced the Caisses régionales d'assurance-maladie (Regional Health Insurance Funds, CRAM) from July 2010, is to support insured persons in difficulty, left in a vulnerable position by illness, accident or disability.
-
At the local level, 102 Caisses primaire de l'assurance-maladie (Primary Healthcare Insurance Funds, CPAM) and four caisses générales de sécurité sociale (general social security funds, CGSS) for the overseas territories are responsible for local relations with insured persons under the general scheme and carry out functions relating to membership, management of health insurance entitlements and processing of treatment forms and health insurance benefits. These funds also draw up annual risk management action plans, in conjunction with health professionals, health prevention and promotion policies, as well as health and social action policies through individual assistance to insured persons, in collaboration with the CARSAT, and collective aid for associations. They also organize visits by health insurance delegates to health professionals.
-
-
The agricultural scheme emerged from the agricultural mutuals created during the nineteenth century, formalized by a specific legal framework with the law of 4 July 1900, which founded the "agricultural mutual insurance" group, and later with the creation of a mutual agricultural benefit society (Mutualité sociale agricole, MSA) in 1930, placed under the supervision of the Ministry of Agriculture. When social security was created, the MSA was maintained under Order No. 45-2250 of 4 October 1945 on the organization of social security, which affirms the principle of the universality of social security and provides for the retention of the wide range of schemes.
The MSA is the compulsory social protection scheme for all agricultural workers and their dependants: farmers, employees (of farms, enterprises, cooperatives and professional agricultural bodies) and labour force employers. It manages all branches of social security: sickness, family, old-age, industrial accidents and occupational diseases, as well as contribution collection. Unlike the general scheme, whose branches are managed by specific funds, including for contribution collection (by the Union de recouvrement des cotisations de sécurité sociale et d'allocations familiales (Union for the collection of social security and family allowance contributions, URSSAF), the MSA is a one-stop shop that manages both benefits and the collection of its contributions.
It is supported by the Caisse centrale de mutualité sociale agricole (Mutual Agricultural Benefit Society Central Fund, CCMSA), a private-sector body responsible for managing a public service, and a network of 35 departmental and inter-departmental mutual agricultural benefit society funds. These funds have a high degree of autonomy and are set up and operate in accordance with the provisions of the Code on Mutual Benefit Societies. They group together a network of 92 production sites (managing contribution collection and benefits) as well as 243 agencies and 349 local offices that see policyholders in person (Cour des Comptes, 2020).
-
The special schemes for certain professions or social groups that already had their own social protection system before the creation of social security. There are 27 special schemes, divided into three main groups:
-
The civil service scheme (civil servants and military personnel).
-
The scheme for public enterprises and establishments.
-
Other schemes structured either on a professional basis (schemes for notary clerks and employees, miners, religious workers, and so on) or on a company basis (schemes for employees of the Paris Opera, RATP, SNCF, EDF-GDF, and so on).
-
The organization and operation of these special schemes are specific to each, with management of the various risks and contribution collection generally divided between the parent company or the institution itself and the specific funds or even the general scheme organizations. With the development of certain professions and industrial sectors, the trend is towards convergence and alignment of the benefits of these schemes with those of the social security system; health risks of some special schemes are now managed in part or in full by the general scheme (Nezosi, 2021).
This first tier is headed by the UNCAM, created by the law of 13 August 2004 on health insurance, which brings together the general scheme and the agricultural scheme. The UNCAM acts in accordance with the health policy objectives and the resulting health plans and programmes, as well as the objectives set by social security financing legislation. In particular, it is responsible for setting reimbursement rates, via agreements with healthcare professionals, co-payments and fixed contributions, and reimbursement rates for medicines. 64
-
The second tier is made up of supplementary schemes, which cover the part of healthcare expenditure not covered and benefits that are not reimbursed at all by the compulsory basic scheme.
A national inter-professional agreement 65 adopted by the social partners in January 2013 extended the general schemes by making complementary health insurance available to all employees. Law No. 2013-504 of 14 June 2013 on securing employment made it compulsory for all private-sector enterprises to offer complementary health insurance to their employees. This extension is also being negotiated for employees of the three public services. Other categories of employees who can take out complementary insurance benefit from tax deductions or lower taxation on their complementary health insurance policies.
There are three major actors in the complementary healthcare sector:
-
-
Mutuals are the main actors in this sector, accounting for 50 per cent of contributions collected.
-
Insurance companies, most of which are for-profit limited companies governed by the Insurance Code. Their business is balanced between individual and group contracts.
-
Social insurance institutions, which are joint bodies (run by employee and employer trade unions) operating on a not-for-profit basis and governed by the Social Security Code. They are particularly active in the field of collective contracts, either for enterprises or for professional sectors.
-
Since November 2019, the Complémentaire santé solidaire (Complementary Health Cover, CSS) has provided complementary health cover free of charge or for a modest financial contribution, which covers the remaining costs of the general scheme. This cover is aimed at insured persons:
-
who have their healthcare covered by virtue of their professional activity or their continuous and legal residence in France; and
-
whose resources are below an amount that depends on the composition of their household. These resources are for the 12 months preceding the application.
From January 2022, the free-of-charge CSS was automatically assigned to new recipients of the Revenu de solidarité active (Active Solidarity Income, RSA). CSS policyholders will have their healthcare costs covered by the health insurance organizations and the management body they have chosen.
It is also worth noting that some local authorities are organizing "communal mutuals" to offer their residents voluntary complementary health cover, by canvassing mutual and insurance companies to negotiate the best prices and cover.
Through these arrangements, 96 per cent of the population is covered by complementary health insurance. The remaining 4 per cent of the population not covered by complementary health insurance is made up mainly of low-income individuals, including the self-employed, the unemployed, the economically inactive and retired people (Pierre and Rochereau, 2022).
Population coverage
Coverage of the national population by the various schemes can be broken down as follows.
Percentage of the national population covered by the various schemes
|
Compulsory health insurance |
||
|
General scheme |
Agricultural scheme |
Special schemes |
|
88% |
5% |
7% |
|
Complementary schemes |
||
|
96% |
||
Source: sécurité-sociale.fr
The legal rate of cover depends on the health insurance scheme, the pathology and the benefits. It is generally 70 per cent for medical and dental benefits, 60 per cent or 70 per cent for other benefits and medical examinations, and 80 per cent for hospital stays. Cover is extended to 100 per cent during maternity and for certain hospitalizations or long-term conditions, as well as for social reasons. Coverage of medications depends on their medical benefit: the rate is 100 per cent for medications recognized as irreplaceable and expensive, 65 per cent for medications with a major or important medical benefit, 30 per cent for medications with a moderately important medical benefit and certain extemporaneous preparations, and 15 per cent for medications with little medical benefit (Ameli, 2021).
Initially, this system was based on the principle of reimbursement: the patient pays the costs in advance and receives a treatment form from the healthcare professional, which must then be sent to the patient's health insurance fund and mutual. Since 1988, with the introduction of the Vitale card, which contains insurance information, and the 2016 law on the modernization of the healthcare system, 66 third-party payment has become widespread. The health insurance fund and complementary insurance company are automatically informed of the treatment provided and reimburse the patient.
As the health insurance system evolves, the trend is towards closer links between the various schemes, with the amounts and payment methods aligned with those of the general scheme.
7.3 Mutuals
Mutuals are the leading provider of complementary health insurance in France, with more than one in two French people covered. They also manage the main non-profit health and social network, with 2,800 healthcare and support services. Mutuals are particularly active in the individual contract segment (where there are only two signatories: the insured person and the insurer), with, in particular, a majority of retired people who, by definition, are no longer eligible for a group contract taken out as part of their professional activity. They are also very active in certain professional categories, such as civil servants. Lastly, some mutuals have volunteered to become CSS accredited organizations, and can be chosen by people eligible for a CSS contract.
Mutuals are a legacy of the mutual aid societies of the eighteenth century. The adoption of the Charter of Mutual Societies in April 1898 founded the mutual society movement and defined the main principles of today's French mutual societies. With the creation of social security in 1945, Order No. 45-2456 of 19 October 1945 on the status of mutual societies created the Code on Mutual Benefit Societies. This brings together all the French legal texts governing the status, composition and operation of mutual societies, with the specific aim of harmonizing the activities of mutual societies with those of social security, which had become compulsory. The Code on Mutual Benefit Societies has been updated several times, with the current version dated 1 June 2022, section L111-1 of which defines mutual societies as follows: "Mutual societies acquire the status of mutual society and are subject to the provisions of this Code from the date of their registration under the conditions laid down by decree in the Council of State. They carry out action, in particular by means of contributions paid by their members, and in the interests of the latter and their beneficiaries, in terms of a provident fund, solidarity and mutual aid, under the conditions laid down in their statutes, in order to contribute to the cultural, moral, intellectual and physical development of their members and to the improvement of their living conditions. They are managed taking account of the social and environmental challenges of their activity".
Almost all mutuals are members of the Fédération nationale de la mutualité française (National Federation of French Mutual Insurers, FNMF). Created in 1902, the FNMF is the trade association for mutual insurers. It leads the mutual society movement and represents it in dealings with public authorities, institutions and all those involved in health and social protection. The federation has 518 national, regional and local mutuals, including 232 health mutuals, and 17 regional unions.
7.4. Resumption of delegations by the general scheme
Several delegated management mechanisms
In 2017, management of the compulsory health insurance scheme for around 12.8 million people was delegated to accredited organizations:
-
5.3 million civil servants and judges and 1 million local authority and hospital employees were covered through the civil service scheme.
-
1.8 million students through the student scheme.
-
4.7 million self-employed workers through the Social Security Scheme for the Self-Employed (RSI) (CSS, 2019).
The civil service scheme and the student scheme were based on the delegation of the management of compulsory health insurance to mutuals by the general scheme. The RSI was a one-stop shop for the self-employed and grouped together the management of several branches of social security. Among these, the RSI's health insurance branch was organized according to the principle of delegating management to accredited organizations.
A series of reports between 2013 and 2016 led the National Assembly and the Cour des Comptes (French National Audit Office) to call into question delegated management. Student health insurance was integrated into the general scheme in 2017. Similarly, the RSI was dissolved on 1 January 2018 and withdrawn permanently on 1 January 2020, and in recent years there has been a significant move towards alignment between mutuals and the CPAM in the management of health insurance for civil servants.
The civil service scheme
Civil servants, who already benefited from a special health insurance scheme under which benefits were provided by mutuals, were granted a special health insurance scheme when social security was created, which entrusts the management of the compulsory health insurance scheme for civil servants to mutuals in accordance with the principle of delegated management. Under the 1947 law, 67 which set up this scheme for civil servants, the health insurance scheme is required to delegate the management of compulsory health insurance for civil servants to mutuals, which are not themselves able to refuse such delegation. However, the scope of this delegation is narrower than that of the Health Insurance Fund; mutuals do not handle industrial accidents or occupational illnesses.
Management of sickness benefits is split between mutual benefit organizations for civil servants, depending on the ministry to which they are assigned, a specific national fund for military personnel (the Caisse nationale militaire de sécurité sociale (National Military Social Security Fund, CNMSS) and through mutuals or the general social security scheme for local authority and hospital employees (who may opt for one or the other). Since 2013, the Cour des Comptes has been questioning the methods, amounts and efficiency of remuneration paid to mutuals, leading to a reduction in their remuneration. Faced with a fall in workforce numbers, almost all mutuals for civil servants have gradually made the financial choice of transferring all or part of their management activities to the general scheme, believing that their size and the reduction in the amount of management remuneration no longer enable them to carry out their activities under optimum conditions.
These mutuals currently manage compulsory health insurance for civil servants in three main ways:
-
Some mutuals, such as the Mutuelle générale de l'éducation nationale (National Education General Mutual, MGEN), continue to manage health insurance using their own tools, thus maintaining integrated management of the compulsory and complementary schemes.
-
Others manage compulsory health insurance but outsource the IT tools used by the CNAM.
-
Lastly, the majority of mutuals have transferred the management of compulsory health insurance to the CNAM, whose IT tools they use for certain functions (enrolment, and so on). Coverage is thus integrated into the general scheme, with the mutuals retaining their proximity to policyholders and continuing to offer complementary insurance products (Viel, 2018).
The student scheme
The law of 23 September 1948 68 extended the health insurance scheme for salaried workers to students and entrusted its management to a national mutual (La Mutuelle des étudiants – LMDE) as part of a public service delegated management initiative (CAS, 2015). From 1972 onwards, a number of regional mutuals developed and took part in the management of compulsory health insurance, also offering complementary health insurance.
Several reports by the Cour des Comptes (2002, 2006 and 2013 reports) and by the Inspectorate General of Social Affairs (IGAS) and the Inspectorate General of Finance (IGF) in 2013 criticized the cost of managing health insurance by student mutuals (CCSS, 2013). Faced with cases of embezzlement and misuse of company assets, as well as major failings (including abnormal delays in reimbursements and in issuing the Vitale card) and massive debt, the LMDE has been attached to the general scheme for the management of compulsory health insurance since 2015 following judicial safeguard proceedings.
The 2017 law on guidance and success of students (ORE) put an end to delegated management of the compulsory part of health insurance for students. Since 1 September 2019, students have been integrated into the general scheme and attached to the CPAM in their place of residence. However, student mutuals will continue to offer and manage complementary health insurance.
Below are the failings noted by institutions and student and consumer organizations:
-
Distorting the preventive actions for which mutuals receive funding by turning them into communication campaigns to gain market share over the competition for the management of the compulsory part of insurance and to sell supplementary health insurance.
-
A growing number of universities are refusing access to campuses to some mutuals accused of misinforming students across the board about the delegated scheme and their business of selling supplementary products, in order to maximize their profits.
-
The particularly high cost of the management delegation system, with the Cour des Comptes estimating that management rebates were funding some of the expenses linked to the sale of complementary health insurance, even though student mutuals carry out this activity in the same way as any other mutual or insurance company.
-
Overall, a number of failings have penalized students by limiting access to healthcare under proper conditions and causing them to forego treatment.
The Social Security Scheme for the Self-Employed
The Social Security Scheme for the Self-Employed (RSI) was set up in 2006 with the aim of simplifying social protection for craft workers, shop owners, service providers and sole proprietorship owners and members of the liberal professions, by merging several social security institutions and creating a single point of contact for all social security formalities.
Since its creation, the RSI has been faced with many vicissitudes: problems processing and monitoring contributions, late payments and financial losses. Many failings resulted from the merger of social security institutions, which had different working practices and internal procedures and incompatible IT systems.
The RSI was dissolved in 2018 and withdrawn permanently on 1 January 2020, and its policyholders are now part of the general social security scheme, which covers their health risks (through the CPAM) and old age (through the CARSAT) and collects their social security contributions (through the URSSAF).
The health insurance branch of the RSI was organized on the principle of delegating management to organizations, mutuals and insurance companies, known as "accredited organizations" (AOs). In this connection, the RSI national fund concluded delegation agreements specifying the geographical scope of AO intervention provided that they complied with the following conditions:
-
belong to one of the categories listed in section R611-79 of the French Social Security Code, in other words: mutual insurers, insurance companies or groups of insurance companies
-
provide guarantees of their ability to fulfil the scheme's management obligations
-
analytical accounting to identify expenditure relating to the management of the RSI health insurance scheme
-
have financial guarantees
-
Have a reception facility in each of the districts where the AO is authorized to operat
Section R611-83 of the Social Security Code gave the RSI the option of terminating the agreement with the AOs if the above conditions were no longer met, or in the event of mismanagement or obstruction of the RSI's control, or if the number of insured persons managed by the AO failed to reach 23,000 for a period of two consecutive years (Ravignon et al., 2013).
Financing
The legal framework for the reimbursement to mutuals of statutory benefits paid to civil servants and the corresponding management costs is defined in section L. 712-7 of the Social Security Code, specified by a decree dated 27 April 2017. This decree organizes the management delegations implemented for the coverage of healthcare costs, within the general scheme for civil servants and students, and within the social scheme for the self-employed. It sets out the procedures for organizing, implementing and financing these management delegations, in particular within the framework of agreements, as well as the conditions under which they may be terminated. 69
The actual benefits are reimbursed directly to the mutuals by the health insurance fund on the basis of standard agreements. The amount of reimbursement of management costs (management rebates) that they receive in return for delegated management does not necessarily correspond to their management costs, which depend on their own productivity.
The objectives assigned and the remuneration of delegated management are set out in multi-year management contracts negotiated between the mutuals and the CNAM or the CPAM. Although these contracts are not agreements on objectives and management, they do include performance indicators (which are different for civil servant mutuals and student mutuals), which are used to determine surcharges or penalties. The method for calculating management rebates is complex and applied differently depending on whether the management of civil servant mutuals or student mutuals was involved. It is based on several elements, which are simplified here:
-
For civil servant mutuals
-
number of active beneficiaries of mutuals, defined as an insured person or a beneficiary who has received health or maternity insurance benefits at least once during the year
-
average cost of managing an active beneficiary in primary healthcare insurance funds
-
performance coefficient set by agreement and applied to this cost in order to take into account the tasks carried out by the CPAM that are not carried out by the mutuals: relations with the health professions, management of daily allowances, risk management, and so on
-
profit-sharing system in the form of bonuses if the targets set in the multi-year management contract are achieved, or penalties if they are not
-
additional remuneration for processing cash benefits for non-permanent staff
-
For student mutuals
-
number of active mutual policyholders
-
average cost of managing an active beneficiary in the 50 best-performing CPAM and electronic processing centres
-
rate of change in each mutual's headcount weighted by CPAM productivity efforts
-
performance coefficient in the same way as for civil servant mutuals
The annual unit amount of management rebates paid to student mutuals was set at €46 per member in 2017. 70
It should also be noted that civil servant mutuals receive subsidies and free services from the State, in the form of services made availability to civil servants, premises, equipment and services.
Delegated functions
The management delegated to civil servant and student mutual insurers covers benefits in kind for sickness, maternity and invalidity insurance. However, it does not include the payment of cash benefits or the management of industrial accidents or occupational illnesses. Mutual insurers do not have a medical service and are not involved in contractual relations with healthcare professionals. However, they do take part in risk management by carrying out preventive actions such as flu vaccination campaigns and cancer screening.
Distribution of functions (before transfers to the general scheme)
|
Functions |
Distribution |
|||
|
General scheme |
Civil servant mutuels |
Student mutuals |
AO of the RSI |
|
|
Definition of the healthcare package |
Compulsory basic health insurance scheme |
|||
|
Agreements |
X (UNCAM) |
|||
|
Education and promotion |
X |
X |
X |
|
|
Enrolment, membership and renewal |
(1) |
X |
X |
X |
|
Contribution collection |
(2) |
|||
|
Resource mobilzation |
||||
|
Pooling of risks covered |
X |
X |
X |
|
|
Payment of benefits |
X |
X |
X |
|
|
Healthcare services |
(3) |
|||
|
Follow-up and steering |
X |
(4) |
||
-
-
-
Local authority and hospital employees belong to the general scheme or to a mutual depending on their department of residence.
-
In all systems, contributions are collected by the URSSAF. Under the RSI, the AOs collect contributions from members of the liberal professions.
-
Some mutuals, including the MGEN, run healthcare and support services.
-
Follow-up by the national and local RSI funds.
-
-
7.5 Impact and lessons learned
As mentioned above, between 2002 and 2013, several reports by the Cour des Comptes and the Inspectorate General of Finance highlighted the failings and high costs of delegated management for civil servants and students.
These reports mentioned:
-
A fragmentation of the SHP system, with multiple mutuals for civil servants and students.
-
Management costs higher than those of the general scheme. Various reports found that the remuneration of mutuals was too high. In 2013, the management cost per beneficiary in the two largest mutuals for civil servants was €51.10 for the MGEN and €63.79 for the Mutualité function publique (Public Service Mutual Society, MFP), compared with €43.67 for the Caisse nationale de l’assurance-maladie des travailleurs salariés (National Fund for Employee Health Insurance, CNAMTS). In the case of student mutuals, the management cost per delegated body and per member was, in some mutuals, up to 64 per cent higher than that of the general scheme, despite a low quality of service (Ravignon et al., 2013).
-
The quality of service was judged to be highly questionable in the case of student mutuals, with delays in enrolment and in obtaining a Vitale card, a low rate of computerization of data flows and reimbursement delays of up to a year, as well as a lack of telephone response to complaints. This assessment was more complex for civil servant mutuals, some of which also experienced long delays in processing policyholder files and low rates of response to claims.
-
In addition, these various reports pointed to new challenges for civil servant mutuals, linked to the fall in recruitment and changes in the status of civil servants. In addition, these mutuals, as well as student mutuals and the mutual society movement in general, were faced with the need to adapt to a sector in the throes of transformation, notably with the implementation of the European Solvency II Directive, 71 which imposed new prudential rules as well as governance and operating rules on financial communication.
All the reports and discussions converged on the proposal to put an end to the delegation of management and to transfer these schemes, particularly the student scheme, to the general scheme. This end to delegation was seen as a source of simplification and improvement in the quality of services for insured persons and a rationalization of management costs.
With the law of 8 March 2018 on guidance and success of students and the law on social security financing for 2018 abolishing the RSI, the latter and the student scheme were transferred to the general scheme. In addition, many civil servant mutuals opted to end their delegation. As a result, of the 12.8 million beneficiaries affected by the delegated management of compulsory health insurance in 2017, some 8.2 million were taken over by the general scheme between 2018 and 2020, including 1.8 million students, 1.76 million civil servants and 4.7 million self-employed workers.
The merger of civil servant mutuals with the general scheme led to the development of new types of partnership:
-
The integration of mutual insurance policyholders into the CPAM, as described above, with them becoming policyholders under the general scheme.
-
The management mandate, whereby mutuals entrust the management of the compulsory part of health insurance to the CPAM but retain the management of relations with policyholders, which remains the responsibility of the mutual.
-
Shared management with, as with the management mandate, a sharing of functions between the CPAM (management of benefits) and the mutuals (management of beneficiaries) and the use of the mutual's data by a general scheme data processing centre.
-
Outsourcing: the mutual manages the compulsory part of the health insurance scheme, using all the tools and data processed by a general scheme data processing centre.
-
Sharing the information system, whereby the mutual also uses the health insurance tools but operates them on its own machines, thus becoming a health insurance data processing centre (CAS, 2015).
At the same time, the law on social security financing for 2016 reorganized the conditions under which these mutuals are delegated the management of the compulsory health insurance scheme. It stipulates that no new management delegations may take place and that "a decree in the Council of State shall determine the terms and conditions for organizing, implementing and financing these management operations", as well as "the conditions under which these management operations may be terminated in the event of failings that make it impossible to manage the compulsory schemes under normal conditions". With the exception of the special MSA scheme, mutuals are now restricted to managing complementary schemes. For local authority employees, the concept of delegation has been replaced since 2017 72 by that of certification, which is issued by the Agence de contrôle prudentiel et de résolution (Prudential Supervision and Resolution Authority, ACPR) for a period of three years. This accreditation enables civil servants and local authority employees to benefit from a contribution from their employer (local authority/public institution) towards their individual complementary health insurance contribution.
Lastly, the transposition of European Union directives, Solvency I in 2002 and Solvency II in 2016, 73 as well as the general expansion of company complementary health insurance in 2016, have forced mutuals to restructure and seek alliances and partnerships in order to achieve critical size and have led to mergers. According to the ACRP, the number of mutuals operating in the complementary health insurance market fell sharply in the early 2000s, from 1,528 in 2002 to 310 in 2019 (Adjerad, 2020; Boned et al., 2018).
References
Adjerad R. 2020. Rapport 2020 : Sur la situation financière des organismes complémentaires assurant une couverture santé. DREES, October 2020. https://drees.solidarites-sante.gouv.fr/sites/default/files/2020-12/rapport-oc-2020.pdf.
Ameli. 2021. "Remboursement des médicaments et tiers payant". Ameli.fr health insurance website, October 2021. https://www.ameli.fr/assure/remboursements/rembourse/medicaments-vaccins-dispositifs-medicaux/remboursement-medicaments-tiers-payant.
Boned O., Guerry R. and Pierron L. 2018. "Les mutuelles de santé face à la réglementation européenne: une banalisation de l'identité mutualiste?" In RECMA 349(3): 42–55. https://shs.cairn.info/revue-recma-2018-3-page-42?lang=fr.
CAS (Commission des Affaires Sociales). 2015. "Mission d'évaluation et de contrôle des lois de financement de la sécurité sociale sur la gestion du régime de l'assurance-maladie obligatoire par certaines mutuelles, Rapport d'information N° 3316". Commission des Affaires Sociales, Assemblée Nationale, Paris, December 2015. https://www.assemblee-nationale.fr/14/rap-info/i3316.asp.
CCSS (Cour des comptes de la sécurité sociale). 2013. "Rapport sur l'application des lois de financement de la sécurité sociale". Paris, September 2013. https://www.securite-sociale.fr/files/live/sites/SSFR/files/medias/CCSS/2019/CCSS%20SEPT%2019%20DEF.pdf.
Cour des Comptes. 2020. "La mutualité sociale agricole". Paris, May 2020. https://www.ccomptes.fr/fr/publications/la-mutualite-sociale-agricole-msa.
CSS (Comptes de la sécurité sociale). 2019. "Les comptes de la sécurité sociale : Résultats 2018 - Prévisions 2019 et 2020, Rapport (volume 2)". Commission des comptes de la sécurité sociale (CCSS), October 2019. https://www.securite-sociale.fr/files/live/sites/SSFR/files/medias/CCSS/2019/CCSS%20SEPT%2019%20DEF.pdf.
Nezosi G. 2021. "La protection sociale : 2e édition" . In Découverte de la vie publique. La Documentation française, 2021.
Pierre A. and Rochereau T. 2022. "The Non-Coverage of Complementary Health Insurance in France in 2019: Initial Findings of the European Health Interview Survey (EHIS)". In Questions d’économie de la santé/Issues in Health Economics No. 268, May 2022. https://www.irdes.fr/english/issues-in-health-economics/268-the-non-coverage-of-complementary-health-insurance-in-france-in-2019.pdf.
Ravignon B., Cayre V., Gardette C., Chastel X., Laurenty A. and Auvigne F. 2014. "Les coûts de gestion de l'assurance-maladie (MAP)". Inspection générale des Finances/Inspection générale des affaires sociales, September 2014. https://www.igas.gouv.fr/Les-couts-de-gestion-de-l-assurance-maladie-MAP.
Viel L. 2018. "Les fonctionnaires en pleine rupture". L'Argus de l'assurance, 8 March 2018. https://www.argusdelassurance.com/acteurs/les-fonctionnaires-en-pleine-rupture.127270.
8. Germany
8.1 Background and development of the national social health protection system
With the adoption of the Health Insurance Act on 15 June 1883, 74 Germany became the first country to introduce compulsory social insurance, giving rise to the so-called "Bismarck" model, which is still used today in German health insurance and in a number of other European countries, such as France and Belgium.
Paradoxically, Germany is still the only European country not to have introduced universal health coverage. The 1883 Act introduced compulsory occupational insurance for some categories of workers, with a twofold limit: first, it only covered blue-collar workers; and, second, incomes could not exceed a certain ceiling (three times the average wage). Farm workers were not initially covered, but were included following a law passed in 1886. Similarly, in 1892, insurance was extended to some civil servants, subject to the same income conditions, and to employees in the liberal professions, then in 1903 to clerical staff and apprentices, again subject to the same conditions.
In contrast, a reform of the health system in 1888 excluded certain categories of self-employed people from statutory insurance, as the legislator considered that they did not need protection. These socio-economic groups set up emergency funds and insurance outside the public health insurance system, thereby giving greater importance to private insurance. Despite changes in the system, this approach prevails today and continues to encourage certain workers to take out private insurance (Sénat, 1999). A 2007 reform law introduced compulsory health insurance for all people who should be covered by public insurance but who, for various reasons, are not yet covered by it. This requirement was extended in 2009 to the categories of people excluded from the public scheme who are covered by private insurance, making health insurance compulsory for all.
Another feature of German public insurance since its creation is its decentralized organization. Management of the scheme was entrusted to various types of company, trade guild or mutual aid funds, as well as to sickness funds set up by the federal states, which existed prior to the 1883 Act. These funds were integrated into the public insurance system, provided that their statutes and operating methods complied with the legal provisions. The Act also provided for the creation, by municipal decree, of local funds for insured persons in a specific branch of industry, or even for a local enterprise, of general municipal funds as well as specific sickness funds for construction companies, reserved for major public works sites.
Germany thus had highly diverse and decentralized health insurance funds, with a significant change following the implementation of the 1992 structural reform law (known as the "Seehofer Reform" after the then Minister of Health). 75 This reform initiated a structural change in public insurance to bolster efforts to control healthcare expenditure that had been under way since 1970. The aim of the 1992 reform was to establish a strict budgetary framework for all insurance expenditure and to strengthen the federal government's supervision of the health insurance system. Another aim was to change the way public health insurance funds were organized by introducing inter-fund competition, leaving insured persons free to choose their own fund. In addition, it promoted fund mergers so as to encourage the funds to make efforts to control non-medical costs and to improve their influence compared to doctors' unions, which until then had been in a strong negotiating position (Hassenteufel, 2014). The public health insurance landscape has therefore changed significantly, with the number of public health insurance funds falling from 35,000 at the end of the nineteenth century to 105 in 2022.
A final key feature of the German social health protection (SHP) system was the high degree of autonomy enjoyed by funds, which until 2007 were free to set their own contribution rates. This autonomy resulted in a wide spread of contribution rates owing to the unequal distribution of risks between funds, depending on the place of work, professional status and other specific characteristics of insured persons. In order to promote the principle of solidarity underpinning the public health insurance system, the 2007 reform law established a new method of financing in the form of a health fund (Gesundheitsfonds) and introduced a single contribution rate set by the government. This measure was accompanied by a compensation mechanism between the funds, based on various criteria (medical care consumption, age, gender, geographical area, and so on).
8.2 The national social health protection system
Architecture and governance
Since the Health Insurance Act of 1883, Germany's national SHP system has been based on a dual structure with, on the one hand, public health insurance, also known as “statutory” (gesetzliche Krankenversicherung – GKV) and, on the other, private health insurance (private Krankenversicherung - PKV) (Kaufmann, 2016).
-
Public health insurance is a branch of German social insurance. It is characterized by its diverse organization and decentralized management. Several types of sickness funds, all of which come under Book V of the German Social Code (SGB), 76 are involved in the management of public health insurance:
-
Allgemeine Ortskrankenkassen (AOK): General local funds set up by one or more municipalities for the same industrial sector. They group together insured persons according to their place of work or residence. Insured persons who do not belong to another fund must be members of a local fund. Following the reforms in the 2000s, the local funds were gradually turned into regional funds, which not only improved risk pooling but also strengthened the position of this type of mutual in the competitive environment since the 1992 structural reform.
-
Betriebskrankenkassen (BKK): Employers may set up their own fund if they employ at least 1,000 employees subject to compulsory health insurance, if their ability to pay contributions is guaranteed in the long term, if the creation of the company fund does not jeopardize any local fund, and the majority of the company's employees approve this measure. Insured persons in voluntary schemes may also join.
-
Innungskrankenkassen (IKK): Trade guild funds organized by profession for colleagues and apprentices. They have been set up within guilds or by enterprises in the same sector of activity and grouped together at territorial division level, which employ at least 1,000 employees subject to compulsory health insurance. The conditions for their creation are more or less the same as for company funds.
-
Socio-professional funds:
-
Landwirtschaftliche Krankenkasse (LKK): Agricultural fund;
-
Knappschaft-Bahn-See (KBS): Fund for miners, railway workers and seafarers.
-
-
Ersatzkrankenkassen: Approved voluntary health insurance funds for white-collar and blue-collar workers, also known as “substitute funds”. These mutual funds are managed solely by the insured persons. Membership of these funds is subject to special conditions and the categories of people who may join are determined by the statutes of the funds, not by the law; the substitute funds may therefore limit their personal scope of application. These funds are also category-based, with funds for employers and others for workers. Substitute funds have proved to be in strong competition with local funds, with these two types of fund covering 37 per cent and 40 per cent, respectively, of insured persons under the public system in 2006. However, their contribution rates and benefits have had the effect of directing the most disadvantaged people and bad risks (people at high risk of illness, and so on) back to the local funds. This situation led to the introduction of a number of measures in the 1990s to limit competition from these funds, in particular by prohibiting the creation of new substitute funds and limiting their geographical area
Since the creation of health insurance in 1883, membership of a particular fund has depended on the individual's socio-professional affiliation or place of residence. With the 1992 structural reform and the introduction of competition between funds, each insured person now has the right to freely choose his or her fund (with the exception of the agricultural, mining and seafaring sectors). Thus, the traditional distinction summarized above has basically lost its original meaning.
Health insurance funds are fully autonomous public-law bodies. They are managed administratively and financially by a governing body made up of social partners or, in the case of substitute funds, insured persons. The Länder ministries and the Federal Ministry of Labour and Social Affairs oversee the funds. As insurance companies, they are also subject to financial control, either by the Länder or, in the case of federal funds, by the Insurance Board (Sénat, 1995).
The funds are grouped into regional associations and a national federation. These groupings perform important functions for the member funds in terms of representing their interests at a political level and, in particular, in negotiating and concluding contracts with healthcare providers. Through this national federation or their regional associations, the funds conclude contracts with doctors' associations, clinics and pharmacies and determine the amounts they will pay for various medical treatments (Federal Ministry of Health, 2020).
The national federation is a federal structure governed by public law, created by the 2007 law and employing around 100 people. Its creation reduced the role of the federal structures that previously existed for each type of fund, which lost their status as public-law organizations in 2009. This development is part of the process of increasing oversight of the self-administration of the funds by the federal government. The federal government is setting increasingly stringent rules and has acquired greater powers to monitor, control, evaluate and impose sanctions on all stakeholders in the health insurance sector (Hassenteufel, 2008).
Last but not least in the evolution of funds, is the change in the health insurance landscape following the reform process undertaken in 1992. As well as encouraging competition, the aim of the reform was to promote the grouping of funds in order to better cope with budget constraints resulting in particular from the high number of insured persons “at risk” or economically disadvantaged in the case of funds established in certain geographical areas. The grouping of health insurance funds is voluntary and the number of such funds has risen steadily since 1883; however, this fell sharply as a result of the acceleration of mergers between funds from the 1990s onwards (Kaufmann, 2016). There were 35,000 health insurance funds at the end of the nineteenth century, then 6,000 in the 1930s and around 1,140 in the early 1990s, before the Seehofer Reform. With the Seehofer Reform, the number of funds quickly decreased, and by 2022 the system had only 105 funds (Federal Ministry of Health, 2020).
-
Private health insurance: Persons who do not fall within the scope of statutory health insurance or who have the right to refuse membership or the right to opt out of statutory health insurance because of their salary level (more than €60,750 per year in 2019) may take out private health insurance. Insurance premiums are graduated, depending on the benefits chosen by the member and the risk assessed, taking into account the person's general state of health, age and gender, and so on. German private health insurance companies can generally refuse to take out insurance with applicants who present health risks. However, in order to guarantee cover for the entire population, private insurance companies have been required since 2009, like public funds, which have been required to do so since 2007, to accept applications for membership from anyone who has at some time been privately insured or who meets the conditions when applying for membership and who is not entitled to be insured under the public health insurance scheme.
Private insurers must also offer a basic health insurance contract, which provides benefits comparable to those provided by statutory health insurance, at a capped price. Members must pay invoices for medical treatment themselves and are then reimbursed by their private insurer under the terms of their policy. Members of the insured person's family cannot be co-insured and are each subject to an additional premium.
Private insurance can also supplement public insurance. This is either “comfort” or “lifestyle” insurance or insurance to cover health costs not covered by social insurance. Such a contract may provide for choices in hospitalization, treatment provided by a certain category of doctor, dental care that is not otherwise reimbursed, alternative treatments and other benefits (Berton, 2019).
Population coverage
Around 87.7 per cent (72.7 million people) of the population in Germany is currently covered by public health insurance fund schemes, 10.5 per cent (8.7 million) by private insurance companies (high-income households) and 1.8 per cent (1.5 million) by special schemes or with no cover at all. The latter group includes those receiving social welfare payments or a military invalidity pension, as well as specific groups, such as army and police officers whose medical care is provided free of charge. Around 0.1 per cent of the population is said to have no cover at all, mainly due to a lack of information about health insurance (Federal Ministry of Health, 2020).
Public insurance covers two main categories of insured persons:
-
Some 75 per cent are compulsorily insured, which includes employees, provided their income does not exceed the statutory ceiling, paid apprentices, students, certain self-employed people (farmers, artists, and so on), pensioners covered by the statutory pension scheme and the unemployed. Dependants (spouse and children) are also covered by public health insurance, without any additional contribution.
-
Voluntary membership, which is generally only possible if an individual was previously covered by public insurance. These include employees whose income exceeds the membership ceiling, but who may remain members of the statutory scheme on a voluntary basis. This also applies to people who cease to be beneficiaries of an insured person, children whose parents have too high an income, persons who are working for the first time and who exceed the ceiling for membership of the statutory compulsory insurance scheme, and employees returning from a long stay abroad (Sénat, 1995).
Individuals not covered by the public insurance scheme are primarily employees whose remuneration exceeds the legal ceiling and who do not opt for voluntary membership of the public scheme. These individuals may take out private insurance. In this case, the employer is obliged to contribute to the scheme chosen by the employee. They are often single people with incomes above the membership ceiling, for whom private insurance premiums may be more attractive, unlike married individuals whose spouse and children are covered as beneficiaries under the public scheme. In addition, almost half of privately insured persons are civil servants whose government covers half, or even up to 80 per cent, of the healthcare costs incurred, with private insurance covering all or part of the remainder (Kaufmann, 2016).
Healthcare package
The scope of public health insurance is determined by Book V of the German Social Code and the benefits provided by the funds are in principle limited to those laid down by law, with consequently little difference from one fund to another. Public health insurance covers a full range of benefits in kind, including preventive services, inpatient and outpatient care, dental care, rehabilitation and prescribed medications. General and specialist care is provided in private practices or outpatient clinics and inpatient care in public and private hospitals; the country also has many not-profit organizations involved in the provision of healthcare. Insured persons have a free choice of practitioner, provided that the practitioner is approved by the health insurance fund to which they pay contributions. They are also free to choose the approved hospital to which they wish to be admitted.
The public health insurance package is determined by the Federal Joint Committee (Gemeinsamer Bundesausschuss G-BA), within the framework of health legislation and taking into account the current state of medical science, the analysis of therapeutic efficacy, the medical need for the services selected and their cost-effectiveness. This committee also decides on measures to safeguard the quality of outpatient and inpatient care. It brings together insurance funds, doctors, dentists, psychotherapists and hospitals (Kaufmann, 2016). By law, however, the funds cannot offer complementary healthcare products (Boned, 2008).
Cover is provided through a general third-party payment system, although co-payments are made for certain services, including hospitalization and medicinal products selected according to their packaging (to encourage the use of generic drugs) and therapeutic class. As mentioned below, membership by insured persons increased with the law on the modernization of the healthcare system in 2003. The poorest people and young people are exempt from co-payment (Sénat, 1995).
Healthcare providers are reimbursed in accordance with the procedures laid down by the regional federations of health insurance funds and the regional associations of doctors within the national framework set by the Federal Joint Committee. These providers send the invoices for patients from the various health insurance funds to the corresponding regional organizations for reimbursement. The organization monitors the volume and cost of each practitioner's services.
Financing
Until the 2000s, the German system was characterized by a high degree of autonomy for the public health insurance funds, which were able to determine their contribution rates within the limits set at the federal level. However, this autonomy and high number of funds led to a wide spread of contribution rates: on 1 January 1992, the two extremes were 8 per cent and 16.5 per cent. With the introduction of competition between funds, this situation proved to be a source of inequality. Some funds, especially the substitute funds, attracted individuals with the “safest” profile, in other words, those with substantial financial resources and the lowest risk of morbidity, which enabled them to offer lower contribution rates. On the other hand, local funds, whose membership was not subject to any conditions, were at a disadvantage. They could not refuse “high-risk” insured persons or those on low incomes with, as a result, a disadvantageous policyholder structure, forcing them to set higher contribution rates.
In addition, due in particular to the impact of reunification in 1991, but also to constant increases in healthcare consumption and expenditure, public health insurance experienced a difficult financial situation in the 1990s, with record deficits in 1991–92 and again in 1995 and 1996. The system's financial equilibrium was restored from 1997 onwards, but it remained fragile, which led the various governments to act on this equilibrium by increasingly intervening directly in the regulation of the entire system (Autret, 2001).
The reform package of the 2000s introduced a strict financial framework for health insurance in order to establish a principle of fiscal balance and reinforce the principle of solidarity on which public insurance is based. The law to modernize the healthcare system, which was passed on 19 November 2003 and came into force on 1 January 2004, introduced measures involving a sharp increase in the financial contribution (introduction and increase of co-payments) made by insured persons towards the cost of healthcare, and the exclusion of certain services (“lifestyle” medications, spectacle frames and lenses, spa treatments, and so on). This law also encouraged greater use of taxation to finance health insurance. Despite a positive effect on the health insurance funds' financial situation, it remained fragile, with deficits forecast from 2007 onwards (Vasselle and Cazeau, 2006). For this reason, the 2007 reform law 77 introduced a new method of financing public insurance with the creation of a health fund (Gesundheitsfonds) financed by contributions from employees and employers on the basis of a single contribution rate set by the government. This uniform contribution rate was 14.6 per cent in 2019, divided equally between the insured person and their employer. This health fund is supplemented by public subsidies from the State, which finance, in particular, cover for beneficiaries, especially children (Vasselle and Cazeau, 2006).
As a result of these various reforms, public funds are now financed by:
-
A lump sum paid by the healthcare fund to the funds for each insured person.
-
This amount is increased by the fund according to the cost of care, age, gender, number of dependants, level of resources and health risks. The aim of this increase is to reduce risk selection by taking into account the disparities between insured persons in the various funds (Hassenteufel, 2014).
-
In addition, funds that are unable to cover all their expenses with the amount paid to them are authorized to levy an additional contribution, the amount of which is payable solely by the insured person, with companies making no contribution. The limit of €8 per month or 1 per cent of the insured person's gross salary was abolished in 2011. However, if the amount of additional contributions exceeds 2 per cent of salary, state funding is provided to reduce the burden on insured persons (Bas-Theron, 2002). This additional contribution is now the main source of competition between funds, as employees have the right to change fund without notice. Conversely, when health insurance funds have a surplus, they can pass this on to their policyholders by offering discounts (Schmucker, 2010).
8.3 From delegated management to governance from a distance
Legal framework
The Basic Law for the Federal Republic of Germany of 1949 defines Germany as a democratic and social federal state. Within this framework, the State delegates a large proportion of public policy to the 16 Länder. However, social policy, including on nursing care and social security, remains a federal legislative responsibility, and the public health insurance system is overseen by the Federal Ministry of Health, which is responsible for compulsory health insurance and nursing-care insurance. The Federal Assembly, the Federal Council and the Federal Ministry of Health are responsible for legislative and supervisory functions. The federal legal framework, in particular the Social Code, regulates the governance, the services to be provided and the financing mechanisms of the healthcare system, with no room for legislative initiative by the Länder (Eichenhofer, 2006).
Since its creation, the organization of the health insurance system has been delegated by the Bismarck Reich and then by the Federal Republic to autonomous health insurance funds, based on the principle of self-management. Broadly speaking, "the State lays down the legal framework and defines the tasks, while the insured persons, the contributors and the service providers organize themselves into associations that are responsible for providing the population with access to medical care under their own responsibility" (Federal Ministry of Health, 2020).
This delegated management model enables the State to influence the development of the overall system, while at the same time freeing itself from direct administration and making use of the expertise of those directly involved, both insured persons and healthcare providers.
However, with the reforms initiated in the 1990s, this system has evolved towards a model of organized competition, accompanied by a reorganization of the range of healthcare services on offer. This development is also reflected in the increased supervision of the health insurance system by the federal government, which is often described as “government from a distance” (Hassenteufel, 2014).
Distribution of functions
Today, the governance and regulation of the insurance system is based around the Joint Federal Committee created in 2003, and the National Association of Statutory Health Insurance Funds (GKV-Spitzenverband), created in 2007. These two public-law institutions employ salaried staff and operate as quasi-agencies with considerable expertise, under the supervision of the Ministry of Health. The creation and professionalization of these bodies reflect the centralization and strengthening of the federal government's management and oversight of health insurance. These two institutions are involved in implementing the policies set out by the federal government. They oversee and mediate in negotiations between doctors, hospitals and health insurance funds.
The public health insurance package of services is determined by joint committees made up of the health insurance funds, healthcare providers and representatives of healthcare users (without voting rights for the latter). They are governed at federal level by the Joint Federal Committee, which has regulatory powers and whose decisions determine the services covered by compulsory health insurance, the standard requirements for the provision of these services and the quality management measures for these services (EU, 2012).
With the introduction of the National Health Fund, the public health insurance funds, which previously set their own contributions and managed them directly, lost their autonomy over management. Today, they now only collect contributions, which are set at a single rate by the State, and pay these contributions to the National Health Fund. The latter, under the authority of the Federal Insurance Office, collects together all the sources of funding for health insurance, in other words, employee and employer contributions and the tax resources allocated to it. As mentioned above, the National Health Fund redistributes these resources to the funds in the form of a lump sum per insured person plus a supplement designed to reduce disparities between insured persons in the various funds. This equalization shifts the pooling of resources and risks to the national level. The funds that levy additional contributions collect and manage them directly.
As already mentioned above, the negotiations and agreements between health insurance funds and healthcare providers are governed at regional and national level by the Joint Federal Committee. However, the law on the modernization of the healthcare system adopted in 2003 allows health insurance funds to set up medical care centres including doctors and other healthcare professionals to provide more integrated patient care. This possibility bypasses the contractual monopoly with the doctors' unions and allows new types of healthcare contracts and organization to be put in place, promoting better patient follow-up, within healthcare networks and channels, and relying on the strengthened pivotal role of general practitioners.
The Medical Service is a "multi-scheme" service, organized regionally and independent of the funds. It is responsible for overseeing the appropriateness of care and for appeals by insured persons against fund decisions. The committee's decisions may themselves be challenged before the Social Affairs Tribunal. The Medical Service is increasingly involved in public health initiatives relating to the efficiency and organization of the healthcare system. The Medical Service is involved in an internal certification and quality assurance process and has its own regional experts in different specialist areas on which practitioners can call (Descamps et al., 2001).
Oversight of the legality and activities of the funds is divided between the federal level, the Länder and the municipalities. The Federal Insurance Oversight Office is responsible for overseeing statutory health insurance funds organized at the federal level. For funds organized at the Land level, oversight is the responsibility of the Ministry of Health of the Land where the fund has its head office. Cities undertake oversight and intervene in disputes at the local fund level.
Distribution of functions
|
Functions |
Distribution |
|||||
|
Federal state |
Länder/municipalities |
Funds |
Medical Service (region) |
|||
|
Joint Federal Committee (G-BA) |
National Health Fund |
National Association of Statutory Health Insurance Funds |
||||
|
Definition of the care package |
X |
|||||
|
Agreements |
X |
|||||
|
Education and promotion |
X |
|||||
|
Enrolment, membership and renewal |
X |
|||||
|
Contribution collection |
X |
|||||
|
Pooling of risks covered |
X |
|||||
|
Payment of benefits |
X |
|||||
|
Healthcare services |
X |
|||||
|
Complaints management and quality assurance |
X |
|||||
|
Follow-up and steering |
X |
X |
X |
|||
8.4 Impact and lessons learned
The German health insurance system as it stands today is the result of a long process of change, particularly over the last 20 years. Public health insurance has undergone a gradual transition, moving from a system of delegated management to a variety of decentralized public insurance funds with complete autonomy over management, to a system that is increasingly supervised by the federal state and which now seems to be moving towards a national health system managed by the State (Hassenteufel, 2014).
The dynamics of this transition is reflected in a number of ways:
-
Increased budgetary oversight of the health system by the State in order to bring the growth in healthcare expenditure under control. The State now intervenes in a system that was previously self-regulating, in particular to set and increase co-payments and reduce reimbursements;
-
The federal government now sets contribution levels, which are centralized and then redistributed by the national health fund using an equalization mechanism, for the funds, which thereby lose much of their management autonomy;
-
A structural change, giving individuals the opportunity to freely choose their health insurance fund, meaning that health insurance funds with a membership that was previously based on socio-professional membership or place of residence are now in competition. Similarly, the reforms of the 1990s accelerated the process of mergers; there are now around 100 funds, compared with several thousand at the start of the system. These various measures have evened out the significant diversity previously found in the German system;
-
Intervention at the central level, through the Federal Joint Committee, in healthcare provision negotiations, which was traditionally self-administered through collective bargaining between the health insurance funds, doctors and hospital management.
The increasing intervention of the State is also reflected in the establishment of federal structures, the Joint Federal Committee and the National Association of Statutory Health Insurance Funds, which are focused on expert functions (assessment of healthcare products, procedures and structures) and act on behalf of the State, although they are officially separate from the administration. These agencies give the State more powers of monitoring, oversight, evaluation and sanction over all the stakeholders involved in health insurance (Hassenteufel, 2014).
However, this does not mean the introduction of a State-run health insurance system. Rather, the current trend has been analysed as the advent of a regulatory state, or government from a distance, which closely monitors the interactions between the various stakeholders in the health insurance system (Hassenteufel, 2014). At the same time, the “self-administration” of health insurance funds, which is the founding principle of the German health insurance system and part of the Bismarck Model, although not completely disappearing, has been seriously eroded.
References
Autret, F. 2001. "Assurance santé: le système bismarckien dans l’impasse?”. In Allemagne 2001: Regards sur une économie en mutation, 401–12. Travaux et documents du CIRAC. CIRAC, 2017. http://books.openedition.org/cirac/872.
Bas-Theron F. 2002. "Le système de santé et d'assurance-maladie en Allemagne: actions concernant la qualité des soins et la régulation des dépenses en ambulatoire". Report No. 2002 052, Inspection générale des affaires sociales (IGAS), May 2002. https://www.vie-publique.fr/rapport/25579-le-systeme-de-sante-et-dassurance-maladie-en-allemagne-actions-concer.
Berton, F. 2024. "Le droit social allemand et le système de sécurité sociale". Cabinet Berton et associés (blog), 8 December 2024. https://www.berton-associes.fr/blog/droit-social/le-droit-social-allemand/.
Boned O. 2008. "Les mutuelles en Europe: le défi de l'identité". Vie sociale 4(4): 131–148. https://shs.cairn.info/revue-vie-sociale-2008-4-page-131?lang=fr&ref=doi.
Descamps U., Kuss, J. J. and Weill G. 2001. "Le service médical de l'assurance-maladie en Allemagne". Revue médicale de l'assurance-maladie, 32(1): 51–58. https://www.ameli.fr/sites/default/files/2001-03_service-medical-allemagne_revue-medicale-assurance-maladie-2001-1_assurance-maladie.pdf.
Eichenhofer, E. 2006. "Federalism and Social Protection in Germany," Lien social et Politiques, 56: 119–125. https://doi.org/10.7202/014975ar.
EU (European Union). 2012. The management of health systems in the EU Member States – The role of local and regional authorities. Publications Office of the European Union: 2013. https://data.europa.eu/doi/10.2863/83788.
Federal Ministry of Health, Germany. 2020. The German healthcare system – Strong. Reliable. Proven. Department L8 – Public Relations, Publications: April 2020. https://www.bundesgesundheitsministerium.de/fileadmin/Dateien/5_Publikationen/Gesundheit/Broschueren/200629_BMG_Das_deutsche_Gesundheitssystem_EN.pdf.
Hassenteufel, P. 2008. "La mise en place du gouvernement à distance de l’assurance-maladie". Regards sur l'économie allemande, 89: 27–33. Bulletin économique du CIRAC. https://doi.org/10.4000/rea.2673.
— 2014. "Assurance-maladie. Une transformation structurelle engagée avant la crise". Allemagne d’aujourd’hui, 210(4): 204–217. https://doi.org/10.3917/all.210.0204.
Kaufmann O. 2016. "La protection sociale en Allemagne". CEPSE (Europa, Centre d’Étude sur la Protection Sociale en Europe). https://www.europaong.org/wp-content/uploads/2015/09/EUROPA-CEPSE-ALLEMAGNE.pdf.
Schmucker, R. 2010. "Le financement de la politique de santé de l'Allemagne: enjeux et perspectives". Note du Cerfa no 77; notes de l’IFRI, August 2020. https://www.ifri.org/fr/publications/notes-de-lifri/notes-cerfa/financement-de-politique-de-sante-de-lallemagne-enjeux.
Sénat (Le). 1995. "La protection sociale". Service des affaires européennes, 4 October 2022. https://www.senat.fr/lc/lc10/lc10_mono.html.
— 1999. "La couverture maladie universelle". Étude de législation comparée no 56, May 1999. https://www.senat.fr/lc/lc56/lc56.html.
Vanlerenberghe J. M. and Daudigny, Y. 2016. "Organisation et financement de la médecine de ville en Allemagne". Rapport d’information n° 867 (2015–2016). Le Sénat, September 2016. https://www.senat.fr/rap/r15-867/r15-867.html.
Vasselle A. and Cazeau B. 2006. "Préserver la compétitivité du "site Allemagne" : les mutations de la protection sociale outre Rhin". Rapport d’information n° 43 (2005–2006). Mission d'évaluation et de contrôle de la sécurité sociale et de la commission des affaires sociales, Le Sénat, June 2006. http://www.senat.fr/rap/r05-439/r05-439.html.
9. Ghana
9.1 Background
From Ghana's economic stagnation and structural adjustment policies led to the introduction of health service user the 1970s onwards, fees, with the “cash and carry” system introducing full payment for treatment by the user. This measure revoked the general tax-funded free access to certain services in public hospitals, health centres and pharmacies introduced by Kwame Nkrumah's government during the post-colonial period. Access to healthcare was thus greatly reduced, especially for the poorest households, for whom exemption policies introduced proved to be ineffective. It was against this backdrop that the first mutuals were set up in Ghana, including the Nkoranza CBHI programme initiated by the Catholic diocese of the Sunyani district, close to the Sainte Thérèse hospital. This CBHI scheme was gradually extended to cover almost 30 per cent of the district's population in 2000 (Blanchet and Acheampong, 2013).
Nkoranza's experience inspired other faith-based actors, healthcare providers, geographical and professional groups and the Ministry of Health to promote other mutual societies, with technical and financial support from external partners, including the Danish International Development Agency (DANIDA) and USAID's Partners for Health Reformplus (PHRplus) project. Similarly, during the 1990s, the Ghana Medical Association, the ILO, the WHO, the European Union and trade union organizations called on the government to create health cover to offset the negative impact of the cash and carry system (Alenda-Demoutiez et al., 2019).
In 2001, the country had 47 mutuals, 43 of which were created between 1999 and 2000 (Alenda-Demoutiez et al., 2019). In 2002, there were more than 140 mutuals; in 2003, there were 258 grouped together in a national mutual network, the Network of Mutual Health Organizations of Ghana (GNEMHO) (Atim, 2015). However, these mutuals covered only around 1 to 2 per cent of the population, with limited benefits, confined to local healthcare providers under contract with the mutuals and financed by registration fees and members' contributions. Most of these community health insurance schemes also lacked appropriate expertise in insurance-specific technical and financial management, community mobilization and participation, and monitoring and evaluation (Otoo, 2016).
Following the presidential elections in 2000, during which the electoral campaign put health insurance at the top of the political agenda, the new government set itself the objective of promoting the experience of mutuals. The aim was multiple: to abolish direct payments but without reintroducing a policy of free healthcare; to tackle the problem of underfunding of health facilities; and to finance health in a sustainable way so as to ensure accessible, affordable and quality healthcare for all, especially the most vulnerable. In this context, and as part of Ghana's Poverty Reduction Strategy (2003), the government developed the National Health Insurance Scheme (NHIS). The National Health Insurance Act was passed in 2003, 78 followed by the National Health Insurance Regulations at the end of 2004. 79 This strengthened and uniform health insurance scheme was designed as an improvement on the mutual society systems developed since the 1990s. The National Health Insurance Act required all districts to set up a mutual health organization (MHO), the organizational structure and financial management of which was standardized, defining a set of minimum interventions that each MHO must cover. In broad terms:
-
Act 650 moved Ghana from a fragmented system with poor geographical and demographic coverage to a national system, covering all districts and aiming to integrate CBHI systems into a regulated yet still decentralized national system. The law established a system of district mutual health insurance (DMHI), based on the experience of existing mutual health organizations, and defined a set of minimum interventions that each MHO had to cover. The law also standardized procedures, particularly for registering families, and set contribution levels. It was also based on the process of decentralizing governance that was under way at the time (Baltussen et al., 2006; Blanchet and Acheampong, 2013). The districts of Ghana thus became the main base for the planned implementation and roll-out of the NHIS.
With the enactment of the law, three types of health insurance schemes came into being: district mutual health insurance schemes (DMHI), private mutual health insurance schemes (PMHIS), and private commercial health insurance schemes (PCHIS). The law makes it compulsory for all residents of Ghana to enrol on one of these three approved insurance schemes.
-
The 2003 Act also established the National Health Insurance Authority (NHIA), which is overseen by the National Health Insurance Council and responsible for registering, licensing, regulating, accrediting and monitoring healthcare providers operating within the health insurance system.
-
The National Health Insurance Fund was set up, responsible for granting subsidies to approved district health insurance mutuals. A tax levy was introduced for health insurance, with the NHIS designed as a semi-contributory scheme, financed partly by contributions from insured persons and, to a large extent, by national taxes.
Act 650, adopted in August 2003, was implemented from 2004 with the adoption of more detailed legal instruments. The system became operational in 83 of the 138 districts by the end of 2005 and most of the 258 MHOs existing in 2003 were integrated into the NHIS (Otoo, 2016). The NHIS reached a total of 2.9 million beneficiaries, or 14 per cent of the population, by late 2005 and 38 per cent of the population in 2006. However, only 19 per cent of workers in the informal sector had received identification cards and were able to access the services offered, and coverage of the poor was low, mainly because of difficulties in identifying and including them (Berkhout and Oostingh, 2008). In 2008, the government supplemented the scheme by introducing free care for pregnant women and children under five years of age as part of the health insurance system (Oxfam, 2012).
The 2003 Act was replaced by a new law 80 in 2012, which has since governed Ghana's health insurance programmes (USAID, 2016). Act 852 of 2012 aims to strengthen the NHIS by removing administrative bottlenecks, introducing more transparency, reducing opportunities for corruption and manipulation of the system and ensuring more effective governance of the schemes (nhis.gov.gh). It also reiterates the obligation for every Ghanaian to enrol on one of the three insurance schemes of the National Health Insurance Scheme (Ridde et al., 2021).
9.2 The national social health protection system
Governance
The NHIS is overseen by the National Health Insurance Council, established by Act 650 as the general body responsible for overseeing the implementation of health insurance schemes in the country.
Technical and financial management is carried out by the NHIA, a public-sector body created by the National Health Insurance Act in 2003 and operating under the supervision of the Ministry of Health. The NHIA is governed by a governing body composed of representatives from a wide range of institutions, including the Ministry of Health, the Ministry of Finance and Economic Planning (MoFEP), the Ministry of Gender, Children and Social Protection (MoGCSP), the NHIA itself, the Ghana Health Service (GHS), the National Insurance Commission (NIC), the Social Security and National Insurance Trust (SSNIT), the Medical and Dental Council (MDC), trade unions and other persons appointed by the President (nhis.gov.gh). The composition of the governing body thus reflects an attempt at a multisectoral approach. The NHIA's organization chart then consists of its central directorate, followed by 16 regional offices in the country's 16 political regions, 166 district offices and five registration centres. These offices stem from the DMHI, which were integrated into the NHIA by the 2012 Act. They are supervised by and report to the regional offices, which in turn report to the national headquarters via the Membership and Regional Operations Directorate (MRO). Registration of members on the scheme and renewal of membership is carried out at the district offices (nhis.gov.gh). The insurance employed around 3,600 staff nationwide in 2019 (Antwi, 2019).
The aim of the NHIA is to ensure access to basic healthcare services to all residents in Ghana as well as those visiting the country, through the NHIS. The NHIA implements the national health insurance policy and to achieve this it may:
-
implement, operate and manage the NHIS;
-
determine, in consultation with the Minister of Health, contributions that should be made by members of the NHIS, promote equity in healthcare coverage, and ensure access by the poor to healthcare services;
-
register members of the NHIS, including those exempt from contributions, and issue policyholder cards;
-
grant credentials to healthcare providers and facilities that provide healthcare services to members of the NHIS;
-
manage the National Health Insurance Fund;
-
receive, process and pay claims from healthcare providers;
-
receive, through decentralized offices, and process complaints from NHIS members and healthcare providers;
-
make proposals to the Minister of Health for the formulation of health insurance policies and programmes that promote the sustainability of the NHIS;
-
Undertake, where possible in collaboration with other organizations, initiatives to raise public awareness of health insurance;
-
develop guidelines, processes and manuals for the effective implementation and management of the NHIS (nhis.gov.gh).
The NHIA is also mandated to regulate private health insurance plans (PHIS), which are divided into two categories by Act 852 of 2012:
-
the Private Mutual Health Insurance Scheme (PMHIS); and
-
the Private and Commercial Health Insurance Scheme (PCHIS).
NHIA functions include:
-
granting licences to insurers and insurance intermediaries carrying out health insurance activities in Ghana;
-
developing and disseminating guidelines for the operation of private health insurance schemes in consultation with the relevant bodies, and supervising transactions between insurers, intermediaries and reinsurers;
-
protecting the interests of members of private health insurance schemes and providing a service to which members of the public can direct their complaints for resolution; and
-
guaranteeing the efficiency and quality of services under the national and private health insurance schemes (nhis.gov.gh).
Through the 2012 Act, Ghana brought all schemes (government, other public initiatives, private-sector insurance, community health schemes) under the umbrella of a single system. As noted above, the Act fundamentally reformed the system established by the 2003 Act by integrating the DMHI (most of which had themselves evolved from CBHI) into the unified NHIS scheme. Prior to this merger, 145 DMHI (one per district) operated as independent schemes with their own governance and management structures and collected contributions directly. These district mutuals faced many governance challenges, including non-compliance with guidelines and corruption in the operations of these schemes (Alhassan et al., 2016). Their supervision by the NHIA was complicated, and this fragmentation weakened risk pooling and increased administrative costs (Otoo, 2016; Alenda-Demoutiez et al., 2019).
Population coverage
The NHIS is aimed at the entire population, through three main groups of insured persons (see below).
-
Employees in the formal sector and the self-employed who contribute to the Social Security and National Insurance Trust (SSNIT), with 2.5 per cent of the funds paid into the NHIS and no increase in employers' and workers' social security contributions.
-
Workers in the informal sector, who are the only group required to pay a direct contribution to the NHIS.
-
Insured persons exempt from contributions. This group includes:
-
children (under the age of 18)
-
pregnant women (for antenatal, delivery and postnatal healthcare services)
-
persons classified as in the poorest category by the Minister for Social Protection
-
categories of people living with a disability, as determined by the Minister for Social Protection
-
persons with a mental disorder
-
SSNIT pensioners
-
persons above 70 years of age (the elderly)
-
other categories prescribed by the Ministry of Social Protection (nhis.gov.gh)
Breakdown of membership categories (2016)
|
Employees in the formal sector (SSNIT) |
Army, police and other security services |
Informal sector |
SSNIT pensioners |
Children under the age of 18 |
Persons above 70 years of age |
Poorest people |
Pregnant women |
|
4.7% |
0.2% |
28.2% |
0.1% |
41.3% |
4.3% |
14.1% |
7.1% |
Source: NHIS, 2022
Looking at NHIA data in 2016, the contribution-exempt group represents 66.9 per cent of NHIS members, which is in line with the scheme's objective of providing financial access to health services for poor and vulnerable people (NHIS, 2022).
The 2003 and 2012 Acts introduced compulsory membership. However, this is not accompanied by coercive measures or penalties for failure to register, nor are there any mechanisms to ensure automatic registration of residents. In practice, therefore, the scheme is voluntary (Antwi, 2019). This partly explains why, despite an initial rapid increase in membership and while the NHIS is offering a generous benefits package, NHIS membership has stagnated for several years at around 40 per cent, and why the majority of members fall into government-subsidized population groups (Dalal et al., 2019). Ghana is still a long way from achieving universal SHP coverage. In addition to the difficulty of enforcing compulsory membership, various studies have highlighted several reasons for this stagnation.
-
Although the annual contributions of employees in the informal sector (which accounts for around 75 per cent of the total workforce) are subsidized, many of these workers cannot afford to pay them (Averill, 2013). Contributions vary for adults (aged 18 to 70) between 7.2 and 48 Ghanaian cedis (US$2 to 10), depending on income and ability to pay (nhis.gov.gh). However, in practice, many DMHI ask for a lump-sum premium because of the difficulty of assessing household income levels. In addition, many are illiterate and do not understand the steps to be taken or know that the card has to be renewed every year (Oxfam, 2012).
-
In addition, the annual membership renewal process at NHIA district offices is time-consuming for both members and NHIA administrative staff, and discourages many members from renewing their membership, resulting in the cancellation of their cover.
-
Deficiencies in technical management have led to dissatisfaction among beneficiaries, particularly with regard to the poor management of healthcare requests and the behaviour of health workers, following delays in the reimbursement of healthcare services (Ridde et al., 2021).
-
In addition, the system faces difficulties in identifying and including poor people in the scheme (almost a third of Ghana's population lives below the poverty line) (Berkhout and Oostingh, 2008).
Overall, almost 60 per cent of the population does not have access to NHIS health cover and continues to pay directly for its healthcare. Until the late 2000s, Ghana was often cited as a model of success, like Rwanda, with population coverage rates of up to 70 per cent. However, various studies and observations by NGOs and civil society have revealed huge discrepancies between "real" and official coverage rates. For example, far from reaching the rates broadcast in the media, the government has had to reduce them to 35 per cent, a level that has only increased slightly since 2014 (Africa 21, 2013).
Healthcare package
The NHIS offers generous, nationally standardized cover. The insurance covers the full cost of 95 per cent of illnesses and health problems, with no co-payments. This cover includes all emergencies, such as road traffic accidents, industrial accidents, paediatric emergencies, and so on, as well as consultations, dental care, tests, X-rays, surgical costs, hospitalization costs and medicines, in public and private health facilities approved by the NHIA, at all levels of the health pyramid. Coverage is linked to compliance with a referral scheme, whereby beneficiaries must first go to a primary healthcare facility and then, if necessary, be referred to secondary and tertiary level facilities. Exclusions include dental, orthopaedic and ophthalmic prostheses, cosmetic surgery, electrocardiograms, dialysis, cancer (other than cervical and breast cancer), as well as services provided by government programmes covering antiretroviral treatment for HIV/AIDS, vaccination and family planning. There is no limit to the amount of medical bills paid by the NHIS, provided that the treatment complies with the provisions of the benefits package. The services covered by the insurance are billed by the care providers to the NHIA. The NHIA has four centres for processing provider claims for reimbursement; reimbursement procedures are lengthy and payment arrears are high.
The range of public and private providers is vast, including community-based health services, maternity units, health centres, district hospitals, hospitals, outpatient clinics and polyclinics, as well as pharmacies and diagnostic centres (nhis.gov.gh). To increase the availability of health services in underserved areas, the government is relying on public-private partnerships. This includes an agreement with the Christian Health Association of Ghana (CHAG), which has developed a network of 183 faith-based healthcare facilities; through this partnership, the government supports the network's facilities with salaries, equipment and medical supplies, and the CHAG provides health services to disadvantaged communities in remote areas across the country (Kuwonu, 2017).
Financing
The NHIS is financed at the national level from a single fund, the National Health Insurance Fund, which groups together all sources of funding and enables resources and risks to be pooled. NHIS resources come from:
-
the National Health Insurance Levy (NHIL), which is an earmarked portion of 2.5 per cent of value added tax (72 per cent of NHIS revenue);
-
statutory transfers of 2.5 per cent of workers' social security contributions (20 per cent of NHIS income);
-
contributions paid by members of non-exempt groups (3 to 5 per cent of NHIS revenues); and
-
other sources (1 per cent).
Only beneficiaries aged between 18 and 69 in the informal sector are required to pay an annual premium in addition to the enrolment fee. Initially, this contribution was theoretically income-adjusted, but in practice a lump-sum premium was charged by many DMHI because of the difficulty of assessing household income levels. Currently, the annual NHIS premium ranges from 7.20 Ghanaian cedis (US$1.60) to 48.00 Ghanaian cedis (US$10.60) per person, depending on the region of residence (nhis.gov.gh) (Salari et al., 2019). Children and the elderly are exempt from paying the annual membership fee. In addition to the membership fee, NHIS members, with the exception of pregnant women and the poorest people, must pay a registration fee and an annual renewal fee for their policyholder card (nhis.gov.ghm). Since 2019, this renewal fee has been harmonized at the national level and amounts to 30 Ghanaian cedis (US$5.5 in 2019) (Kipo-Sunyehzi et al., 2019).
9.3 Experience of delegated monangemetn at the district level from 2004 to 2012
The management system set up under the 2003 Act
As detailed above, Ghana's health insurance system, introduced with Act 650 of 2003, was based on the mutuals and other CBHI mechanisms developed throughout the country since the 1990s. The government's strategy for extending health cover to all Ghanaians, particularly those in the informal sector and rural areas, was based on the following principles:
-
The definition at the national level of a reference healthcare package (outpatient and inpatient).
-
The creation of DMHI affiliated to the national system, for which they received financial support to set them up.
-
The option given to existing mutuals to join the NHIS and become district mutuals, or to remain independent on condition that they do not compete with the national system by offering more attractive benefits than the NHIS. As detailed below, most of the existing mutuals chose to join the NHIS and reorganize as DMHI when the Act came into force.
This strategy was a model for a public health insurance system based on, and integrating, private actors in order to benefit from their expertise, particularly in terms of purchasing healthcare services, training local expertise and creating accountability and transparency frameworks for healthcare structures. This alliance with mutuals is considered to be one of the factors that has helped the population's coverage rate rise from 1 per cent in the 1990s to almost 40 per cent today (Lambert and Del Hierro, 2017).
Delegation of management to district mutuals
DMHI are the most common form of insurance mechanism set up at district level as part of the national scheme launched in 2004. These mutuals were set up as companies limited by guarantee, registered in the National General Register. As such, they presented themselves as independent economic and legal entities. Each DMHI also had to apply for a licence from the NHIA before it could start providing services to its members. The DMHI schemes thus retained a certain degree of autonomy in their management and governance structure, while benefiting from technical support from the NHIA and public funding.
Act 650 provided for the creation of a DMHI in each district, municipality or metropolitan area. By the end of 2006, 139 DMHI were in place and providing services to their members (Grüb, 2007). With the creation of new districts, Ghana had 145 DMHI in 2012, operating under the regulation of the NHIA (Antwi, 2019).
Each district mutual was administered by:
-
a general assembly
-
the governing body
-
a management team for the scheme
-
community health insurance committees across the district, whose elected delegates represented the insurance members at the general assembly
The general assembly and governing body were responsible for directing the scheme's policies and appointing employees. In addition to the members of the mutual, the governing body also included representatives of religious communities, traditional authorities, women's groups, health services and the district administration.
Day-to-day management was carried out by the management team, which consisted of a scheme manager, a training systems manager, a claims manager, a public relations officer and an accountant (Grüb, 2007).
DMHI acted as delegated management structures and carried out a large proportion of the health insurance functions within the NHIS.
-
Each district health mutual was responsible for deploying and administering public health insurance within its area of intervention.
-
It was responsible for registering and renewing members and identifying the poorest people based on criteria laid down by the NHIS (not having a job or visible income resources; having no fixed abode; not living with someone who has a job and a fixed abode; having no significant support from anyone).
-
DMHI collected all contributions from contributing beneficiaries (workers in the informal economy), and received an annual premium from the National Health Insurance Fund for each beneficiary exempt from contributions. This annual amount per individual was initially 8 Ghanian cedis, then gradually increased to 14 cedis.
-
In addition to this capitation fee, DMHI received subsidies to balance their budgets. These represented 80 to 90 per cent of their resources, making DMHI highly dependent on NHIA subsidies.
-
The healthcare package was determined at the national level. In addition to these basic guarantees, each DMHI could choose to provide additional services.
-
Lastly, the district mutuals signed agreements with healthcare providers and acted as purchasers (Gajate-Garrido and Owusua, 2013), with the result that cover for insured persons was limited to healthcare providers in the district.
Distribution of functions between the NHIA and DMHI
|
Functions |
Distribution |
|
|
NHIA |
DMHI |
|
|
Definition of the healthcare package |
X |
|
|
Agreements |
X |
|
|
Education and promotion |
X |
X |
|
Enrolment, membership and renewal |
X |
|
|
Contribution collection |
X |
|
|
Resource mobilization |
X |
|
|
Pooling of risks covered |
X |
|
|
Payment of benefits |
X |
|
|
Healthcare services |
||
|
Follow-up and steering |
X |
|
As detailed below, the insurance scheme put in place by the 2003 Act has faced significant challenges in terms of governance, accountability and compliance with national guidelines by DMHI. The revision of the Act in 2012 (Act 852) reformed this system by integrating all DMHI into a unified NHIS governed directly by the NHIA, replacing district mutuals with NHIA offices.
Private mutuals
Two major groups of mutuals existed when the 2003 Act was passed:
-
Mutuals set up by a clearly defined local community or group of people, whether inhabitants of the same village or traditional area, migrants from the same region of origin, women and children only, members of a producers' cooperative union or members of credit cooperatives.
-
Mutuals organized on a wider geographical basis, in other words, the target hospital or district area.
The services provided by the mutuals in these two groups were generally limited to major risks, in other words, covering major and catastrophic hospital expenses. On the other hand, outpatient healthcare was not covered at all, or only to a very limited extent.
A provision of Act 650, reiterated in Act 852 of 2012, allows these mutuals to continue to operate as autonomous health mutuals subject to approval by the National Health Insurance Council and the obligation to provide the minimum benefits in the NHIS healthcare package. In return, these mutuals also receive a subsidy from the government through the National Health Insurance Fund. However, faced with the requirement to provide the minimum NHIS benefits, many community mutuals have stopped providing services and have taken on the status of community health insurance committees relaying information on the DMHI of their district in their area of intervention and representing the communities in this area to the district mutual. Most of the mutuals in the second group chose to join the NHIS and become DMHI (Grüb, 2007).
The same provision also exists for private commercial insurers, for which the law also provides for licensing, regulation and supervision by the NHIA. These private insurers must provide the minimum benefits in the NHIS healthcare package, but are not eligible for state subsidies (Antwi, 2019).
9.4 Impact and lessons learned
The use of the experience acquired by mutuals since the 1990s during the implementation of the NHIS is generally considered, through the various studies and other documentation on the experience in Ghana, to be one of the factors that have enabled a rapid increase in take-up rates. Enrolment in health insurance has also had a positive effect on the use of modern health services and a protective effect on the level of personal expenditure on outpatient care. However, Ghana is still a long way from the SHP goal of universal coverage, with enrolment stagnating at around 40 per cent (Dalal et al., 2019).
After several years of operation, a number of challenges have been documented:
-
The majority of DMHI were faced with a lack of human resources in terms of numbers, appropriate training and motivation, compounded by low salaries and frequent delays in payment.
-
Inadequate logistics and infrastructure: limited number of computers, vehicles and appropriate premises, as well as internet and electricity outages.
-
Poor governance at certain DMHI, failure to comply with national directives and numerous corrupt practices in the management of claims for reimbursement of healthcare costs.
-
A lack of cooperation from healthcare providers, particularly with regard to compliance with NHIS drug lists and tariffs, overbilling, fictitious, erroneous or overcharged services and delays in submitting claims for reimbursement.
-
Insufficient implementation of measures to control fraud, adverse selection and prevent benefit cost slippage.
-
High level of administrative costs, the lack of local resources (contributions from insured persons in the informal sector) linked to poverty in certain regions, and the lack of adequate funding.
-
Low awareness of the scheme and the target groups' lack of interest and confidence in the NHIS, partly due to a lack of communication and awareness of the insurance scheme (Gajate-Garrido and Owusua, 2013; Antwi, 2019).
Overall, the fragmentation of the insurance scheme with a large number of district mutuals has reduced risk pooling and led to significant administrative costs. In addition, supervision of all the district mutuals proved complicated for the NHIA (Amporfu et al., 2022). In addition, coverage was limited to the DMHI area of intervention (district, municipality or metropolitan area), with no pooling at regional or national levels, and no agreement between DMHI schemes to cover an insured person outside his or her district.
One recommended response to these challenges was to professionalize the insurance system, with greater involvement of the NHIA in technical and financial management. This approach was adopted when Act 650 was revised and Act 852 adopted in 2012, which integrated all DMHI into a unified system governed directly by the NHIA. The district mutuals were replaced by NHIA offices and the system became centralized, with the NHIA becoming the main agency for mobilizing resources, pooling risks and purchasing healthcare services.
It is interesting to note, however, that the legal framework established by the 2003 Act, and then the 2012 Act, allows for the existence of autonomous mutuals, which can operate subject to approval by the NHIA and on the condition that they do not compete with the NHIS. These mutuals must therefore offer at least the NHIS package of services; in return, they receive state subsidies for groups exempt from contributions. The current existence and functioning of these mutuals appears to be poorly documented at present, yet they could be an interesting way of extending the NHIS to the entire population. These mutuals, which stem from social networks, professional or corporate organizations, could potentially have a greater wealth of trust than the public insurance system; they could also benefit from the technical mechanisms (data system, computerization of procedures and mobile payment of contributions developed by the NHIA since 2017) and subsidies from the latter (Dalal et al., 2019). In the light of the experience of Ghana and the other African and European countries examined in the various case studies, one pitfall to be avoided is the proliferation of mutuals, which can be achieved by promoting large-scale, professionalized and transparent systems working within a clear framework of partnership with the NHIA.
References
Africa 21. 2013. "Gouvernance du financement de la santé mondiale : enjeux et perspectives africain". Africa 21, Note 2, February 2013 https://knowledge.uclga.org/IMG/pdf/gouvernancedufinancementdelasantemondialeenjeuxetperspectivesafricains.pdf.
Alenda-Demoutiez J., Antwi A., Mendo E. and Ba Z. S. 2019. "Health Protection in Ghana and Senegal: What is the ILO’s Role?" In International Development Policy | Revue internationale de politique de développement 11: 111–131, Part 2, 1 June 2019. https://journals.openedition.org/poldev/3040.
Alhassan R. K., Nketiah-Amponsah E. and Kojo Arhinful D. 2016. "A Review of the National Health Insurance Scheme in Ghana: What Are the Sustainability Threats and Prospects?" In PloS One. 10 November 2016. 11(11): e0165151. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0165151.
Antwi A. 2019. "The pathway of achieving the universal health coverage in Ghana: the role of social determinants of health and "health in all policies"". Economics and Finance. University of Lille, 2019. English. NNT: 2019LILUA002 tel-03633484f. https://tel.archives-ouvertes.fr/tel-03633484/document.
Amporfu E., Agyei-Baffour P., Edusei A., Novignon J. and Arthura E. 2022. "Strategic Health Purchasing Progress Mapping: A Spotlight on Ghana's National Health Insurance Scheme". In Health Systems & Reform 8(2): Making Progress on Strategic Health Purchasing in Africa, 13 June 2022. https://doi.org/10.1080/23288604.2022.2058337.
Atim C. 2015. "Le financement de la couverture santé universelle : leçons tirées de l’expérience du ‘NHIS’ (la CNAM) au Ghana". Haiti, April 2015.
Averill C. 2013. "Universal health coverage: Why health insurance schemes are leaving the poor behind". Oxfam Briefing Paper No. 176, Oxfam International, 9 October 2013. https://www-cdn.oxfam.org/s3fs-public/file_attachments/bp176-universal-health-coverage-091013-en__3.pdf.
Baltussen R., Bruce E., Rhodes G., Narh-Bana S. A., and Agyepong I. 2006. "Management of mutual health organizations in Ghana". In Tropical Medicine & International Health 11(5): 654–659. https://onlinelibrary.wiley.com/doi/10.1111/j.1365-3156.2006.01621.x.
Berkhout E. and Oostingh H. 2008. "Health insurance in low-income countries: Where is the evidence that it works?" Oxfam Briefing Paper No. 112. https://www-cdn.oxfam.org/s3fs-public/file_attachments/bp112_health_insurance_0805_4.pdf.
Blanchet N. J. and Acheampong O. B. 2013. "Building on Community-based Health Insurance to Expand National Coverage: The Case of Ghana". USAID, 30 December, 2013. https://www.hfgproject.org/building-on-community-based-health-insurance-to-expand-national-coverage-the-case-of-ghana/.
Dalal A., Morgan L. and Nanda S. 2019. "Case Brief: NHIA, Ghana". Impact Insurance, ILO, December 2019. https://researchrepository.ilo.org/esploro/outputs/encyclopediaEntry/Case-brief-NHIA-Ghana/995218605302676.
Gajate-Garrido G. and Owusua R. 2013. "The National Health Insurance Scheme in Ghana Implementation Challenges and Proposed Solutions". IFPRI Discussion Paper 01309, IFPRI, December 2013.
Grüb A. Unpublished. "Ghana – Social Security Schemes for Health”. Study on linkages between statutory social security systems and community-based social protection mechanisms. ILO, ISSA and AIM, Accra, March 2007.
Kipo-Sunyehzi D., Dramani D., Ayanore M.A., Kweku Dzidzonu D. and Ayalsuma Y. 2019. "Ghana's Journey towards Universal Health Coverage: The Role of the National Health Insurance Scheme". In European Journal of Investigation in Health, Psychology and Education 10(1): 94–109. https://doi.org/10.3390/ejihpe10010009.
Kuwonu F. 2017. "Public health schemes: Getting it right". From Africa Renewal: December 2016–March 2017. United Nations digital magazine Africa Renewal. https://www.un.org/africarenewal/magazine/december-2016-march-2017/public-health-schemes-getting-it-right.
Lambert A. and Del Hierro E. 2017. "Comment étendre la couverture de l’assurance santé en Afrique ?" ID4D media for sustainable development, 26 January 2017. https://ideas4development.org/couverture-maladie-afrique/.
NHIS (National Health Insurance Scheme). 2017. National Health Insurance Authority 2016 Annual Report. Ghana Health Service. https://www.moh.gov.gh/wp-content/uploads/2017/09/2016-Annual-Report.pdf.
Otoo N. 2016. “Financial Protection and Improved Access to Health Care: Peer-to-Peer Learning Workshop – Finding Solutions to Common Challenges". Accra, 15 February 2016.
Oxfam. 2012. "Au Ghana, encore des efforts à faire pour l'assurance-maladie". Oxfam France, 10 February 2012. https://www.oxfamfrance.org/financement-du-developpement/au-ghana-encore-des-efforts-a-faire-pour-lassurance-maladie/.
Ridde V., Antwi A., Boidin B., Chemouni B., Hane F. and Touré L. 2021. "Les défis des mutuelles communautaires en Afrique de l’Ouest". In Vers une couverture sanitaire universelle en 2030? Editions science et bien commun: 2021. https://scienceetbiencommun.pressbooks.pub/cus/chapter/implications-pour-la-recherche-et-pour-les-politiques-de-sante/.
Salari P., Akweongo P., Aikins M., and Tediosi F. 2019. "Determinants of health insurance enrolment in Ghana: evidence from three national household surveys". In Health Policy and Planning 34(8): 582–594. https://doi.org/10.1093/heapol/czz079.
USAID (United States Agency for International Development). 2016. "Health insurance profile: Ghana," African Strategies for Health, USAID. February 2016. https://pdf.usaid.gov/pdf_docs/PA00MBBH.pdf.
Other documents consulted:
NHIS (National Health Insurance Scheme). n.d. NHIS website https://www.nhis.gov.gh/ [consulted on 15 October 2023].
10. Japan
10.1 Overall System Overview and Background of Health Insurance in Japan
Japan achieved universal population coverage in 1961. 3 years earlier, the Community Health Insurance Law had made enrolment of all those who were not previously covered mandatory, and had mandated municipalities to establish the National Health Insurance (NHI) plans. Thanks to this social health protection system, all those officially residing in Japan are now covered by one of the statutory health insurance schemes
There are four types of compulsory social health insurances in Japan:
-
The Employees’ Health Insurance, EHI (Hiyosha Kenko Hoken), an occupation-based scheme;
-
The National Health Insurance, NHI (Kokumin Kenko Hoken), which is region-based, for those not employed, self-employed, and retirees;
-
The Health Insurance for Advanced Elderly scheme that covers all adults who are 75 years and older (Koki Koreisya);
-
And an age-based long-term care insurance scheme (Kaigo Hoken)
(Ikegami, Naoki; Phe Goursat, Marielle 2021) .
The EHI gathers 4 different types of schemes: the Societies (or Union)-managed Health Insurance (Kumiai Kansho Kenko Hoken); the Japan Health Insurance Association-managed Health Insurance, JHIA-mHI (Zenkoku Kenko Hoken Kyokai Kansho Kenko Hoken); the Mutual Aid Association Health Insurance, MAAHI (Kyosai Kumiai Kenko Hoken); and Seamen’s Insurance SI (Sen-in Hoken).
Emergence of Health Insurance Societies and Mutual Aid Associations
Prior to the introduction of the National Health Insurance Act No. 192 in 1958, various social health protection schemes had already been implemented in Japan. The initial Health Insurance Act was introduced in 1922. It provided that companies regularly employing a certain minimum number of employees had to set up health insurance societies, which were established as public corporations. For those who remained uncovered, the Act provided the creation of Japan’s first Employee’s Health Insurance (EHI) scheme, implemented in 1927 and targeting at first manual laborers but expanding soon to formal employees.
In parallel, mutual aid associations were operating in Japan, including the national public servant mutual aid association. Others came later such as the Seamen's mutual aid association in Seamen's Insurance Act of 1940. The Ministry of Health, Labour, Welfare Mutual Aid Association of Japan defines mutual aid associations as “A social security system designed to help cooperative members help each other and improve the stability and welfare of each other's lives.”
Several reasons for the emergence of health insurance societies and mutual aid associations can be cited: An increase in work injuries and the deterioration of workers’ health due to changes in the industrial structure; increasing wages of employees; the development of medical services and utilization thereof, which increased medical out-of-pocket expenses; the expansion of labour movements; employers’ interest in the employee’s welfare; and lastly national alignment on international efforts towards extension of social protection including the first International Labour Conference in 1919
Introduction of the National Health Insurance
However these schemes did not manage to achieve full population coverage; for example, agricultural industries and small business owners were not covered by any scheme. Despite limited coverage, however, the fact that certain categories of population could be insured by health insurance societies and mutual aid associations prior to 1958 certainly eased the introduction of the National Health Insurance (NHI) then. When introducing the NHI, a survey’s result showed that over 90% of those who had already joined in any mutual aid association wanted to be kept insured
In 1958, the National Health Insurance Law was enacted and started providing coverage to those who were out of any health insurance society or mutual aid associations. It provided geographical, rather than employment-based insurance. Revenues of the National Health Insurance came from a mix of central taxation, local taxation, and social contributions.
Current Health Insurance Societies and Mutual Aid Association Overview
National Health Insurance and Employees’ Health Insurance complement each other and function as different insurers under different laws.
Currently, all Japanese people should join one of the main health insurance schemes cited above. The table below gives further information on these schemes:
|
Name of the scheme |
Target groups |
Managing entities |
Number of people covered (thousand) |
|
Employees’ Health Insurance |
Those who are working at private companies that have five or more regular employees; and their dependents under certain conditions. |
Japan Health Insurance Association and Health Insurance Societies (1,444) - Societies are organized by single companies (Single Health Insurance Societies) or jointly by several business owners within the same industry (General Health Insurance Societies). |
69,298 |
|
Mutual Aid Association’s Health Insurance |
National and Local Public Employees, private school teachers and staff members |
Mutual aid associations (85), including: - Federation of National Public Service Personnel Mutual Aid Associations (20 mutual aid associations) - Mutual Aid Association of Prefectural Government Personnel (64 mutual aid associations), - Mutual Aid Association of Private School Personnel (1 mutual aid association). |
8,424 |
|
Seamen’s insurance |
Seamen |
Government |
118 |
|
Health Insurance for Advanced Elderly |
Those who are over 75 years old |
Associations of Medical Care Services for Older Senior Citizens (47 associations in all prefectures) |
18,032 |
|
Citizens’ Health Insurance (Kokumin kenko hoken) |
The self-employed, unemployed, their dependents and retirees under 75 years of age. Any person officially residing in Japan is eligible until they enrol in another health insurance scheme. |
Municipalities and Citizens’ Health Insurance associations |
29,324 |
Source:
Participants in the mutual aid association can receive the services by paying a contribution. Contribution rate is revised every year, on the basis of the entire mutual aid’s expenditure to ensure financial balance on a yearly basis
Coverage of mutual aid associations is broader than the NHI coverage, as dependents are also covered. Healthcare benefit package is harmonized for all schemes; however health insurance societies and mutual aid associations include additional contingencies. For example, an allowance for the sick and wounded is included, while it is provided only optionally in the national health insurance.
10.2 Main characteristics of delegation
Legal Basis of the delegation
The Constitution of Japan includes the right to health and affirms the State’s responsibility in fulfilling this right
Laws regulating health insurance societies and mutual aid associations differ. The National Public Officers Mutual Aid Association Act (for civil servants) was established in 1958. According to this Act, as long as a person is working at the national government, they are eligible to participating in the National Public Officers Mutual Aid Association. For those who belong to local government, the Local Public Care Service Mutual Aid Association Act (Act No. 152 of 1962) prevails. The Promotion and Mutual Aid Corporation for Private Schools of Japan Act (Act 48 of 1997) covers specific private schools employees. The Health Insurance Law (1922) applies for those who are in health insurance societies for private companies, comprising of 1,444 health insurance societies.
Characteristic of Delegation
Since all health insurance societies and mutual aid associations including Mutual Aid Association for national public servants have an official autonomous status under the law, and they can freely define their contribution rates and modalities. Their benefit package is approximatively the same as other national social health protection schemes but the mutual aid associations typically apply higher benefits’ amounts.
Regarding the providers’ network, members can freely go to any hospitals or clinics which are approved by Ministry of Health, Labour, and Welfare. Fee-for-service payment is applied for purchasing. There are only a few directly owned hospitals by mutual aid associations.
Each mutual aid association yearly reviews its financial situation to determine the next year’s contribution rate. They have autonomy in risk pooling and revenue collection. For health insurance societies, the State provides fixed amount subsidies for expenditure related to benefits provision of Health Insurance Societies. It also covers the total amount of admin costs for National and Related Public Service Mutual Aid Associations, and parts of administrative costs of Private school teachers and employees mutual aid association. Municipalities cover the total amount of admin costs for Local Government Employees' Mutual Aid Association. In addition, the Japanese government, as employer of civil servants, transfers funds equal to 50% of the total contribution of civil servants to Mutual Aid Association for national public officers.
Delegated functions
Concretely, the various functions of health insurance are ensured as follows:
|
Function |
Details of delegated function |
|
Coverage |
|
|
Population coverage |
Mutual aid associations cover those who are working as national civil servants, local public employees, private school teachers and staff members - from the first day of working. Health insurance societies cover private company workers in companies with over 5 employees. Companies that do not establish their own health insurance societies must join the health insurance plan operated by the National Health Insurance Association (Kyokai Kenpo). Enrolment is mandatory. |
|
Benefits package definition and levels |
All schemes provide a similar comprehensive set of benefits, which is determined and approved by the National Government This includes: (i) medical examinations; (ii) provision of medication or materials for medical treatment; (iii) treatment, operations or any other medical treatment; (iv) in-home medical care management as well as caretaking and any other nursing involved in in-home medical care; (v) hospitalization or visiting a clinic, and caretaking and other nursing incidental to medical treatment provided there. Out-of-pocket expense ratio varies depending on income and age. In general, 70% of the cost is covered by the insurance and the remaining 30% is paid out-of-pocket. Different shares apply for preschool-aged children and people between 70 and 75 years old. In addition, regular medical check-up can be provided for free (or subsidy is paid), which it is not included in the benefit package of the national health insurance. However, depending on the mutual aid association, benefit levels including sickness benefit, maternity benefit, childcare leave allowance, long-term care allowance, disaster, or death can be higher than the national health insurance. |
|
Provider networks |
Generally, whatever types of mutual aid associations or private health insurance societies) people belong to, members can receive services from a hospital or clinic approved by Ministry of Health, Labour and Welfare, or directly managed by the social health protection scheme. For example, the health insurance law includes under the article 63 “(i) a hospital or clinic designated by the Minister of Health, Labour and Welfare […] or a pharmacy designated by the Minister of Health, Labour and Welfare […]; (ii) a hospital, clinic, or pharmacy which provides medical care or prescriptions to an insured person administered by a specific insurer and which is specified by the insurer; and (iii) a hospital, clinic, or pharmacy established by an insurer which is a health insurance society.” Some mutual aid associations, especially the mutual aid association for public servants, have their directly managed hospitals (see section on “Provision”). Yet members can freely choose their providers outside of directly-managed facilities. |
|
Implementation |
|
|
Education / Promotion |
Health insurance societies include specific health checkups and guidance depending on the conditions prevailing in the company, thereby acting similarly to occupational safety and health services. |
|
Enrolment / Renewal |
Enrolment happens at health insurance societies / mutual aid association levels. For health insurance societies a person in charge of health insurance is designated in each company. |
|
Revenue collection (if application) |
Contributions are deducted from contributors’ salaries. Contribution rates are set by health insurance societies and mutual aid associations. To limit deficits, contribution rates can be revised each year by health insurance societies and mutual aid association unit for short-term benefits including all health services. Employers / the State and employees / civil servants contributed equally, each half of the contribution. Contribution rates are capped at 13% of salary. The average contribution rate for health insurance societies is 10% of the salary. |
|
Pooling |
Pooling happens at the mutual aid association / health insurance society unit. However, it is legally possible for health insurance societies to pool their contributions to subsidize specific high-cost medical expenses and/or assist health insurance societies when they encounter financial difficulties. |
|
Purchasing |
Whichever facility is accessed, fee-for-service is applied and 70% of the cost is covered by insurers. The fee schedule is uniformised at national level and revised both at global and item-by-item levels |
|
Provision |
Some mutual aid association have their directly owned hospitals. However, the hospital needs to be approved by Ministry of Health, Labour, Welfare and service quality should be the same since it must meet with the quality and rules mentioned at Japan Medical Care Law (Law No. 205 of July 30, 1948). In the case of the Federation of National Public Service Personnel Mutual Aid Association there are 32 directly managed hospital by the association, Japan mutual aid association of public school teachers has 8 directly managed hospitals In this context beneficiaries are free to choose to access any hospitals and clinics in Japan. Yet some mutual aid associations provide discounts if members use their directly owned hospitals. For example, in mutual aid association for staffs of Ministry of Health, Labour, Welfare, a 20% discount applies if the participants use the directly managed hospital Similarly only some of the health insurance societies have directly own hospitals |
|
Claim management and reimbursement |
Hospitals and clinics calculate all expenses incurred monthly and apply to the “Healthcare bill check and payment organization”, which directly reviews claims and pays them, while charging the mutual aid association / health insurance society |
|
Feedback mechanisms (quality assurance) |
There is no official harmonized complaint system, but for any complaints from members, they can call their mutual aid association / health insurance society free hotline. |
10.3 Impact
As of today, health insurance societies and mutual aid associations are still major elements of the social health protection system in Japan. Under the Mutual Aid Association’s schemes, around 8.5 million people are covered (around half of this group of population is contributor, and the rest are their dependent (family members)
However, it is to be noted that health insurance societies are facing financial distress. In 2021, a 78% of the countries health insurance societies were expected to post deficits.81 While accelerated through the COVID-19 pandemics, the financial situation of health insurance societies has been chronically difficult. This situation is due to a continuous increase in benefits payment due to technology developments and ageing, while revenues from contribution decline with a dropping number of enrollees.
10.4 Lessons learned
Health Insurance Societies and Mutual Aid Association as enablers for Japan’s universal health coverage
Health insurance societies and mutual aid association pre-existed to the State’s attempt to provide social health protection for all. Back then, enrolment was on a voluntary basis and employers did not have the obligation to offer them to their employees. Benefit packages as well as contribution rates varied. The Japanese Government introduced regulation through the 1922 Health Insurance Law, when it became mandatory for companies of 10 employees or more to establish a health insurance.
Both health insurance societies and mutual associations responded to a concern and need for social health protection, expressed by the public opinion. They further enabled the extension of coverage through the 1958 Law, as they created a collective expectation on this regard.
State’s overall responsibility for social health protection
The Japanese government created a regulatory framework whereby health insurance societies and mutual aid associations are autonomous, yet it did not disengage from its overall responsibility to provide social health protection coverage to its population. At financial level, the governmental subsidizes health benefits expenditure of health insurance societies and partial or total amount of administrative costs of mutual aid associations, thereby providing financial support to these schemes. In addition, if a health insurance society has to shut down due to financial difficulties for example, the beneficiaries can be transferred to the Japan Health Insurance Association, a scheme directly managed by the State. The State therefore plays the role of insurer of last resort.
In the case of Japan, revenues raised through health insurance societies and mutual aid associations in the form of social contributions, create greater fiscal space for other categories of population not covered by these schemes. Namely, around half of the Long Term Care Insurance budget is funded from tax revenues
Greater coverage keeps health insurance societies and mutual aid associations attractive
Although the government support goes to National Health Insurance, health insurance societies and mutual aid association’s participants can receive benefits for different types of contingencies (such as maternity and sickness), while the national health insurance benefits are limited to healthcare. For this reason people are still motivated to join in their mutual aid association. In addition, dependent family members, including children, can be covered under health societies and mutual aid association schemes, while not covered in National Health Insurance.
In addition, health insurance societies and certain mutual aid associations can set a maximum rate of co-payment. If out of pocket expense go over a certain amount, the scheme can cover its expense as allowed by the Health Insurance Act by Ministry of Health, Labour, Welfare where it is set that 25,000 Yen per month can be advised to set as a maximum of patient’s out of pocket expense. This participated in the attractiveness of these schemes.
References
11. Lao PDR
11.1 Overview of the national social health protection system
The Government of the Lao People’s Democratic Republic (Lao PDR) made a strong commitment to provide social health protection for the entire population in its Health Sector Reform Strategy 2014-2025. Through this framework, the Government is aiming to ensure equitable access to health care services for all and protect households from catastrophic health expenditure, while moving towards achieving Universal Health Coverage (UHC) by 2025.
Over the past decades, the social health protection system has been reformed and expanded gradually. First, two schemes were initiated under the Ministry of Labour and Social Welfare (MLSW), one for the formal sector including civil servants, and the other for enterprises’ employees and their dependents. The compulsory plan for government officials was first launched in 1995 and revised in 2005. This scheme was managed by the State Authority for Social Security (SASS) with a view to provide social security including health protection. In 2001, the Lao Social Security Organization (SSO) was launched aiming to provide social security, including health benefits, to workers in the formal private economy.82 These two schemes are contributory, with contributions shared by employers and employees. Both SSO and SASS were established as semi- autonomous bodies under the MLSW. They were later merged under one umbrella and managed by the SSO, under the oversight of the MLSW as per the Law on the National Social Security System issued in 201883. The target population under this formal public and private employment scheme only accounts for around 20 per cent of the total population.
In order to extend coverage to those in informal employment and their dependents, the Government implemented various initiatives over the years:
-
A voluntary health insurance scheme (Community Based Health Insurance) was implemented under the oversight of the Ministry of Health (MOH) in 2002. This scheme was launched as a pilot and gradually extended in most provinces.
-
In addition, the MOH introduced a health protection scheme for the poor and vulnerable known as the Health Equity Fund (HEF) in 2004, mostly under the initiative of and with financial support from donors. This scheme not only provided health care benefits, but also other benefits such as daily allowance and transportation fees for the poor.
-
Additionally, in 2010 the Free Maternal, Neonatal and Child Health (FMNCH) policy was implemented to provide free care for children under 5 and free maternal care for pregnant woman, including delivery, ante-natal care and post-natal care. This was formalized as per Government Decree No 273 on subsidies for delivery and health care for children under 5, issued in 2014.
In parallel, the scheme for the military and police is operated separately from the social security system and managed under the respective ministries.
The next section provides insights on the history of the development of the Community Based Health Insurance (CBHI) scheme in Lao PDR, how it functions today in Vientiane Capital and how the foundations of the current National Health Insurance (NHI) scheme were laid.
History and development of Community Based Health Insurance in Lao PDR
In Lao PDR, the CBHI scheme was established as a voluntary health insurance scheme to provide financial health protection to those not covered by the SSO and SASS schemes and their dependents. A unique feature of Lao PDR’s CBHI was its direct implementation by the Government, as opposed to by communities. The design of the initial scheme is further detailed below (section in II.1), including its transition towards the current NHI scheme (II.2). The CBHI scheme now only exists in Vientiane Capital, as described below (in section II.3).
Early stages of CBHI implementation
The CBHI pilot schemes were initiated from 2002 to 2004 in different districts of the Central, Northern and Southern regions of Lao PDR, with technical support from the World Health Organization (WHO). All districts were concentrated in semi-rural or urban areas, where facilities were geographically accessible. In order to minimize the risk of adverse selection and provide some level of risk pooling, enrollment was family-based. The contribution was designed as a prepayment, the amount of which was proportional to the number of household members. The collection of contributions was undertaken at the village level through village collectors with the support of the village authorities.
The benefit package was set in an implicit manner and covered outpatient services and inpatient care, including surgery, delivery and caesarean section with some limited exclusions84 (see details in the regulations and guidelines on the implementation of CBHI, annex 2 and 3). The health care providers’ network included district hospitals and provincial hospitals in the catchment area as the first entry point in the health system, with a strong gate keeping system to access the referral hospital. Capitation was the main method of provider payment for both outpatient and inpatient care. The share of capitation between the main contracted and referral hospital was made on the basis of negotiations and based on the level of care of providers.
The district health insurance office worked as an account manager for CBHI, and contributions were pooled at district level. Not all villages of a district were automatically included in CBHI scheme, depending on availability of health care providers.85 At central level, the CBHI team was in charge of defining rules governing the schemes as well as monitoring, supervision and support to provincial and district operations, and negotiations with the hospitals.
Towards the end of the pilot phase in 2006, the CBHI team implemented technical adjustments on CBHI regulations such as benefit packages (treatment of diabetes was added for instance), invested in capacity strengthening, and developed tools such as promotion materials. Upon completion of the pilot, the implementation of the scheme was expanded. From 2009 to the end of 2012, the extension and capacity strengthening of CBHI was accompanied by AFD financial support and GRET-Swiss Red Cross technical assistance, covering the two provinces of Savannakhet and Vientiane Capital, encompassing 15 districts and nine districts respectively. This support extended to account managers at district level.
By 2012 the CBHI scheme was present in 42 districts of nine provinces but only effectively covering 178,000 people or 3 per cent of the total population.
Move towards subsidies
At this time, it became clear that the CBHI had limited capacity to extend coverage on a voluntary basis and without subsidies to cover a population with limited and irregular incomes. The Government opted for the provision of partial subsidies to the contributions, and introduced a 50 per cent government subsidization of contributions to CBHI through the adoption of Decree 470/PM (art. 11).
Decree 470/PM also introduced major changes to attempt to reduce fragmentation of the social health protection system. The first step was to place most of the existing schemes (SASS, SSO, CBHI and HEF) under one umbrella, thereby creating the NHI. The National Health Insurance Bureau (NHIB) was launched in 2013 with a view to create a single purchaser in Lao PDR. In line with Decree 470/PM, the management of the scheme was promoted from the CBHI Division under the MOH Department of Finance to the NHIB as one department of the MOH, facilitating more negotiating power with health care providers. This management structure was then replicated at lower administrative levels through provincial health insurance and district health insurance offices.
In 2014, a pilot of 50 per cent subsidies was launched in one district of Lao PDR with financial and technical support from ILO, WHO, Luxemburg and the EU. The rolling out of this policy started from 2015-2016 through the government budget. However, despite continuous efforts from both government and development partners, it failed to expand coverage significantly as no compulsory measure was foreseen and contributory capacity remained limited among the target population. By 2016, the scheme reached 51 districts in 17 provinces reaching 5 per cent of its target population.
Figure 1. Social Health Protection coverage as % of the target population in 2006
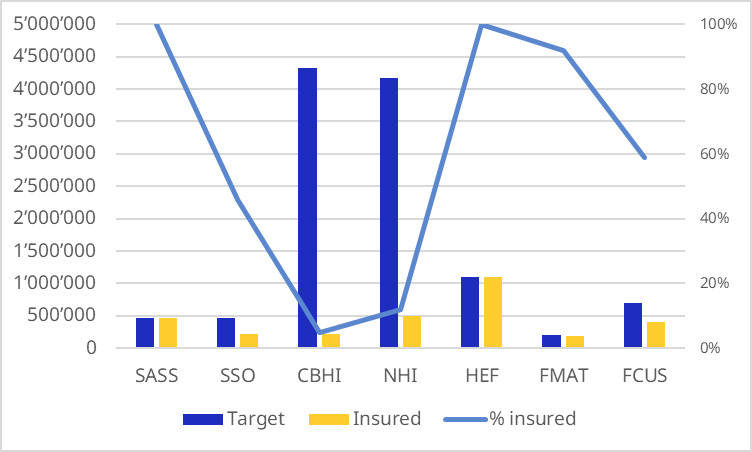
Source: NHIB. Key features of social health protection in Lao PDR for the year 2016.
The idea of shifting financing mechanisms towards a more tax-based approach with no prepayment was considered. The decision was made by the MOH to move towards full subsidies financed by the Government’s general revenues to all those not covered by the NSSF. The reform also included the continuation of small co-payments at the time of use for subsidized members, and the integration of CBHI and HEF. This was first piloted in three of the smallest and poorest provinces, namely Luangnamtha, Attapeua and Saysomboon, in the middle of 2016. It was then quickly expanded throughout the country at the end of 2017.
The public subsidies allowed a rapid increase of population coverage, which reached up to 90 per cent as of 2023. The system was not rolled out to Vientiane Capital,86 where the CBHI system remained active to provide a voluntary option to access financial health protection. This signaled the end of the CBHI approach, with the exception of Vientiane Capital. Through the expansion of the NHI scheme, the free MCH scheme was also merged under the NHI Bureau, while the free MCH scheme in Vientiane Capital still provides benefits to target populations in nine districts of the province.
Building from the initial period of implementation of the NHI scheme, the Health Insurance Law was developed and endorsed in December 2018.87 Along with this, the merging of the segmented social health protection schemes introduced by Decree 470/PM was further materialized.88 A pilot was implemented in the beginning of 2018 and completed at the end of 2018, leaving active military scheme members with their respective social security scheme outside of the merger. Retired persons and dependents of formally employed workers are included in the LSSO scheme.
Today, the NHI benefit packages provided to beneficiaries are comprehensive, covering outpatient and inpatient services including high-cost treatments with some limited exclusions. The poor, pregnant women, children under 5 and members of formal sector schemes do not pay co-payments at the point of service. However, in Vientiane Capital, the population either relies on CBHI, which remains in service, or on the voluntary NSSF scheme to be protected against health risks.
Adjustment of the CBHI in Vientiane Capital
-
Governance and design
The health insurance fund in Vientiane Capital is currently managed by the provincial NHI office under the oversight of the Vientiane Capital Management Committee. With the reform in Vientiane Capital, the responsibility for financial management has moved to the Vientiane Capital health insurance unit under the oversight of the management committee. The NHI unit plays the role of purchaser for health care services and monitoring the progress of the scheme. It reports to the management committee and the NHIB central level.
The design of the CBHI scheme in Vientiane Capital was initially similar to the schemes implemented outside the capital city. Later, the scheme was adapted to the urban context and needs of the target population. Formalized through the development of new CBHI regulations for Vientiane Capital, the reform had several components including the modification of contribution collection methods, the adjustment of the premium rate, the pooling of funds at Vientiane Capital level, and a change of provider payment mechanisms.
The reform also aimed at enhancing financial management, in particular contractual arrangements with central hospitals, in order to improve the providers’ responsiveness and attract more members through enhanced quality of health care services (see the annex summary table for the reform). In accordance with this reform, the contribution rate increased, and the collection period was set at least quarterly or annually with incentives provided for longer term payments. In addition, people had the choice to select the package or option for payment in relation to the choice of main provider (district hospital or central hospital). The rate of contribution was higher for package 1, for which the central hospital is the main provider. Various payment points were set up to increase accessibility of the CBHI: people were given a choice to pay the contributions at the village level through a village collector, at the district Health Insurance office through the CBHI account manager, or through the Vientiane Capital Health Insurance office at the Provincial Health Office. During this period, a web-based system was developed and used for registration of members, which provided a choice for people to enroll where convenient, and create the opportunity to pool the funds collected. Funds were pooled at Vientiane Capital Health Insurance scheme office where the contract with providers was established.
The table below summarizes the key features of the CBHI scheme in Vientiane capital, as implemented today.
Table 1. Key features of the CBHI scheme
|
Category |
Features |
|
Population coverage |
In 2021, the scheme covered about 24,789 members or 3 per cent of the total population in Vientiane Capital |
|
Financing |
The scheme is financed by contribution and government allocations (human resources, some running costs and top-up of the contributions paid by the NHI). Contributions: There are two types of benefit packages, with different levels of contributions: Type 1:110,000 kip/person/year (average) Type 2: 80,000 kip/person /year (average) Lower rate applies for bigger families. |
|
Enrollment |
Household based voluntary enrollment. Quarterly payment is required (See contribution collection). |
|
Benefit design (benefit package, cost coverage) |
Benefit package is rather comprehensive. It includes OPD services and IPD services including surgery. Exclusions remain: Heart surgery, organ transplantation, easthetic surgery, thalassemia, hemodialysis, sterilisation (except when prescribed by doctors), traffic accidents, artifical tooth or teeth adjustment, chemiotherapy and radiotherapy, eye glasses or artificial lenses, medical check ups for documentation purpose etc. No co-payment at the time of use. In addition, the scheme in VT Capital also provides a small cash benefit as a funeral grant for the member’s family in case of death. |
|
Eligibility conditions |
The qualifying period is set as one month for all services for new members who have paid the full amount of contributions (quarterly or more). New members can pay in installments (monthly) but they will be eligible only one month after completing at least a quarterly payment. Members must have been registered for more than 6 months in order to be eligible for funeral grant. |
|
Network of health care |
Public health facilities only. People in VT Capital must select a main contract hospital which will be their point of entry to the health system. They can choose between a district hospital or central hospital and can change on a yearly basis. Package 1 - central hospital as entry point (or main provider): Beneficiaries can use the services at their selected hospital directly. In case of emergency, they can go to another hospital but need to inform their main/contracted hospital within 72 hours. In terms of referral, the main/contracted central hospital can refer patients to another hospital for the necessary medical purpose. However, payment to the hospital selected (outside the contract) is borne by the main/contracted hospital. Package 2- district hospital (usually closest to the living area) - as entry point (or main provider). Beneficiaries have to use the district hospital as first contact, which plays the role of gate-keeper. If referral is needed, the main contractor will send patients to the connected central hospital or referral hospital under the contract. In this case the capitation method is used and shared by the main contractor and referral hospital. |
|
Education/promotion |
Promotion is undertaken by local level/district and village team with the support of Vientiane Capital team through awareness campaigns, using communication tools such as posters, leaflets and brochures. |
|
Affiliation/registration/rewards |
Registration is household based. Registration is completed based on the names listed in the family book and per individual for monks and students living in dormitories. Registration is completed on the basis of supportive documents from related institutions. |
|
Contribution collection (if applicable) |
The collection can be undertaken by village collectors, village funds, district account managers, or premium collection units at the Health Insurance division of Vientiane Capital. Households can register all year round with the district account manager and provincial health insurance office. The period of time is set as twice a year for the registration with the village collector/village fund (first session is in October-November – December; second session is from May- June – July). |
|
Risk pooling |
Risk pooling is at provincial level (VT Capital) and not district based as before in the rest of the country. A small reserve (about 5 per cent of contribution collected) from the contributions is available to use for unexpected health care claims/expenditures, and system development such as IT improvement or maintenance. The use of this reserve fund needs to be approved by the Director of Vientiane Capital Health Office as Vice Chair of CBHI management committee. |
|
Purchasing |
The VT Capital health insurance unit issues the contract with contracted hospitals to provide the health care benefits to members through capitation for both OPD and IPD, and additional payment for some determined high cost and risk adjusted capitation for six defined diseases. |
|
Health services delivery |
Members need to use the services at the main contract hospital that they selected. In cases where their main contract hospital is a district hospital, the referral hospital will be mandatorily selected following the national referral system. In cases where the central hospital is selected as the main contractor, the member can use that central hospital directly or the district hospital linked to the selected central hospital. |
|
Claim management |
The provincial health insurance office is in charge of claim management with support from NHIB. The claim is first reviewed by the provincial team before sending to NHIB for funding request |
|
Complaints and Appeals |
The hospital team in charge of HI receives complaints and appeals, which are then passed to the CBHI management committee at district level, and then to provincial and central level for final consideration. |
-
Main challenges
Vientiane Capital has a population of around 900,000 persons, with an estimated target of 70 per cent coverage for the CBHI scheme. However, the extension of coverage as a voluntary scheme seems to be very challenging to achieve. It is particularly difficult for the CBHI team to convince the population to join the scheme, due to the voluntary nature of the scheme, limited understanding of entitlements, and subsequent dissatisfaction of members with benefits covered. In addition, due to the uncertain status of the roll out of the NHI to Vientiane Capital, there is reluctance to implement CBHI awareness campaigns which could improve coverage.
From the operational side, the Vientiane Capital Health Insurance team remains small, and not fully capacitated to manage all the health insurance functions. In this context, the relation between the CBHI scheme and the health providers poses particular challenges. The capacity of the Vientiane Capital health insurance unit, both in terms of power and technical capacity to negotiate with central hospitals, is limited. This is compounded by low capitation rates, which create dissatisfaction from the hospitals and limited incentive to provide quality care to the patients covered by the CBHI.
There is no medical benefit management system as the health insurance office only focuses on fund collection and the claims review is done with the support of the NHI central team.
According to the 2022 yearly report on CBHI in Vientiane Capital, CBHI members in Vientiane increased from 25,220 in 2021 to 27,364 in 2022, with 2,575 new members. Although, membership is gradually growing and membership variation due to dropout is limited, the implementation of the CBHI in Vientiane Capital has proven difficult, especially in terms of coverage extension and sustainable financing.
11.2 Delegation of administrative functions / linkages between CBHI and national health insurance
Prior to Decree 470 on National Health Insurance
In 2000, the oversight and management functions of CBHI were established at both central, provincial and district levels, in accordance with CBHI regulation No 723 issued by MOH, dated 13/4/2005. The Management Committee of CBHI was responsible for the oversight of the scheme and this was broken down at all levels. This Committee was chaired by the Vice Minister of Health and formed by the representation of concerned stakeholders such as the Department of Finance and the Department of Health, which represented providers, and population representatives through Labour Unions. At district level, CBHI beneficiaries, such as senior persons and village collectors, were included.
At central level the Health Insurance Division was established under the Department of Finance and Planning at the MOH, to develop and implement the CBHI scheme. It played the role of secretariat to the Management Committee of CBHI at central level. At the local level, Health Insurance Offices were also established as branches at provincial and district levels following the establishment of the management committee. The core functions of the health insurance office included the following: awareness campaigns, premium collection, pooling, purchasing/contracting, claims processing and conflict resolution, including capacity strengthening and scheme development with some variations according to the management level (central, provincial and district). This structure allowed for a high degree of centralization and therefore harmonization of CBHI implementation, while enabling representation of key stakeholders at all levels.
Initially, it appeared difficult to recruit skilled staff members to operate in the field of health insurance and health care financing, as the scheme was new in the country, and academic training was almost non-existent. In addition, there were few staff members qualified in financial management, especially at the local level. Thus, most district health insurance offices had to hire volunteers to work as account managers for the scheme. Recruiting of additional staff members was also limited by imposed recruitment quotas of Government. The centralized management model meant that the expertise – such as payment and monitoring – was concentrated at central level, with the duty to capacitate and supervise lower administration levels.
After the implementation of Decree 470 on National Health Insurance
In April 2013, in accordance to the NHI Decree No 470/GO
At the provincial level, the health insurance office is operated as a section under the Provincial Health Office. The Health Insurance provincial management committee is chaired by the Provincial Governor and provides oversight to health insurance management. Similar to the provincial level, the district health insurance office is mostly placed under the District Health Office. The district health insurance management committee is chaired by the district governor, in order to increase proximity to the local population.
The function and mandate of health insurance offices at all levels have been developed with the aim to increase potential for institutional strengthening and ease the management and pooling of the fund from different social health protection schemes in the future, as stipulated in the NHI Decree no 470/GO.
11.3 Impact and results of the coverage provided by the CBHI
Impact on population coverage
The population coverage under Community Based Health insurance scheme has historically remained limited, in spite of the Government’s efforts in implementing awareness campaigns and improvement to the system. The voluntary nature of the scheme made it difficult to encourage people to join and contribute. The renewal of memberships was particularly challenging, with high drop-out rates. The voluntary registration also exposed the scheme to adverse selection even though this was partially limited by the household-based enrollment.
As an illustration, the graph below depicts flat membership trends over the months in the year 2011 for a selection of districts in which the CBHI is implemented.
Figure 2. Monthly trend of membership per province in 2011
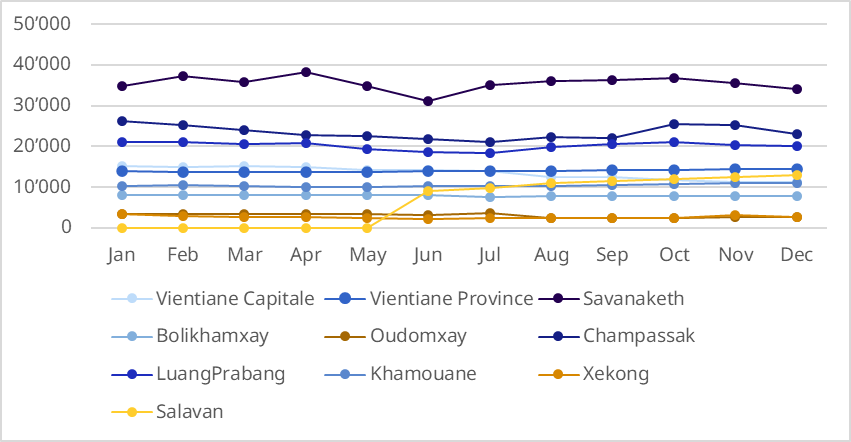
Source: Ministry of Health, CBHI Annual data report 2011.
Following the implementation of full subsidies to all those not covered by the NSSF, and without requiring any pre-registration mechanisms, a rapid expansion of the National Health Insurance scheme took place. It increased from covering a mere 10.5 per cent in 2008 to 94 per cent of the total population covered in 2018 (see figure3). The majority of its members are covered under subsidies (see figure 3 below).
Figure 3. Coverage of social health protection scheme in Lao PDR (2008 - 2018)
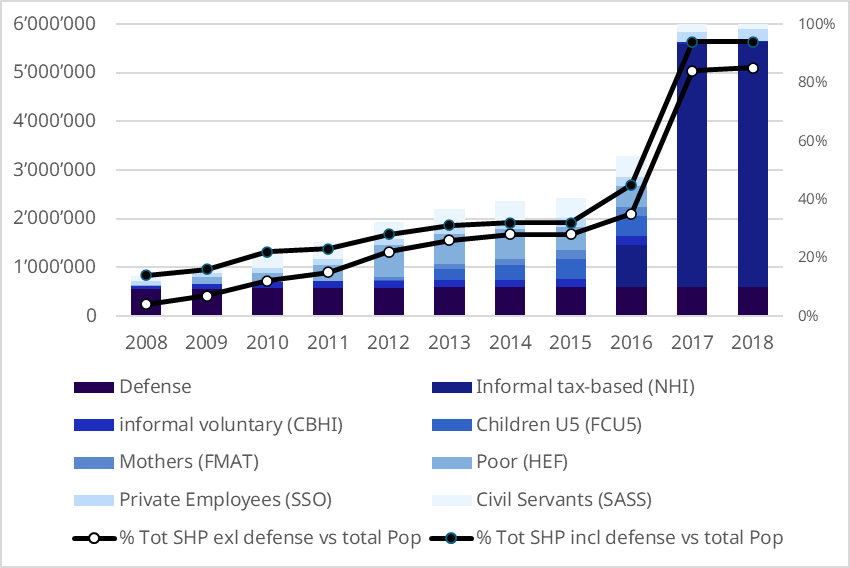
Source: NHIB. 2019. 10 Key features of SHP in Lao PDR for year 2018.
In Vientiane Capital, although CBHI membership increased regularly from 2016, coverage remains limited. The number of members in Vientiane Capital increased from 14,021 people in 2016 to 27,364 people in 2022 (see the graph below). However, it only represents 3 per cent of the population in Vientiane Capital, estimated at about 900,000 inhabitants.
Figure 4. Trend of CBHI membership in Vientiane Capital
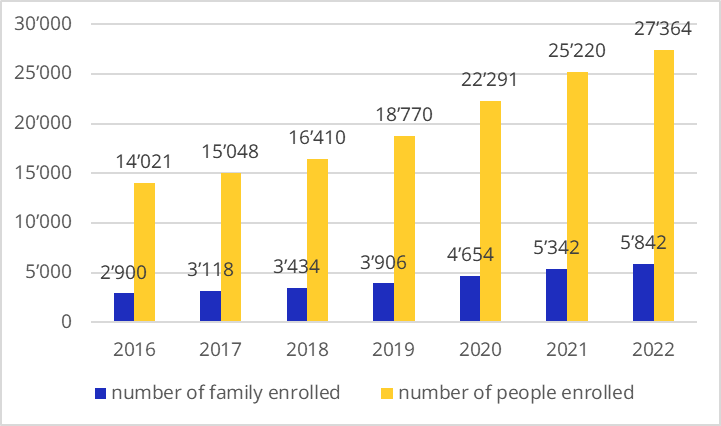
Source: Ministry of Health, NHIB, trend of CBHI membership in Vientiane Capital (internal data provided by MoH).
Impact on access to health care
The CBHI scheme seems to have had a positive impact on accessibility of health care services. The trend of health care utilization under different social health protection schemes from 2008 to 2016 (before rolling out of the full subsidies) shows higher utilization rates for CBHI members compared to other schemes, as well as increases in utilization over time (see figures 3 and 4 below). Factors contributing to higher utilization among CBHI members compared to other schemes are not known. The phenomena could be explained by adverse selection, moral hazards or higher health care needs, but could also be due to the impact of greater proximity to facilities or greater empowerment of individuals with regard to the CBHI scheme.
Figure 5. Trends in outpatient visits by different social health protection schemes (2008 – 2016)
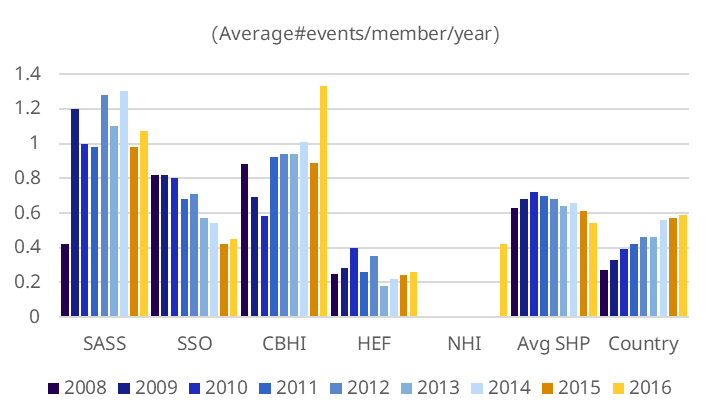
Figure 6. Trends in inpatient admission by different social health protection schemes (2008 - 2016)
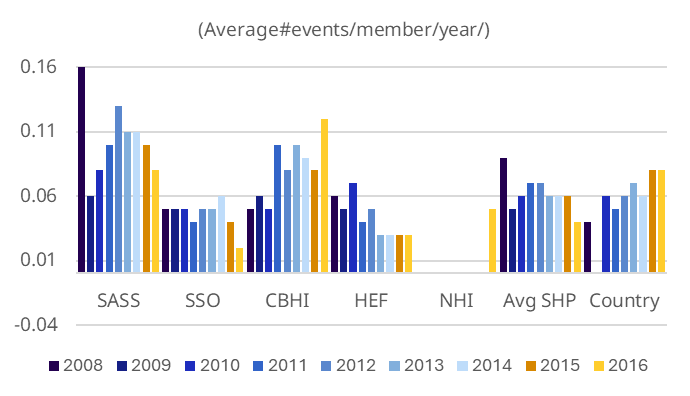
Impact on financial protection
Data on the impact of the health insurance schemes on financial protection is limited compared to data on utilization. There are no clear data or studies on the impact of health insurance, including CBHI, on the level of out-of-pocket (OOP) health expenditure and the incurring of catastrophic health expenditure89 under CBHI.
Data from the Lao Expenditure and Consumption Survey (LECS 3 and 5) show a decrease of catastrophic expenditure from 2.67 from 2002-2003 to 1.70 from 2012-2013. Given the low social health protection coverage at that time, it is unlikely that the various schemes (SSA, SSO, HEF, free maternal and child care) played a major role in this decrease.
Figure 7. Catastrophic incidence by quintile

OOP expenditure as a share of Total Health Expenditure decreased from 48.6 per cent in 2010-2011 to 45.1 per cent in 2015-2016.90 The OOP health expenditures as a percentage of household expenditures is higher among households in the richest quintile, which could be due to utilizations of private facilities or tertiary level of public system.
Table 2. OOP spending on health as percentage of total household expenditure and capacity to pay, based on diary data (LECS 5 2012-2013)
|
Average OOP |
OOP% of capacity to pay |
OOP % of total household expenditure |
|
|
Poorest |
6,831 |
2.9% |
0.8% |
|
Q2 |
11,948 |
3.1% |
0.9% |
|
Q3 |
24,189 |
3.1% |
1.4% |
|
Q 4 |
56,044 |
3.8% |
2.1% |
|
Richest |
169,928 |
3.2% |
2.4% |
|
Average |
53,751 |
3.2% |
1.5% |
Other impacts from the design of CBHI on provider
The CBHI scheme faced several challenges related to its voluntary nature. Research on the impact of CBHI on providers is limited but some issues were raised based on annual reviews.
Firstly, in Lao PDR, the capitation was defined by the amount of contribution collected minus the incentive for village collectors and account managers, and the small administration budget for the district health insurance office. Therefore, the capitation rate was not set through a refined formula based on actual utilization and costs, but depended only on the number of households enrolled in the scheme and the amount collected in that period. Payments to facilities were then directly impacted by delays in contributions payment and dropouts.
In addition, the hospitals experienced a sudden increase of workload with an increased influx of patients. In 2011, the average increase was 28 per cent and 15 per cent of OPD and IPD of hospital activities respectively.91 The hospitals considered that the capitation payment rate was insufficient to compensate the health care services provided to CBHI members. Most hospitals claimed they were facing financial deficits when comparing the capitation paid to the reported charges, especially for referral hospitals. For instance, data from 2011 showed the gap between average capitation paid to the hospital of 47,738 Lao Kip/member and the reported charge per capita amounting to 64,623 Lao Kip.
Current National Health Insurance – what is the CBHI legacy ?
-
Design and financing
The NHI scheme design was informed by the experience of the CBHI scheme. For instance, the NHI benefit package was defined on the basis of the package proposed by the CBHI and has the same exclusions. It was later adjusted gradually to align with current health needs and high-cost services such as high-cost surgery, hemodialysis, chemotherapy, and CT scans. The waiting period was removed. Regarding the purchasing of health care, the NHI maintained the same CBHI model, with a network of public providers, and implementation of a referral system. Payment by capitation was maintained for OPD services, with the addition of case based for specific IPD services.
A major difference between CBHI and NHI lies in the financing mechanisms used. Upon learning that the voluntary nature of the CBHI scheme and the absence of subsidies would make it difficult to extend CBHI population coverage on a contributory basis for workers in informal employment and their dependents, the Government mobilized public funding to provide tax financed coverage to this share of the population. This addressed the failure of the prepayment system of CBHI in relation to coverage extension. As noted above under Section I, after the issuance of the NHI Decree, the pilot of 50 per cent contribution subsidies for CBHI members was applied, but quickly replaced by full subsidies in mid-2016. This was launched without strong legal support, but its implementation followed the Decree on Health Insurance No 470/GO. De facto, the CBHI functions of registration and contribution collection disappeared.
Co-payments were introduced with the implementation of the NHI to create an additional source of income, but were kept to a minimum to avoid creating financial barriers to access.
-
Management and governance
The development of the health insurance infrastructure and the technical capacity from the experience gained from the CBHI scheme allowed the country to implement the new national health insurance scheme with ease. Several design components of the CBHI were adjusted in order to align with the current situation, as well as the governance and management arrangements. The health insurance division was upgraded to a Department of the MOH. The core staff of the health insurance office, at both national and local levels, had been involved in the preparation and implementation of the CBHI scheme. Prior to the launch of the NHI scheme, the health insurance office was very small and established only where CBHI was present. Based on the HI Decree No 470/GO, the roles and responsibilities of HI were developed and rolled out nationwide before the launching of the NHI scheme.
The CBHI scheme was administered by the health insurance office under the supervision of CBHI management committee at their respective levels. The management of the scheme at district level focused on the collection of contributions and played the role of fund holder and purchaser of health care services. In the case of the CBHI scheme, the staffing of the HI office was very limited, especially at the district level which partially relied on volunteers and donor funded positions. Building from this, the NHIB team is currently growing both in terms of size and capacity, although policy and technical capacities remain concentrated in Vientiane.
Most of the technical functions of the health insurance, such as provider payment calculation, negotiations with providers, communication, supervision of provincial and district offices, and so on, were also developed under the CBHI scheme, which contributed to the current implementation of the NHI. The tools used in the CBHI scheme have been adjusted and applied to NHI, including for the monitoring system. Initially implemented with multiple paper-based forms, the system was later upgraded to a web-based system, with the introduction of NHI. Despite this improvement, a comprehensive and modernized online system is still needed to facilitate easier management of data and claims payments.
The table below provides a summary comparison of the CBHI model with the current design and operational functions of the NHI.
Table 3. Comparison of the CBHI model before Decree 470 and NHI today
|
Function |
CBHI before Decree 470 |
NHI today |
|
Population coverage |
5 per cent of total population (data 2016). This does not include the poor as they are registered under the Health Equity Fund. |
93 per cent of total population covered, 73 per of which are workers in the informal economy, including the poor. |
|
Enrollment |
Voluntary enrollment, household based. |
Workers in formal employment: enrolled through NSSF, under the employer’s responsibility No enrollment for population not covered by the NSSF. Presentation of an ID is enough to access services. |
|
Benefit design (benefit package, cost coverage) |
The benefit package is quite comprehensive and defined with both negative and positive definitions. It covers consultation & admissions incl. surgeries with no co-payment or formal additional payment. Exclusion: Individual request, care provided at private facilities, selected high- cost services, already paid for services such as vertical programme. |
The benefit package is quite comprehensive and defined with both negative and positive definitions. It covers consultation & admissions incl. surgeries with no co-payment or formal additional payment. Exclusion: Individual request, care provided at private facilities, selected high-cost services, already paid for services such as vertical programme. Introduction of a small flat rate co-payment applied at the point of service. Rates varies by level of health facilities such as HC, DH and PH. Exemptions apply for the poor, vulnerable, pregnant women and children under 5. In addition, the poor are eligible for non-medical benefits for hospital admission and referral such as daily allowance and transportation. |
|
Eligibility conditions |
The qualifying period is set as 1 month for OPD, 3 months for IPD, 3 months for acute surgery and 6 months for surgery and delivery. People with late contribution payment or renewal payment continue to be covered during a 3 month period (known as the “warning period”). |
Patients who come with updated identification document are eligible to use services without waiting period. |
|
Network of health care providers |
The contracts were established with public hospitals in their specific catchment areas. Usually district hospitals were the main contractor and provincial as referred through gate keeping system. Health centers were subcontracted from district hospitals. |
Covers all public hospitals (HC, DH, PH/RH and central hospital in case of necessity). There is no strong referral system for IPD cases as people can choose to use the IPD services at DH type A and PH but need referral for CH. However, for OPD cases, patient has to follow the gate keeping system otherwise they have to pay for health care services. Only one private hospital is piloted as a referral hospital for provincial hospitals in one region. In Vientiane capital where the NHI is not implemented as in the provinces, the Central Hospital only functions as a referral hospital, without third-party payment. |
|
Education/promotion |
Promotion and awareness campaigns are conducted by the CBHI office with the support of local authorities using leaflets and brochures including through the village speakers. |
Promotion and awareness campaign is undertaken at local and national levels through meetings, workshops, media and hotlines. |
|
Affiliation/registration/rewards |
Village collector and district account manager are established to ensure membership registration and contribution collection. They are paid a small “reward” based on the percentage of contribution collected (about 2,000 Lao kip per family, roughly 10 per cent of contribution collected). |
NSSF members register through their employers. No registration is required from the rest of the population. Family book or other identification letter are used to certify their identity at the point of service. |
|
Contribution collection (if applicable) |
Contribution is collected by village collector and account manager of DHI Office. The collection is set as monthly payment rate but people encouraged to pay for several months in advance. The contribution is set in accordance to family size categories with reduced rate for larger family such as single family, 2-4 members, 5-7 members and 8 or more member families. Average rate was about US$5 per person/year. |
Contributions for health and other social security benefits to the NSSF are paid on a monthly basis, through salary deductions. The share corresponding to health (1.25 per cent) is remitted to the NHIB. No contributions collected for the rest of the population. Patients need to pay co-payment at the time of use of services. |
|
Risk pooling |
Risk pooling took place at district level with no cross-subsidization between districts. Family enrollment limited adverse selection to some extent |
Larger risk pooling as NHI covers the entire population (national population), except Vientiane Capital. |
|
Purchasing |
The management committee and health insurance office at district level played the role of purchaser to manage contract with contracted providers, including both main and referral hospital to provide health care services for the members. Central and Provincial management committee participated in the contract signing as witnesses. Capitation used for both OPD and IPD and the split of capitation between main contractor and referral hospital is based on the rules of CBHI and the agreement of related providers prior to the contract signing, especially related to the capacity of the main provider. The rate of capitation payment depends on the money collected as the scheme is design to pay main contracted and referral hospitals 90 per cent of money collected, while 10 per cent is used for collector incentive and administration for CBHI at district level. |
There is no contract with public health facilities which are de facto covered. Capitation is used as payment mechanism for OPD services. Capitation rates are based on utilization rate of previous years and supposed to be revised for inflation. Rates vary by level of facilities. Case based payment applies for IPD and some OPD cases such as minor surgeries and hemodialysis. Different case base rates applied by level of health facilities (health center, DH type A, DH type B, PH and Regional hospitals) but are uniform across the country (same rate for same level of health facilities). |
|
Health services delivery |
From primary to tertiary care with gate keeping system. The beneficiaries can choose their first contracted provider. No co-payment made at the service site. |
From primary to tertiary care with gate keeping system. The beneficiaries can choose their first contracted provider. No co-payment made at the service site for NSSF members, pregnant women, children under 5 and households identified as poor. Others pay a small co-payment. |
|
Claim management |
Third party payment applies. No review of specific claims, since hospitals are paid through capitation. |
Third party payment applies to health insurance offices at all levels under the supervision of NHI Management Committee to ensure the claim review and payment to facilities. |
|
Complaints and Appeals |
Hospital team in charge of CBHI receives complaints and appeals which are then passed to CBHI management committee at district level, and then to Provincial CBHI management committee for final consideration. |
Complaints and appeals are made to National Health Insurance Bureau or to the Health Insurance Management Committee at their respective level for consideration. |
11.4 Conclusion
The CBHI scheme in Lao PDR was the first attempt by the State to provide social health protection to households relying on the informal economy nationwide. While it did not achieve satisfactory population coverage due to inherent design limitations (namely the voluntary nature of enrollment), its legacy has determined the later design and rollout of the NHI scheme in Lao PDR. The experience of CBHI has triggered an increase in the utilization of health services and had a potential impact on the reduction of OOP expenditure.
In addition, while evidence is scarce, it seems that CBHI has helped to build capacity at all levels, which later became an enabling factor for the rollout of the NHI scheme. In addition, communities and providers were already sensitized to the principles and benefits of health insurance, creating fertile ground for the extension of the NHI.
However, this legacy is not a panacea. Financial sustainability relies heavily on the government budget, and the Government’s future commitment to continue financing NHI subsidies is uncertain. Current allocations are already insufficient to pay for health facilities at the current payment rates, while these must also be increased to better reflect real costs and inflation. In this context, the roll-out of NHI subsidies to persons working in the informal economy in the Capital city is unlikely in the near future.
Today in Vientiane Capital, in the absence of this roll out, the CBHI scheme constitutes one option, in addition to the NSSF voluntary scheme, for people to access some level of financial protection against health risks. However, coverage remains limited to a small proportion of the population. The ongoing revisions of the Law on Health Insurance and the Law on Social Security provide an opportunity for reforms towards the extension of coverage. In particular, the provision of subsidies for vulnerable households, the enforcement of compliance to boost registration with the NSSF, as well as the integrated management of the schemes in Vientiane Capital, are anticipated to accelerate progress Universal Health Coverage in Lao PDR.
References
ADB Institute (2019). Quality of health care in the Lao People’s Democratic Republic https://www.adb.org/sites/default/files/publication/515076/adbi-wp981.pdf
Alkenbrack, S. E. (2011) Health insurance in Lao PDR: examining enrolment, impacts, and the prospects for expansion. Thèse de doctorat, London School of Hygiene & Tropical Medicine. DOI: https://doi.org/10.17037/PUBS.01544173
Alkenbrack et al. (2013). Achieving universal health coverage through voluntary insurance: what can we learn from the experience of Lao PDR? https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3893613/
Banque mondiale (2010). Community-Based Health Insurance in Lao P.D.R. Understanding Enrollment and Impacts.
Bodhisane, S. (2019). Factors affecting the willingness to join community-based health insurance (CBHI) scheme: A case study survey from Savannakhet Province, Lao P.D.R https://pubmed.ncbi.nlm.nih.gov/30549109/
Chaleuvong, K. et al. (2020). Factors affecting knowledge of National Health Insurance Policy among out-patients in Lao PDR: an exit interview study https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7480647/
Ministère de la Santé, «Community Based Health Insurance Development in Lao PDR», présentation Powerpoint du Directeur AMBC. https://www.asean-ssa.org/files/ASSA%20Board%20Meeting/LAO%202008/Implementation%20experiences%20of%20Community%20Based%20Health%20Insurance%20(CBHI)%20Scheme%20in%20Lao%20PDR.pdf
NHIB (2017). Key features of social health protection in Lao PDR for the year 2016.
Organisation internationale du Travail, OIT (2021a). Social protection in action: building social protection floors for all: Country brief: Lao PDR https://www.social-protection.org/gimi/Media.action?id=18725
— (2021b). Extending social health protection: Accelerating progress towards Universal Health Coverage in Asia and the Pacific. https://www.ilo.org/publications/extending-social-health-protection-accelerating-progress-towards-universal-0
— (2024). Social Protection Floors in Action: 100 success stories to achieve Universal Social Protection and SDG 1.3.1. Moving towards universal social health protection in Lao PDR https://www.social-protection.org/gimi/Media.action?id=16917
République démocratique populaire lao, ministère de la Santé (2012). CBHI Annual data report 2011.
République démocratique populaire lao, ministère de la Santé, NHIB (2019). 10 Key features of SHP in Lao PDR for year 2018.
Sydavong et al. (2019). «Potential demand for voluntary community-based health insurance improvement in rural Lao People’s Democratic Republic: A randomized conjoint experiment». https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0210355
12. Mali
Background
The process of building a national system of universal health insurance began in the 1990s, and has evolved in line with policies and strategies on social protection, including:
-
the National Solidarity Policy (PNS) developed in 1993, which promotes the creation of new systems, including mutual health insurance schemes and new structures such as the National Solidarity Fund, the Caisse nationale d'assurance maladie (National Health Insurance Fund, CANAM) and the National Medical Assistance Agency;
-
the Declaration of National Social Protection Policy (PNPS), adopted in 2002, reinforced the key areas of the PNS and laid the foundations of the current SHP architecture with the creation of Compulsory Health Insurance (AMO), the Régime d’assistance médicale (Medical Assistance Scheme, RAMED) and the strengthening of the mutual society movement;
-
the Plan d'actions national d'extension de la protection sociale (PAN-EPS) 2005–2009, which is based on the PNPS, aims to gradually extend the personal and material scope of social protection, with the goal of covering approximately 15 per cent of the population with social security schemes, and organizing health cover for 6 per cent of the elderly, 3 per cent of the population with mutual insurance schemes and 5 per cent of the population with the Fonds d'assistance médicale au profit des indigentes. While these goals have only been partially achieved, the action plan has led to the adoption of legislation on AMO and the RAMED;
-
the National Action Plan for the Extension of Social Protection (PAN/EPS) 2011–2015 aims to help strengthen existing systems and gradually extend the scope of contributory and non-contributory social protection mechanisms in Mali by 2015. One of the expected results of this action plan is the development of mutual societies and other solidarity-based organizations, so that people not covered by compulsory schemes can benefit from basic social cover;
-
the National Health Financing Policy for the Universal Health Insurance Scheme (RAMU) 2014–2023;
-
the adoption in 2011 of the Stratégie nationale d'extension de la couverture maladie par les mutuelles aux secteurs informel et rural (SNEM) 2011-2015, with the aim of extending health cover to the agricultural and informal sectors through mutual health organizations;
-
the ten-year Health and Social Development Plan (PDDSS) 2014–2023, which highlights the low level of coverage expected from AMO, mutuals and the RAMED and promotes energetic measures to strengthen and extend these mechanisms, in particular the gradual introduction of an appropriate, coherent and comprehensive national health insurance management system.
As part of this process, Mali introduced an initial system in 2009 based on:
-
a compulsory health insurance scheme (AMO) 92 for civil servants, workers, members of parliament, pensioners and their dependants, managed by the CANAM; 93
-
a medical assistance scheme (RAMED), managed by the Agence nationale d'assistance médicale (National Medical Assistance Agency, ANAM), 94 for the poorest people and other entitled beneficiaries;
-
at the same time, the national strategy for the development of mutuals adopted in 2011 was intended to promote the extension of a régime d’assurance-maladie volontaire (voluntary health insurance scheme, AMV) to the population of the informal and agricultural sectors.
Analyses carried out from 2012 onwards, as part of the development of national policies and plans, highlighted a number of difficulties encountered in particular by AMO. The latter was faced with considerable reluctance by workers in the formal sector, owing to their mistrust of the CANAM's management ability, its lack of communication with potential beneficiaries and the poor quality of services provided in public health facilities under agreement. At the end of 2012, AMO covered only around 30 per cent of its target population. In 2013, the RAMED covered only 0.2 per cent of its target population, mainly due to poor coordination between the ANAM and the decentralized bodies responsible for the poorest people. The number of mutuals increased significantly with the implementation of the 2011 development strategy, but the penetration rate only rose from 3.7 per cent of the national population in 2011 to 4.47 per cent in 2014, far below the expected results (Louis dit Guérin, 2014). These analyses have further highlighted the fragmentation of this scheme, a lack of complementarity or consistency between the various schemes, and a disparity in services covered, as well as with the different free programmes (pregnant women, children, and so on).
Based on these findings, the Ministry of Solidarity and Humanitarian Action launched a process to reform the system in 2015. This process was led by a task force to monitor the operationalization of universal health coverage in Mali, 95 with a group of experts in charge of leading the work and producing the instruments needed for the introduction of universal health coverage in 2018 and its operationalization by 2019. Various studies and consultations have been undertaken to define the care package for universal coverage, draw up a financing strategy and identify the AMU architecture. These led to the adoption of Law No. 2018-074 establishing the Régime d’assurance-maladie universel (Universal Health Insurance Scheme, RAMU) by the National Assembly on 13 December 2018 and its promulgation on 31 December 2018 (Diarra, 2021).
In 2022, the RAMU had yet to come into operation and the national SHP system was still the system put in place from the 2000s with AMO, the RAMED and mutuals. Below is therefore a description of the RAMU scheme pending its coming into operation.
12.1 The national social healthcare protection system
Governance
The reform of the national SHP system begun in 2015 aims to bring together the schemes set up in the 2000s, in order to offer the entire Malian population a single health insurance scheme that will cover all social categories through more appropriate mechanisms.
To achieve this objective, the reform entrusts the management of the RAMU to the CANAM, building on its experience in managing a public health insurance scheme and reorganizing it to extend its remit to cover people in the agricultural and informal sectors, who will be able to join through social mutuals, and to RAMED beneficiaries. Under the new plan, the CANAM will delegate some of its responsibilities to DMOs:
-
The Institut national de prévoyance sociale (National Institute of Social Security, INPS) for salaried employees. It should be noted here that the Malian government has introduced voluntary insurance under certain social security schemes managed by the INPS 96 for self-employed members of the liberal professions, craft trades, commerce and industry. These people can take out insurance under schemes managed by the INPS, including family benefits, old age, disability and death insurance and compulsory health insurance.
-
The Caisse malienne de sécurité sociale (Malian Social Security Fund, CMSS) for civil servants and similar employees.
-
Mutual insurance, through a contract with the Union technique de la mutualité malienne (Mutual Societies Technical Union of Mali, UTM) or other mutual insurance umbrella organizations, for the agricultural and informal sectors as well as RAMED beneficiaries.
Population coverage
The target set for the RAMU in the Health and Social Development Plan (PDDSS) 2014–2023 is to cover 45 per cent of Mali's entire population by 2023. The following table shows that coverage is progressing, but is still a long way from this target. It should also be noted that these figures relate to the populations registered in the various schemes and enrolled in the RAMU from 2018. These figures do not reflect the number of individuals actually insured and covered by the RAMU, as not all of them are necessarily up to date with their contributions.
Population coverage
|
2012 (1) |
2015 (2) |
2018 (3) |
2021 (4) |
|
|
Total population |
15.98 |
17.44 |
19.08 |
21.11 |
|
AMO |
557 082 |
721 394 |
||
|
Social mutuals |
375 496 (a) |
490 000 (b) |
||
|
RAMED |
1 526 |
40 636 (c) |
||
|
Population covered |
934 104 |
1 252 030 |
2 200 000 |
5 911 360 (d) |
|
Coverage rate |
5.8% |
7.2% |
11.5% |
28.0% |
Notes: (a) in 2010; (b) estimate based on the number of beneficiaries at the end of 2014 and in 2016; (c) in 2015, 153,942 beneficiaries of the social safety net programme were also in the process of registering with RAMED; (d) this figure includes private insurance companies.
Sources: (1) Louis dit Guerin, 2014; (2) Louis dit Guerin, 2018; (3) Ministry of Solidarity and Humanitarian Action, 2018; (4) Ouédraogo, 2022.
Healthcare package
The framework for the healthcare package covered by the RAMU is set out in Law No. 2018-074.
-
Article 17: The universal health insurance scheme entitles beneficiaries to direct payment of the costs of curative and preventative medical care and rehabilitation required due to their state of health or maternity. The conditions and procedures for direct payment of healthcare costs are determined by decree issued by the Council of Ministers.
-
Article 21: Under the universal health insurance scheme, part of the cost of healthcare is paid directly by the management organization, while the other part is paid by the insured person. However, the RAMU entitles people eligible for the medical assistance scheme to have all healthcare costs covered.
The basic scheme offered by the RAMU has not yet come into operation. The plan is to bring it into line with the AMO scheme, with coverage of medicines limited to generic and essential drugs only. The services currently covered by the AMO include preventative and curative care: general medical procedures and medical and surgical specialities; pregnancy, childbirth and postnatal care; hospital care and surgical interventions; medical biological tests; radiology and medical imaging; and medicines. Various services such as cosmetic surgery, spectacles, dental prostheses and all other services not covered by the nomenclature of medical treatments and medicines drawn up by the ministers responsible for health and social protection are excluded.
AMO benefits are available only from a network of healthcare providers approved by the CANAM, including public, community and private healthcare facilities; medical analysis laboratories; nurses, midwives and other paramedical specialists; dentists; private doctors and pharmacies.
These services are covered by third-party payment, with a reimbursement rate of:
-
80 per cent of the cost of care in the event of hospitalization (all care provided while the beneficiary is in hospital);
-
70 per cent of the cost of outpatient treatment (all treatment provided outside of hospitalization); and
-
the rate of reimbursement remains at 100 per cent for people eligible for the RAMED, as well as for services covered by current free-of-charge programmes (caesarean sections and children from birth to five years of age) and the various category-based mechanisms or those linked to the treatment of certain pathologies that will be managed by the RAMU.
Financing
The RAMU combines:
-
A contributory scheme with contributions based on the salaries of civil servants and military personnel, workers' wages and the allowance of members of parliament. These contributions as a percentage of income subject to contributions are currently set in AMO at:
-
4.48 per cent paid by the State or local authority as employer;
-
3.06 per cent payable by working salaried employees and 3.50 payable by private-sector employers;
-
0.75 per cent payable by pensioners.
-
-
A semi-contributory scheme for people in the informal and agricultural sectors who join the RAMU through mutuals and whose contributions are 50 per cent covered by the State. An actuarial study carried out in 2016 estimated the contribution at 6,600 CFA francs per year per beneficiary (Letourmy, 2014).
-
A non-contributory scheme for people currently eligible for the RAMED. This scheme is financed 65 per cent by the State budget and 35 per cent by local authorities.
According to health financing policy forecasts, the State will have to disburse a subsidy of 83 billion CFA francs by 2023 to achieve the target of 45 per cent of the total population covered, in order to co-finance contributions from the informal economy and finance coverage for the poor (Ouattara and Ndiaye, 2017).
12.2 Mutuals
Mutuals have experienced a major boom in Mali since the 1990s, with a number of important milestones:
-
The adoption of Law No. 96-022 of 21 February 1996 governing mutual societies in the Republic of Mali and its implementing regulations: Decree No. 96-136/PRM of 2 May 1996 laying down the conditions for investing and depositing mutual society funds; Decree No. 96-137/PRM of 2 May 1996 establishing standards for mutuals and mutual unions and federations; and Interministerial Order No. 97-MSSPA/MATTS-SG of 2 April 1997 setting out the procedures for approving mutuals.
-
The creation of the UTM in 1998 as part of a Mali-France agreement on mutual health insurance. The UTM is an umbrella organization with a dual mission:
-
Technical, through the promotion of rural and urban mutuals.
-
As an umbrella organization playing an intermediary role. The UTM is involved in discussions with the government and donors on the introduction of national health insurance schemes.
-
-
The Stratégie nationale d'extension de la couverture maladie par les mutuelles aux secteurs informel et rural 2011–2015 (National Strategy for the Extension of Health Coverage by Mutuals to the Informal and Rural Sectors, SNEM), adopted in 2011, was aimed in particular at promoting mutuals in the communes, with a target of 351 by the end of a three-year pilot phase, as well as improving the quality of the services offered by mutuals and structuring the movement at national level. The SNEM has also introduced the co-financing of 50 per cent of mutual members' contributions by the State.
-
The creation of the Agence malienne de la mutualité sociale (Malian Social Mutual Society Agency, AMAMUS) 97 in 2019, in accordance with Directive No. 07/2009/CM/UEMOA of 26 June 2009 on regulating social mutual schemes within the WAEMU. The AMAMUS is responsible for examining applications for approval and keeping the register of social mutuals and umbrella organizations. The AMAMUS is also involved in the promotion of mutuals and in communication and capacity-building activities for mutual society actors under the umbrella of the RAMU.
There are different types of social mutuals in Mali today:
-
community mutuals – in villages, health districts and, more recently, rural communes
-
inter-professional mutuals – in regional capitals and some secondary cities
-
national professional mutuals
The first two categories are directly involved in the roll-out of the RAMU (professional mutuals generally do not cover health and offer retirement or death benefits). Community mutuals and inter-professional mutuals are the result of the strategy developed by the UTM, with two approaches:
-
Voluntary health insurance (AMV) in urban and semi-urban areas: in 2000, the UTM launched a single healthcare product for its member inter-professional mutuals operating in urban areas (notably in Bamako, Kayes and Sikasso) and targeting the informal sector. The technical management of this product is undertaken by the UTM, which registers beneficiaries, collects contributions and pays healthcare providers. The UTM negotiates agreements (which include quality criteria) directly with health service providers, health centres and hospitals. The role of mutuals is focused on enrolling beneficiaries, keeping members informed and participating in the evaluation of the health services covered by reporting back to the UTM information relating to the reception and care of beneficiaries in the health facilities covered by the agreements.
AMV covers 75 per cent of out-patient and in-patient treatment in community and public health facilities (community health centres, referral health centres, public hospitals and specialist facilities) and approved pharmacies, with a contribution of 575 CFA francs per month per beneficiary. A second guarantee extends cover to private healthcare providers and specialist services, at a premium ten times higher. Take-up of this product is especially low (Louis dit Guerin, 2018).
-
A rural approach aimed at a poorer population, with support for the promotion of communal mutual health insurance schemes, based on the SNEM concept and implemented by NGOs, local organizations or community health associations. These mutuals offer a range of services to their members, taking into account the specific realities of the target populations, with cover often limited to primary health care and 50 per cent of health expenses.
The number of mutuals is evolving gradually in a very uneven way across the country, rising from 143 mutuals in 2010 to 174 in 2014 and 197 in 2017, some 110 of which were members of the UTM, including 23 inter-professional mutuals. In 2019, there were more than 220 mutuals, covering an estimated 4 per cent of the population of Mali (Sissouma, 2019).
A 2016 Direction nationale de la protection sociale et de l’économie solidaire (National Directorate for Social Protection and the Solidarity Economy, DNPSES) database of 161 mutuals, including UTM member mutuals and other non-members, provides a profile of these mutuals.
Monitoring indicators for mutuals, 2016
|
Number of registered members |
112 284 |
|
Men |
69% |
|
Women |
31% |
|
Proportion of self-employed members |
73% |
|
Proportion of salaried members |
27% |
|
Number of registered beneficiaries |
307 154 |
|
Men |
87% |
|
Women |
13% |
|
Number of paid-up members |
59 422 |
|
Number of beneficiaries up to date with contributions |
140 323 |
|
Average annual contribution |
3,700 CFA francs/beneficiary |
|
Average monthly contribution |
300 CFA francs/beneficiary |
|
Expected contributions |
2 377 million CFA francs |
|
Amount of contributions actually received |
1 424 million CFA francs |
|
Average recovery rate |
60% |
|
Proportion of beneficiaries in receipt of benefits |
46% |
|
Average size of registered households |
2.7 people |
|
Average household size in receipt of benefits |
2.4 people |
Source: Calculations from the DNPSES database (Louis dit Guerin, 2018)
12.3 Delegation of management under the RAMU scheme
Legal framework
In July 2021, the National Transition Council adopted a bill amending Act No. 09-016 of 26 June 2009 creating the CANAM. This became the RAMU management body, with the capacity to delegate, under its supervision, certain powers to DMOs.
A management agreement 98 specifies, as required, the functions delegated to each DMO. It is accompanied by a contract of obligations and management protocols between the CANAM and the DMOs, which sets out in detail the duties and obligations of each party. In return for undertaking their obligations, the DMOs receive an administrative allocation to cover operating costs and a technical allocation to cover the payment of services.
The delegation of management has been tried by the CANAM, in partnership with the INPS and the CMSS, in the context of compulsory health insurance. With the RAMU, this delegation is to be extended to two new DMOs, the UTM and the ANAM.
The aim is to manage resources efficiently and use the experience acquired by each DMO in managing their target populations.
Target populations
Article 9 of Law No. 2018-074 renders any natural person resident in Mali and any public or private natural or legal person who employs at least one salaried worker within the meaning of the legislation in force subject to the scheme. Organizations managing public pension schemes and mutual benefit organizations are treated in the same way as employers subject to the universal health insurance scheme.
Each DMO is responsible for a specific target group in the RAMU:
-
The INPS and the CMSS for AMO in the formal sector, which covers working and retired civil servants, working and retired employees governed by the Labour Code, public and private-sector employers, working and retired members of parliament and their dependants, representing around 17 per cent of the national population.
-
Social mutuals for those working in the informal sector, in agriculture and in the organized liberal professions, in other words 78 per cent of the population.
-
The RAMED for the poorest people, beneficiaries of the social safety net programme, orphans, prisoners, disaster victims, the war-wounded, the homeless and other entitled beneficiaries, in other words 5 per cent of the national population.
-
Within this system, the remit of the mutual health insurance movement is especially important and ambitious, given that mutual health insurance organizations must cover 78 per cent of the Malian population in the informal sector and in rural areas, and even 83 per cent if they are also responsible for covering those eligible for the RAMED.
Delegated functions
The RAMU scheme divides functions between the CANAM and the DMOs. Under this scheme, the CANAM allocates funds to the DMOs to cover their expenditure on services and day-to-day management.
The CANAM is responsible for:
-
definition of the healthcare package
-
final enrolment of insured persons and beneficiaries. To this end, it deploys a computerized network of terminals and enrolment sites throughout the country to register, enrol and issue cards to policyholders
-
development of RAMU management guidelines and procedures
-
pooling resources and risks
-
contracting with healthcare providers
-
medical oversight
-
support, monitoring and oversight of DMOs
The functions delegated to DMOs, including mutuals, relate to
-
actions to promote the RAMU, for which the UTM provides communications and marketing support for mutuals
-
pre-registration of insured persons and members of their families within their target group
-
collecting contributions and transferring them to the CANAM
-
settlement of treatment forms and payment to approved service providers. The DMOs, including mutuals, receive a technical grant and are responsible for the initial checking of invoices from insured persons and reimbursement of healthcare providers
-
monitoring the implementation of agreements with healthcare providers
-
oversight of RAMU governance.
Distribution of functions under the agreement between the CANAM and DMOs
|
Functions |
Distribution |
|
|
CNAMU |
DMO |
|
|
Definition of the healthcare basket |
X |
|
|
Agreements |
X |
Monitoring implementation |
|
Education and promotion |
X |
|
|
Enrolment, membership and renewal |
X |
Pre-registration |
|
Contribution collection |
X |
|
|
Resource mobilization |
X |
|
|
Pooling of risks covered |
X |
|
|
payment of benefits |
X |
|
|
Healthcare services |
||
|
Follow-up and steering |
X |
X |
12.4 Impact and lessons learned
In 2022, the RAMU had yet to come into operation, but lessons can already be learned from the functions delegated to the INPS and the CMSS by the CANAM under AMO since 2009. A number of challenges have been observed concerning compliance with the obligations of the DMOs and the failure by the CANAM to implement the penalties provided for, particularly regarding:
-
-
repayment to the CANAM of all the contributions collected and compliance with repayment deadlines;
-
low involvement in the collection of policyholder files for registration (pre-registration);
-
providing the CANAM with proof of the amounts received by DMOs as part of their operating grants; and
-
failure to comply with CANAM directives on the processing of treatment forms, particularly with regard to checking that healthcare providers are complying with agreed tariffs.
-
The challenges to be met by the RAMU in terms of ownership of the process by stakeholders at all levels and technical management of the insurance are significant, especially as the number of DMOs will be increased alongside mutuals.
Mutuals pose another challenge. Under the RAMU, they will have to provide cover for people in the informal and agricultural sectors, in other words 78 per cent of the national population, or even 83 per cent with the coverage of people eligible for the RAMED. However, the deployment of mutuals throughout the country is still limited and unevenly distributed, especially in the current security context, and their coverage is poor.
For the UTM and mutuals, the RAMU is presented as an opportunity, in particular because the healthcare package, which should be close to that currently covered by AMO, is more extensive than the cover offered by mutuals. With more extensive cover that is partially subsidized by the State, membership of mutuals could therefore be more attractive.
However, solutions will have to be found to increase the rate of development of these mutuals and to strengthen their capacities. In addition, this approach raises the question of the multiplication of mutuals, particularly in rural areas. It can be seen from the other case studies that the trend in the countries observed is towards a reduction in the number of mutuals, given the difficulty, or even inability, of providing technical support, developing management capacities, and making viable and overseeing a large number of organizations scattered throughout the national territory. In the specific context of Mali, it is up to the UTM to ensure the promotion of these mutuals, which also raises the question of the technical union's capacity to achieve the objective of covering the country. Added to this is the issue of security. Finally, another lesson learned from the countries in the region is the low level of ownership of community mutuals by the target communities, especially when the initiative for the mutuals comes from outside the community.
References
Diarra M. 2021. "Régime de protection sociale au Mali : Des précisions sur les avancées dans le processus d'opérationnalisation du RAMU". Fasomali.com, 9 June 2021. https://fasomali.com/regime-de-protection-sociale-au-mali-des-precisions-sur-les-avancees-dans-le-processus-doperationnalisation-du-ramu/.
Letourmy A. 2014. "Développement d'un panier de soins de base au Mali". WHO and Ministry of Solidarity, Humanitarian Action and Reconstruction of the North.
Louis dit Guérin O. 2014. "Examiner et évaluer le potentiel des mutuelles de santé en Afrique de l’Ouest". Mali Review, UNHCR, September 2014.
— 2018. "Etude comparative sur la protection sociale au Mali, en Mauritanie et au Sénégal (draft), Programme de Coopération Sud-Sud pour les Pays d'Afrique dans le domaine du Dialogue Social". ILO Algiers, July 2018.
Ouattara O. and Ndiaye P. 2017. "Potentiel des mutuelles de santé à la mise en œuvre de la Couverture Maladie Universelle au Mali et au Sénégal". MASMUT, June 2017. https://bit.ly/3guBo0a.
Ouédraogo P. 2022. "MALI: RAMU now operational!" P4H, 25 January 2022. https://p4h.world/en/news/mali-ramu-now-operational/h.
Sissouma I. 2019. "La délégation de gestion dans le cadre du RAMU vue par la mutualité". PowerPoint presentation.
Other documents consulted:
Deville C., Hane F., Ridde V. and Touré L. 2018. "La Couverture universelle en santé au Sahel : la situation au Mali et au Sénégal en 2018". Ceped Working Paper No. 40, Ceped, October 2018.
Ridde V., Antwi A., Boidin B., Chemouni B., Hane F. and Touré L. 2021. "Les défis des mutuelles communautaires en Afrique de l’Ouest". In Vers une couverture sanitaire universelle en 2030? Editions science et bien commun, 2021.
Sorro M. 2015. "Implementation of the Couverture Maladie Universelle (CMU) in the context of the UEMOA Community Regulation of Mutuality". Dissertation for the Master 2 professionnel de Droit Gouvernance mutualiste, Université Versailles St-Quentin-en-Yvelines, 2015.
Traoré S. 2019. "Le régime d’assurance-maladie universelle au Mali et la délégation de gestion". PowerPoint presentation.
13. Morocco
13.1 Background
The introduction of health cover for all in Morocco is the result of a long process that began in the 1990s. In the 1993 Speech from the Throne, His Majesty King Hassan II announced the principles of basic health cover.
In 1995, the government approved an initial draft law introducing Assurance-maladie obligatoire (compulsory health insurance, AMO), but it was abandoned because it only covered around 16 per cent of the population, namely civil servants, private sector employees and pensioners, and excluded the poorest people. This draft law was subsequently taken up by an interministerial commission on medical coverage, emerging from social dialogue, and led to the adoption in 2002 of Law No. 65-00 establishing the Basic Medical Coverage Code (CMB), 99 which introduced two schemes:
-
AMO, based on the principle of contributions and risk pooling for the benefit of the solvent population, in other words, employees in the formal public and private sectors and self-employed workers. AMO came into force on 18 August 2005, and its management was entrusted with two health insurance funds: the Caisse nationale des organismes de prévoyance sociale (National Social Insurance Societies Fund, CNOPS) and the Caisse nationale de sécurité sociale (National Social Security Fund, CNSS).
-
The Régime d’assistance médicale (Medical Assistance Scheme, RAMED), based on the principles of social assistance and national solidarity for the benefit of the underprivileged population. The RAMED was tested in the Tadla-Azilal region in 2008 and then rolled out countrywide in 2012.
Law No. 65-00 also led to the creation of the Agence nationale de l’assurance-maladie (National Health Insurance Agency, ANAM) in 2005 as a public body with legal personality and financial autonomy. The main tasks of the ANAM are to regulate and supervise the AMO scheme, in particular the CNSS and CNOPS, to which AMO management is delegated. Since 2012, the ANAM has been managing the resources of the RAMED. It ensures overall compliance with the provisions of the law governing the Basic Medical Coverage Code.
Following the new Constitution promulgated in 2011, Article 31 of which affirms the "right to healthcare, social protection, medical cover and mutual solidarity or solidarity organized by the State", a process of medical coverage reform was launched by the Head of Government in October 2013 in order to extend basic medical coverage to categories of the population not yet covered. Discussions were held between 2013 and 2017 as part of this reform, leading to (CESE, 2018):
-
the selection of ANAM as the entity responsible for steering the evaluation and monitoring unit in December 2014;
-
the adoption in July 2015 of Law No. 116-12 100 on health insurance for students, with coverage managed by the CNOPS;
-
the review in March 2016 of the proposal to cover ascendants, which was initially intended to cover the parents of insured persons in the public sector. A draft bill (no. 63.16) amending and supplementing Law No. 65.00 has been submitted by the government since 2017 but is still awaiting adoption by parliament;
-
the adoption in June 2017 by parliament of Law No. 98-15 101 on the health coverage scheme for self-employed workers and self-employed persons in the liberal professions, known as the Assurance-maladie des indépendants (Health Insurance for the Self-Employed, AMI).
A draft revision of the CNOPS legal framework was launched in 2016 and resulted in the adoption of Decree-Law No. 2-18-781 creating the Caisse marocaine de l’assurance-maladie (Moroccan Health Insurance Fund, CMAM), 102 published on 11 October 2018. The CMAM is a public institution that replaces the CNOPS in its AMO mandate.
The reform begun in 2013 is being continued in the priority areas of the 2017–2021 Government Programme, with a major boost provided by King Mohammed VI's Speech from the Throne in 2020, announcing the extension of compulsory health insurance to 22 million additional beneficiaries (including 11 million self-employed workers and 11 million current RAMED beneficiaries, who should all switch to AMO) by the end of 2022. These were to be added to the 11.17 million beneficiaries already covered by AMO in 2020 (El Haïti, 2021). In 2021, Morocco adopted Framework Law No. 09.21 on social protection. 103 This extends AMO cover and the same rights and healthcare packages as private-sector workers to self-employed workers (shop owners, craft workers, farmers, the self-employed in the liberal professions and other self-employed business managers). This framework law marks the entry into force in December 2021 of Law No. 98-15 adopted in 2017.
13.2 The national social healthcare protection system
Architecture and governance
Following a process that began in the 1990s, basic medical coverage, introduced by Law No. 65-00 of 2002, is provided through a contributory and a non-contributory system comprising five schemes:
-
The contributory system
-
The scheme for private-sector employees and pensioners (AMO-private), managed by the CNSS, covers private-sector employees and pensioners and their dependants (spouses, children of the insured persons and dependant children with disabilities).
-
The scheme for public-sector employees and pensioners (AMO-public), managed by the CNOPS, covers public-sector employees and pensioners and their dependants (spouses, children of insured persons and dependent children with disabilities).
-
The (contributory) student scheme (AMO-student) managed by the CNOPS, for post-baccalaureate students in public/private establishments who are under 30 years of age at the time of enrolment and who are not covered by other basic medical insurance schemes. This scheme is contributory for students enrolled in higher education or vocational training establishments in the private sector as well as those enrolled in fee-paying courses offered by public higher education or vocational training establishments or by establishments under the authority of a ministerial department or under its supervision.
-
The self-employed and liberal professions scheme (AMO-TNS) for self-employed workers (travailleurs non salariés, TNS), managed by the CNSS. The roll-out of this scheme is based on the principle of gradual implementation, with target groups categorized and a timetable initially providing cover for shop owners, professionals and craft workers subject to the Contribution professionnelle unique (Single Professional Contribution, CPU) scheme, shop owners and craft workers keeping accounts, and certain professionals who are already organized and have representative bodies (pharmacists, healthcare providers, architects, lawyers, notaries, transport professionals, self-employed entrepreneurs, and so on). In a second phase, the other socio-professional categories will be integrated as and when they have professional representation and are organized, with defined technical management procedures (membership, collection, and so on).
-
The non-contributory system
-
The (non-contributory) student scheme (AMO-student): The contributions of students who are not covered by the contributory AMO-student scheme are paid by the Moroccan State in accordance with Law No. 116-12. These are students enrolled in public-sector higher education or vocational training establishments. However, Law No. 116-12 provides for the possibility of this scheme evolving into a contributory system in the future for all these students.
-
The Medical Assistance Scheme for the economically deprived (RAMED) is based on the principles of social assistance and national solidarity for the benefit of the underprivileged population. The RAMED is managed by the ANAM, in conjunction with the Ministry of Health, the Ministry of the Interior and the Ministry of the Economy and Finance.
-
In addition to non-contributory mechanisms, medical cover is also provided for former victims of serious human rights violations (between 1956 and 1989): since 2009, under a tripartite agreement with the CNOPS and the National Council for Human Rights (CNDH), the State has paid the cost of membership of the CNOPS, which provides cover identical to that of the AMO-public (AMO-CNDH). Similarly, some categories of the population, in particular imams and mosque preachers, auxiliary staff of the authorities and veterans and members of the People's Liberation Army, are covered by the State, which takes out contracts with private insurers for cover identical to that of the AMO-public.
-
In addition to basic medical coverage, some workers are still covered by mutual societies and individual or group insurance contracts. Article 114 of Law No. 65-00 of 2002 gave employers who had taken out policies with private insurance companies before the law came into force a renewable transitional period of five years in which to switch to AMO. This period was intended to allow the employers concerned and their insurers, in particular private and mutual insurance companies, to prepare properly for the changeover (Haddougui, 2017). However, the status quo still prevailed in 2020, and some 400,000 employees continued to be covered by private insurance companies, a situation resulting from a lack of clarity in implementing legislation and the reluctance of private companies. One way of resolving this stalemate is for the CNSS to delegate the management of AMO benefits to private insurers (La Vie éco, 2012; CESE, 2018).The basic medical coverage schemes are supervised by the ANAM, a public body with legal personality and financial autonomy. The ANAM was created in 2005 to ensure the proper application of Law No. 65-00 and the smooth operation of the basic medical coverage scheme. It is responsible for the regulation and technical supervision of AMO and the financial management of the RAMED.
Its main tasks are described below.
-
Ensuring that the operation of compulsory basic health insurance is in line with the State's health objectives.
-
Leading negotiations on the establishment of national agreements between AMO management organizations and healthcare providers and suppliers of medical goods and services.
-
Monitoring the overall balance between resources and expenditure for each compulsory basic health insurance scheme and proposing to the administration the measures needed to regulate the compulsory basic health insurance system and, in particular, the appropriate mechanisms for controlling the costs of compulsory basic health insurance and ensuring compliance therewith.
-
Providing technical support to management organizations in setting up a permanent system for assessing the care provided to beneficiaries of compulsory basic health insurance schemes.
-
Providing arbitration in the event of disputes between the various parties involved in health insurance.
-
Ensuring the standardization of management tools and documents relating to compulsory basic health insurance.
-
Keeping consolidated statistical information on compulsory basic health insurance based on the annual reports sent to it by each of the management organizations.
-
Making the different reference systems available to management organizations, particularly concerning the identification of healthcare professionals in the private and public sectors, healthcare products and services, the nomenclature of procedures, and so on (ANAM, 2021).
Population coverage and healthcare packages
Through these various measures, Morocco's objective is to gradually achieve universal coverage. Such coverage has improved significantly with the implementation of the Basic Medical Coverage Code and continues to expand gradually, but 30 per cent of the population remained excluded in 2021. These are mainly people working in the informal sector, the self-employed and those in the liberal professions, as well as their dependants, who are not identified as poor or vulnerable according to the methodology established by the RAMED. Similarly, older people are not covered if they have not worked in the formal sector for the number of days required to receive their pensions (UNICEF, 2018).
Basic Medical Coverage Code coverage (as a percentage of the national population)
|
2005 (1) |
2014 (2) |
2018 (3) |
2021 (4) |
|
|
AMO |
28.8% |
31.0% |
||
|
RAMED |
31.0% |
30.6% |
||
|
Specific schemes |
9% |
8.4% |
||
|
Population covered |
16% |
60% |
69% |
70% |
Sources: (1) Haddougui, 2017; (2) ACAPS, 2019; (3) Cour des Comptes, 2022; (4) Ortiz, 2021
AMO beneficiaries have access to treatment in public facilities and in private facilities under agreement, but the parameters differ between AMO-public and AMO-private. In both cases, beneficiaries must pay the costs in advance and then claim reimbursement from their health insurance fund (one claim per month; each claim must be made within two months of the first day of treatment to be valid). Serious cases are covered by third-party payment by means of a prior request to the health insurance funds via the healthcare providers.
AMO healthcare package and reimbursement rates
|
Healthcare package |
AMO-private |
AMO-public |
|
Group I: Outpatient general medical, specialist medical and surgical, paramedical, functional rehabilitation and physiotherapy procedures, excluding medications. |
70% of the national benchmark tariff (TNR) |
80% of the national benchmark tariff (TNR) |
|
Group II: Care related to hospitalization and surgical procedures, including reconstructive surgery and blood and labile blood derivatives. |
70% of the TNR. 90% of the TNR when hospitalization is provided in a public hospital |
90% of the TNR. This rate is increased to 100% when services are provided in public hospitals, public health facilities and state health services. |
|
Group III: Medicines eligible for reimbursement. |
70% of the reimbursement base price |
70% of the reimbursement base price |
|
Group IV: Medical eyewear, medical devices and implants required for medical and surgical procedures. |
70% of the TNR |
Lump-sum fixed payments in the TNR |
|
Group V: Medical prosthetic and orthotic appliances eligible for reimbursement. |
70% of the TNR |
Lump-sum fixed payments in the TNR |
|
Group VI: Oral and dental care. |
70% of the TNR |
80% of the TNR |
|
Group VII: Medically required orthodontics for children. |
70% of the TNR |
Lump-sum fixed payments in the TNR |
Source: Moudhi, 2018
The RAMED provides basic medical coverage identical to AMO, but based on free care and services that are medically available only in public hospitals, health centres and state health services. Coverage is conditional on compliance with the care pathway, which must begin at the local health centre and may end at the hospital.
Financing of the Basic Medical Coverage Code
AMO is a contributory scheme based on contributions from workers and employers and a subsidy from the State:
-
AMO-private: The contribution rate for working employees is 5.5 per cent, 2 per cent of which is paid by the insured person and 3.5 per cent by the employer. The contribution rate for pensioners is 4 per cent (payable by the insured person).
-
AMO-public: The contribution rate for working people is 5 per cent of remuneration, 2.5 per cent of which is payable by the employer and 2.5 per cent by the employee, subject to a minimum monthly amount of 70 Moroccan dirhams and a maximum monthly amount of 400 Moroccan dirhams, which apply to both employees and employers. For pensioners, the rate is 2.5 per cent of the total amount of basic pensions, again subject to a monthly minimum of 70 Moroccan dirhams and a monthly maximum of 400 Moroccan dirhams.
The RAMED is funded by the State and local authority budgets. It is fully covered for persons living in poverty. 104 However, a partial annual contribution for vulnerable beneficiaries 105 is set at 120 Moroccan dirhams per person per year, subject to a ceiling of 600 Moroccan dirhams per household, regardless of the number of people in the household (www.ramed.ma).
13.2 Mutuals
The mutual insurance sector is governed by the provisions of Dahir No. 1-57-187 of 12 November 1963 on the status of mutual insurance. 106 There are currently 28 mutual societies set up for the benefit of employees in the public (11 mutuals), semi-public (7 mutuals) and private (5 mutuals) sectors, as well as the self-employed (5 mutuals). These mutual societies had 1.3 million members and a population of 3 million beneficiaries (around 8.2 per cent of the national population) at the end of 2018 (ACAPS, 2019).
These mutuals offer a range of services for their members and their families, including: basic medical coverage (under the AMO-public scheme) or complementary cover, as well as cover against the risks of death, old age, disability and accidents. Mutual societies may also offer aid, assistance and advances on sickness benefits and manage social welfare services, particularly of a health nature, for the benefit of their members.
The CNOPS, which is responsible for AMO-public, is itself closely linked to the mutual insurance sector. It is in fact a union of eight public-sector mutuals:
-
Mutuelle de la Police (Mutual Society for the Police, M. Police)
-
Oeuvres de Mutualité des Fonctionnaires et Agents au Maroc (Mutual Societies for Civil Servants and Employees in Morocco, OMFAM)
-
Mutuelles Générale des Postes et Télécommunications (General Mutuals for the Post Office and Telecommunitions, MGPTT)
-
Mutuelle des Forces Auxiliaires (Mutual for the Auxiliary Forces, MFA)
-
Mutuelle des Douanes (Mutual for the Customs Service, M. Customs)
-
Mutuelle Générale du Personnel des Administrations Publiques du Maroc (General Mutual of Public Administration Personnel, MGPAP)
-
Mutuelle Générale de l'Education Nationale (General Mutual for the National Education Service, MGEN)
-
Mutuelle du Personnel de l'Office d'Exploitation des Ports (Mutual for Port Service Personnel, MODEP)
The CNOPS, as the Fédération des Sociétés Mutualistes Du Secteur Public (Federation of Public-Sector Mutual Societies) was created in 1950 (CNOPS, 2009). Dahir No. 1-57-187, which currently governs public-sector mutuals, also applies to the CNOPS insofar as its provisions do not conflict with the terms of Law No. 65-00 establishing compulsory health insurance. Under this law, the CNOPS and its mutuals manage AMO for working and retired public-sector employees.
Alongside mutual societies, community mutuals are developing in several provinces, on a geographical basis (at the level of one or more communes), in order to facilitate people's access to health services (essential medicines, free evacuations, and so on) in return for an annual contribution of between 150 and 200 Moroccan dirhams per household (Haddougui, 2017). These community mutuals do not operate within the AMO framework or the November 1963 Statute on Mutual Societies, but their statutes, when they declare them, fall within the framework of the law on associations. They operate mainly in rural areas or suburban neighbourhoods, generally with technical and financial support from external partners, in particular the WHO and UNICEF. These community mutuals are generally little known and poorly documented.
13.3 Delegation of management as part of AMO public
Legal framework
The management of AMO for employees and retirees in the public sector (State, local authorities and public establishments) was entrusted to the CNOPS by Law No. 65-00 establishing basic medical coverage. Since 2015, it has also been responsible for managing AMO for students. The CNOPS and its member mutuals share tasks on the basis of a multi-year delegated management agreement 107 signed in 2006 and renewed in 2010:
-
The CNOPS collects contributions and provides overall cover for AMO-public and AMO-student. It directly manages high-risk files (hospitalization and long-term conditions as well as prior agreements).
-
Mutuals handle outpatient care files on behalf of the basic scheme, in return for a management fee. They also provide complementary cover and social welfare services.
From 2014, Law No. 120-13 108 amending and supplementing Law No. 65-00 authorized the CNOPS to enter into management delegation agreements with mutual societies other than the eight mutuals under the CNOPS. As such, and in implementation of the provisions of article 114 of Law No. 65-00, the CNOPS signed a management delegation agreement with the Mutuelle de la Prévoyance Sociale des Cheminots (Railway Workers’ Social Insurance Mutual) in 2018.
These agreements specify the organizational, administrative and financial management procedures, as well as the deployment of local services and the quality of services provided to insured persons.
Delegated functions
As the AMO management organization for working and retired public-sector employees, as well as for AMO-CNDH and AMO-student, the CNOPS performs a number of strategic and operational functions:
-
Preparation and adoption of national agreements with healthcare providers
-
Preparation of AMO management accounts
-
Processing of employer enrolment, registration, membership and updating of the administrative situation of insured persons
-
Collection of employee and employer contributions
-
Processing of claims for hospital treatment in Morocco and abroad
-
Reimbursement or direct payment of benefits covered by Law No. 65-00
-
Medical checks in coordination with the mutual societies concerned
The CNOPS member mutuals are responsible for receiving, processing, checking and settling claims relating to outpatient care. Once checked and authorized, the files are submitted to the CNOPS for transfer or payment to the insured person (CNOPS, 2009).
Mutuals also provide complementary cover: 20 per cent of the tarif nationale de référence (national benchmark tariff, TNR) for outpatient care and 16 per cent for reimbursable medicines. They also run welfare schemes for their members and provide certain additional benefits, such as death grants, retirement grants, schooling for children with disabilities, and so on. Like the Mutuelle générale du personnel des administrations publiques du Maroc, these mutuals can manage mutual health facilities offering a range of high-quality medical, clinical and paraclinical services to mutual members and their dependants, at an affordable cost.
Distribution of functions
|
Functions |
Distribution |
||
|
Status |
CNOPS |
Mutual insurance |
|
|
Definition of the healthcare package |
X |
||
|
Agreements |
X |
||
|
Education and promotion |
X |
X |
|
|
Enrolment, membership and renewal |
X |
||
|
Contribution collection |
X |
||
|
Pooling of risks covered |
X |
X |
|
|
Medical checks |
X |
X |
|
|
Payment of benefits |
X |
||
|
Healthcare services |
X |
||
|
Follow-up and steering |
X |
X |
|
13.4 Impact and lessons learned
Overall, the contributory system within the Basic Medical Coverage Code is characterized by a fragmentation of schemes and disparate parameters, resulting in a lack of solidarity and risk pooling between the different categories of population covered. As a result, the national system is not yet in line with the principle of solidarity, mutualization and unification, affirmed by Law NO. 65-00 on basic medical coverage (MEFRA, 2019). This fragmentation is compounded by difficulties in setting up the self-employed scheme, a high frequency of insurance-related risks (over-consumption, over-prescribing, extensive use of specialist doctors, and so on) and governance-related shortcomings (lack of an integrated information system, regulation, and so on) (Sninate and Bennana, 2017). In addition, the healthcare package has seen very little updating since the advent of AMO in 2005, with the result that the national benchmark tariff has become outdated. According to the 2018 report by the Cour des Comptes (National Audit Office), the impact of this failure to update has only increased the out-of-pocket expenses of insured persons, reaching 35 per cent in 2016 against 28 per cent in 2010. When non-reimbursable AMO treatments are added, policyholder contributions reach the same level as direct household costs in Morocco, which are close to 51 per cent (Cour des Comptes, 2018). Relations between the CNOPS and the mutuals under the delegated management mechanism within AMO-public do not appear to be problematic overall, apart from a conflict with the Mutuelle générale du personnel des administrations publiques du Maroc during the deployment of the "Esquif" information system in the CNOPS in 2016 (Zerrour, 2016). On the other hand, several failings at the CNOPS have been highlighted by the Economic, Social and Environmental Council and the Cour des Comptes:
-
The CNOPS legal framework is divided between three laws: Dahir No. 157.187 of 12 November 1963 on the status of mutual societies, Law No. 65-00 on the Basic Medical Coverage Code and its implementing decrees, which govern compulsory coverage for civil servants, public-sector pensioners and students, and Law No. 116.12 on the compulsory basic health insurance scheme for students.
-
Under the laws governing the establishment of budgets for the compulsory basic health insurance schemes managed by the CNOPS, each scheme must have a separate budget. These are as follows:
-
Budget relating to the AMO-public scheme provided for in article 90 of Law No. 65.00
-
Budget relating to the compulsory basic health insurance scheme for students provided for in article 20 of Law No. 116-12
-
However, neither of these budgets are available to the CNOPS, nor does it have its own budget consolidating all its investment and operating expenditure and clarifying the management costs associated with each scheme, as well as the criteria used to forecast and apportion common costs.
-
In its agreements with its member mutuals, the CNOPS has failed to comply with Law No. 65.00, article 44 of which prohibits organizations managing AMO from combining such management with "the management of facilities providing diagnostic, care or hospitalization services or facilities set up with a remit to supply medicines and medical materials, devices and equipment". Some CNOPS member mutuals have medical units and act as healthcare providers, including in the context of AMO, which makes them incompatible with Law No. 65.00. However, the mutuals concerned have found solutions to this problem by separating the management of AMO from that of the medical units and transferring the latter to new mutuals. These are dedicated to the creation and management of health and social welfare services under delegated management agreements with the parent mutuals.
-
In terms of administration and management, failings have been observed in governing body meetings. In 2018, the Cour des Comptes highlighted the impact of these failings on the approval of budgets (2017 and 2018) and accounts for the 2016 and 2017 financial years, as well as the approval of activity and financial reports for these two years.
-
Lastly, AMO-public's financial situation is fragile and deteriorating, due in particular to stagnating revenues, the growing number of pensioners within the insured population, the increasing prevalence of long-term or serious and costly illnesses, the growing rate of claims and, overall, continued rising expenditure. As a result, the fund recorded its first deficit in 2017, and actuarial projections carried out in 2018 by the Cour des Comptes concluded that far-reaching reforms of AMO-public were needed to curb a growing technical deficit and ensure the scheme's long-term future (Cour des Comptes, 2018).
The failings identified in implementing the provisions relating to the governance of the AMO-public scheme and the need to resolve the legal difficulties encountered by the CNOPS led the Ministry of Labour to initiate a reform of AMO-public. In this connection, the Head of Government’s Circular No. 6/18 of 30 March 2018 on establishing rules for the conduct and governance of the reform of the social protection system put in place the CMAM, the intention being that it would eventually take over the compulsory health insurance schemes managed by the CNOPS.
The CMAM is a public institution created in 2018 109 with a view to subjecting these schemes to the rules of good governance to which all public institutions are subject and establishing new base leadership to preserve achievements and make up for the lack of implementation of the provisions on AMO governance.
Decree-Law No. 2-18-781 authorizes the CMAM to delegate some of its tasks to public-sector mutuals and to any public or private legal entity, in line with the terms and conditions set out in an agreement approved by the governing body and based on a set of specifications on:
-
the nature of the benefits and the procedure for managing the reimbursement of guaranteed benefits;
-
reimbursement terms;
-
administrative and financial organization, geographical distribution, management costs and information and statistics relating to activities;
-
the methods for carrying out administrative checks and audits and the terms and conditions for accessing data;
-
the methods for carrying out medical checks;
-
the quality of services provided to insured persons;
-
the information system and arrangements for managing sickness file archives; and
-
administrative penalties in the event of failure to comply with the provisions of the agreements or the terms and conditions of the specifications.
The switch from the CNOPS to the CMAM is taking place gradually. By 2022, responsibility for the CNSS and the CMAM had transferred from the Ministry of Labour to the Ministry of Finance, which has embarked on a project to extend social protection to all Moroccans.
References
ACAPS (Autorité de Contrôle des Assurances et de la Prévoyance – Supervisory Authority of Insurance and Social Welfare). 2019. "Rapport d’activité 2019". ACAPS, 2022. https://www.acaps.ma/sites/default/files/publication_documents/2019_rapport_acaps_vf.pdf.
ANAM (Agence nationale de l’assurance-maladie). 2021. "Missions de l'ANAM", ANAM website, 2021. https://anam.ma/anam/lanam/missions-de-lanam/.
CESE (Commission des Affaires Sociales et de la Solidarité). 2018. "La protection sociale au Maroc, Revue, bilan et renforcement des systèmes de sécurité et d'assistance sociale, Rapport du Conseil Economique, Social et Environnemental, Auto-saisine 34/2018". CESE, 2018.
CNOPS (Caisse nationale des organismes de la prévoyance sociale). 2009. "Un passé riche d'avenir". CNOPS website, 2009.
Cour des Comptes. 2018. "Régime de l'assurance-maladie obligatoire gérée par la Caisse nationale des organismes de prévoyance sociale, Rapport annuel de la Cour des Comptes au titre de l'année 2018". Cour des Comptes, 2019. http://www.courdescomptes.ma/upload/_ftp/documents/17_R%C3%A9gime_AMO_CNOPS.pdf.
— 2018b. "L'Agence nationale de l'Assurance-maladie (ANAM), Rapport annuel de la Cour des Comptes au titre de l'année 2018". Cour des Comptes, 2019. http://www.courdescom ptes.ma/upload/_ftp/documents/15_ANAM.pdf.
— 2022. "Rapport annuel de la Cour des Comptes au titre des années 2019 et 2020" Cour des Comptes, Kingdom of Morocco, 2022. http://www.courdescomptes.ma/upload/MoDUle_20/File_20_836.pdf.
El Haïti H. 2021. "Assurance-maladie obligatoire: 11,17 millions de bénéficiaires en 2020, 22 millions supplémentaires en 2022". Le Matin, 13 December 2021. https://lematin.ma/express/2021/assurance-maladie-obligatoire-1117-millions-beneficiaires-2020-22-millions-supplementaires-2022/368937.html.
Haddougui D. 2017. "Couverture maladie de base (CMB): AMO", PowerPoint presentation, 20 July 2017.
La Vie éco. 2012. "Le basculement des assurés du privé vers l'AMO ne se fera pas de manière directe". https://www.lavieeco.com/ (blog). 9 July 2012. https://www.lavieeco.com/economie/le-basculement-des-assures-du-prive-vers-lamo-ne-se-fera-pas-de-maniere-directe-22710/.
MEFRA (Ministry of the Economy, Finance and Administration Reform). 2019. "Politique publique intégrée de protection sociale 2020-2030". UNICEF and EU, November 2019.
Mouhdi H. 2018. "L'apport d'un système d'information intégré à la couverture médicale de base, cas du Maroc". PhD thesis, Faculty of Medicine and Pharmacy, Mohammed V University, 2018.
Ortiz J. 2021. "Marruecos aumenta la tasa de cobertura médica a más del 70%". Atalayar, 15 December 2021. https://atalayar.com/fr/content/le-maroc-augmente-le-taux-de-couverture-m%C3%A9dicale-de-plus-de-70.
Sninate I. and Bennana A. 2017. "Les leviers de performance de l'Assurance-maladie obligatoire au Maroc". In Journal Marocain des Sciences Médicales 21(3). https://doi.org/10.48401/IMIST.PRSM/jmsm-v21i3.12521.
UNICEF (United Nations Children's Fund). 2018. "Mapping Morocco’s Social Protection System". Kingdom of Morocco, UNICEF, 2018. https://www.unicef.org/morocco/media/976/file/Mapping%20de%20la%20protection%
Zerrour L. 2016. "Blockage du système d'information / MGPAP-CNOPS : Le bras de fer !" Aujourd'hui le Maroc., 14 March 2016. https://aujourdhui.ma/societe/blocage-du-systeme-dinformation-mgpap-cnops-le-bras-de-fer.
14. Rwanda
14.1 Background
The first experience of prepayment for healthcare in Rwanda dates back to the 1960s, with mutual benefit societies such as Muwandimwe (Kibongo) and Umubano mubantu (Butare), followed in the 1980s by the introduction of health insurance systems managed by health centres (Rukoma Saké) or hospitals (Gikoré, Murunda, Kayove, and so on), which were essentially religious-based, for the benefit of the populations in their intervention areas. This experience, which achieved high coverage rates for the target populations, disappeared with the 1994 genocide. The years 1994–96 were a period of assistance, with the Rwandan government providing free public healthcare with the support of donors. With the reduction in this support, direct payment of healthcare costs was reintroduced in public facilities in 1996, leading to a decline in the use of healthcare services. This situation prompted the government to renew its interest in prepayment systems, and more specifically in mutuals; they are at the root of the national SHP system as it is known today, which has been developed in several key phases (Hitimana, 2022):
-
In 1999, the Ministry of Health, with technical support from USAID and the consulting firm Abt Associates, launched a pilot project for mutuals in three pilot districts (Byumba, Kabutare and Kabgayi). The project was gradually extended to the whole country, with strong incentives given by the State for local authorities to become actively involved in promoting mutual schemes, with the creation of such schemes in their provinces and districts becoming an element in the evaluation of these authorities by the Ministry of Local Administration (MINALOC).
-
In 2002, the Poverty Reduction Strategy Paper (PRSP), the guiding framework for policy and the fight against poverty, included the extension of mutuals as a national priority. More broadly, the PRSP emphasized the need to make social protection one of the pillars of its strategy, alongside investment in access to basic social services and wealth creation to ensure sustainable poverty reduction (Kamwenubusa et al., 2011). In 2004, mutuals were present in almost all of the country's provinces and covered around 2.1 million people, or 27 per cent of the national population.
This first wave of mutuals formed a heterogeneous group in terms of contributions (varying from 3,000 Rwandan francs (US$5.1 at the time) per average household of six people per year in rural areas to 11,500 Rwandan francs (US$19.5) in urban areas) and the coverage offered, which was essentially limited to primary health services. The Mutual Health Insurance Policy in Rwanda, 110 introduced in 2004, harmonized the organization of the mutual society movement and standardized coverage and contributions, which were set at 1,000 Rwandan francs (US$1.7) per person per year. However, this amount proved to be both too high for a large proportion of households (60 per cent of Rwanda's population lived below the poverty line in 2004) and too low for the viable financing of health insurance. The 2004 policy laid the foundation for subsidizing mutual health insurance by the formal sector, the State and external partners, to cover secondary-level care and include the poorest households. This subsidy policy was implemented 111 in 2006, along with risk pooling mechanisms at the district and national levels. In 2007, the country adopted Law No. 62/2007 of 30 December 2007 on the creation, organization, functioning and management of mutuals, which sets out the architecture and legal framework for mutuals. This law, which came into force in 2008, established community-based health insurance (CBHI). It also made membership of mutuals 112 and other schemes compulsory for the formal sector, stipulating that "all Rwandan residents must be affiliated to a health insurance scheme". From 2008 to 2010, mutual health insurance coverage continued to rise, from 74 per cent of the population in 2007 to 85 per cent in 2008, with 86 per cent in 2009 and 91 per cent in 2010 (Kalisa et al., 2015). This impressive increase in coverage is the result of a combination of different factors, including compulsory membership and the sometimes authoritarian practices of local officials in enforcing this obligation, as well as public and private subsidies and substantial funding by international aid donors, allowing contribution amounts to be reduced (Chemouni, 2018).
-
In 2009, the government carried out a functional analysis of CBHI with a view to improving it, leading to two important measures.
-
On the one hand, a national guarantee fund to provide financial support for community insurance was set up and financed by the Ministry of Health.
-
On the other, a new policy for the development of mutuals was developed in 2010. This introduces different levels of contributions based on the Ubudehe programme implemented by the ministry responsible for local authorities since 2001.
Between 2010 and 2015, the CBHI system entered a consolidation phase. However, several analyses carried out in 2014 showed that the system was dysfunctional management-wise, with high levels of fraud and a lack of technical capacity among local actors. In addition, the system was experiencing difficulties in maintaining its high level of coverage of the target population, with a negative trend before 2015 and the coverage rate varying from 90 to 76 per cent.
-
These difficulties led to the adoption of Law No. 03/2015 of 2 March 2015 governing the organization of the Community-Based Health Insurance Scheme, which transfers responsibility for CBHI from the Ministry of Health to the Rwanda Social Security Board (RSSB). In addition to improving insurance management, the law also aims to separate the functions of provider and purchaser and centralize insurance resources at the national level by moving from fragmented pools to a single pool. The 2015 law established CBHI in its current form, which, despite the use of the term "mutual health insurance scheme", is now a compulsory insurance system managed centrally by a public body that pools financial resources from domestic revenue, international aid and contributions from individuals. From 2015 to the present day, a number of measures have improved the system, including new sources of funding and the development of electronic management.
The term "mutual" is also retained by Law No. 48/2015 of 23 November 2015 governing the organization, functioning and management of health insurance schemes in Rwanda. This reaffirms the obligation for all Rwandans and foreigners resident in the country to join one of the national health insurance schemes.
To date, community involvement in CBHI has been limited to promotional efforts and financial contributions, making the system highly centralized rather than purely community-based. As a result, there are no delegated functions, as the government, through the RSSB, manages CBHI itself.
14.2 The national social health protection system
Architecture of the national system
The national SHP system currently comprises several schemes, each aimed at a specific population group. In addition to CBHI managed by the RSSB, the system includes the following schemes:
-
Health insurance for workers in the formal economy and their dependants is managed by the RSSB, which was created in 2010 113 by merging the two main social security institutions that were in place: the Rwandaise d'assurance-maladie (Rwandan Health Insurance, RAMA) and the Caisse sociale (Social Fund) or Social Security Fund of Rwanda (SSFR).
The RAMA was introduced through Law No. 24/2001 of 27 April 2001, initially for the benefit of civil servants, whose membership is automatic. The scheme is now also open to private-sector enterprises with at least seven employees. Retired members can join the scheme if they are in receipt of an RSSB pension and have already contributed to the scheme. Coverage is extended to members' spouses and children.
-
Military personnel are covered by a special scheme called Military Medical Insurance (MMI), created in 2005, 114 based on the same model as the RAMA, and administered by the Ministry of Defence.
|
Military Medical Insurance (MMI) |
RSSB Rwanda Social Security Board |
Medical Insurance Scheme of the National University of Rwanda |
Private insurance (SAHAM, RADIANT, UAP, MEDIPLAN, BRITAM, and so on) |
||
|
Health branch (RAMA) |
Community-based health insurance scheme (CBHI) |
||||
|
Regulation |
National Health Insurance Council |
||||
|
Guardianship |
Ministry of Defence (MINADE)/National Bank of Rwanda |
Ministry of the Economy and Finance (MINECOFIN)/National Bank of Rwanda |
National University/National Bank of Rwanda |
National Insurance Supervisory Commission/National Bank of Rwanda |
|
|
Legal coverage |
Military personnel Security service agents |
State officials and employees of the civil service, enterprises and private organizations |
Population not covered by the RSSB, MMI or private insurance |
Employees Students |
Employees of private companies |
|
Healthcare facilities covered |
Public health centres and hospitals, approved private providers and pharmacies |
Public health centres and hospitals, approved private providers and pharmacies |
Health centres and public hospitals |
Public health centres and hospitals, approved private providers and pharmacies |
Public health centres and hospitals, approved private providers and pharmacies |
|
Coverage rate |
85% |
85% |
Health centres: Lump-sum co-payment = 200 Rwandan francs Hospitals: 90% |
85% |
Varies depending on the insurance product |
|
Financing |
22.5% of gross salary (17.5% State; 5% insured person) |
15% of basic salary (7.5% employer; 7.5% worker) |
Annual contribution per person based on the Ubudehe categorization: Cat 1: 2000 Rwandan francs subsidized 100% by the State Cat 2: 3000 Rwandan francs Cat 3: 7000 Rwandan francs |
Employees: 15% of basic salary (7.5% employer; 7.5% worker) Students: 2.6% of grant awarded |
Varies depending on the insurance product |
-
Employees in the private sector may be members of the RAMA or are covered by their employers under insurance contracts with private insurance companies.
Health insurance schemes (in 2018)
Source: Louis dit Guérin, 2018
Population coverage
Article 3 of Law No. 48/2015 of 23 November 2015 states that "Any person, whether a Rwandan or a foreign national, who is on Rwandan territory shall be required to have health insurance. Any person entering the Rwandan territory without having any other form of insurance must subscribe to insurance with an insurance scheme of his/her choice within a period not exceeding thirty (30) days". It thus reiterates the compulsory nature of health insurance established under Law No. 62/2007, the implementation of which has sometimes been accompanied by authoritarian practices by local authorities, as highlighted above.
Coverage is now almost universal. The 13 per cent who are not insured (see table below) are covered by CBHI; according to the RSSB, the main reasons for this shortfall in the CBHI goal of 100 per cent target population coverage are as follows:
-
Self-employed workers and those in the liberal professions with high incomes who cannot be covered by the public schemes (RAMA and MMI) do not join because they feel that CBHI cover is too low (limited to public health facilities).
-
Young people who live alone are not interested in insurance because they are in good health.
-
Errors in the Ubudehe categorization mean that some households have to pay contributions that are too high in relation to their real income; these households do not join because they do not have sufficient contributory capacity (Louis dit Guérin, 2018).
Coverage rates for the various schemes
|
MMI |
RSSB Rwanda Social Security Board |
other |
Uninsured |
||
|
RAMA |
CBHI |
||||
|
Population covered (% of national population) |
0.2 |
4 |
82 |
1 |
13 |
Source: Uwaliraye and Hitimana, 2022
Community-based health insurance today
Following the process summarized above, CBHI has been managed administratively and financially by the RSSB since 1 July 2015. Although the term is still used, it no longer refers to mutuals but to a compulsory social insurance scheme covering the whole country, managed by a national fund and with contributions and benefits set by the State. The system is managed centrally by the RSSB. However, the fund has retained from the previous system a branch in each health facility, which receives and checks entitlement to benefits (the branches are connected to the RSSB information system) and guides insured persons. This branch also carries out an initial check of treatment invoices before forwarding them to the RSSB agencies in each district, where they are entered into the RSSB information system.
Membership
Article 11 of Law No. 48/2015 of 23 November 2015 governing the organization, functioning and management of health insurance schemes in Rwanda defines the CBHI target population as all Rwandans who have no other health insurance. This population includes the self-employed, workers and entrepreneurs in the informal economy and the agricultural sector, and their dependants. Contribution is individual, but membership for the whole household is compulsory.
One of the characteristics of CBHI in Rwanda is the simplicity of its procedures for policyholders, in particular membership, which involves payment of the annual contribution without any other administrative procedure. However, to join and contribute, the household must be categorized in the Ubudehe and members over the age of 16 must have a national identity card which serves as an insurance card (children under 16 receive an insurance card from the RSSB).
CBHI also covers specific groups such as prisoners, orphans in state care and some local authorities. These groups are registered in CBHI by the government, which provides 100 per cent of the funding for their contributions.
Healthcare package
CBHI covers all services and medicines provided in health centres (paquet minimum d’activités (minimum package of health services, PMA)), all services and procedures provided in district and provincial hospitals (paquet complémentaire d’activités (complementary package of health services, PCA)) and the full paquet tertiaire d’activités (tertiary package of health services, PTA) provided in national referral hospitals. Some health services are excluded from coverage, including medical certificates, mortuary fees, spectacles, dental prostheses, chemotherapy and dialysis for chronic cases (dialysis for acute cases is covered by CBHI, with a maximum treatment period of six weeks). Similarly, medicines and brands and specialist products sold in private pharmacies are not covered unless a hospital requests authorization from the RSSB, on the grounds that the products are needed and are not available in the healthcare facility’s pharmacy (Louis dit Guérin, 2018).
Health expenses are covered by third-party payment, with patients making a co-payment:
-
A lump sum of 200 Rwandan francs (US$0.2 in 2022) is paid by users at the RSSB branch in health centres and corresponds to a contribution to the administrative costs of the insurance.
-
Hospital expenses are 90 per cent covered by the CBHI scheme, with a 10 per cent user fee retained by the health facilities.
Financing
CBHI is funded from a variety of sources (see below).
-
State subsidies: Since February 2020, the government has created new CBHI subsidies through Prime Ministerial Order No. 034/01 of 13 January 2020. These subsidies are funded by various taxes and levies, including on salaries (0.5 per cent), gaming companies, parking fees, tourism revenues, and so on; expected to generate nearly US$3 per member annually.
-
Other health insurance schemes: the RSSB health branch (the RAMA) and private insurers pay the CBHI scheme a contribution equivalent to 10 per cent and 5 per cent, respectively, of the contributions they collect (Hitimana, 2022).
-
External partners (Global Fund, and so on).
-
Lump-sum co-payments by users of health centres and hospitals.
-
Annual contributions from households account for almost half CBHI resources. These contributions vary depending on the status of each household within the Ubudehe categorization. 115 Members are divided into three categories:
-
Contribution per person in category 1 (Category 1 of the Ubudehe) is fully funded by the State; cover is therefore free for these poorest households.
-
Contribution for category 2 (Ubudehe Categories 2 and 3) is 3,000 Rwandan francs (US$3) per person per year.
-
Contribution for category 3 (Ubudehe Category 4), which amounts to 7,000 Rwandan francs (US$6.6) per person per year.
-
The contribution for the third category corresponds to the actual amount of the contribution with no state subsidy. In other words, the State subsidizes the contributions of individuals in categories 1 and 2, who account for more than two thirds of CBHI members, by 7,000 Rwandan francs and 4,000 Rwandan francs, respectively.
The simplicity of the CBHI scheme is reflected in the mechanisms for contribution payments, which can be made either on the "Irembo" online platform 116 or at a branch of the Umurenge Savings and Credit Cooperatives (Umurenge SACCOs), or through an agent of the MobiCash mobile banking platform. As contributions can be paid in several instalments, each household can check its contribution account at any time by sending an SMS to the RSSB database to see what it has paid and what it still needs to pay to complete the total contributions for the household. When an insured person has paid all the contributions due for their household, they receive an SMS from RSSB informing them that their entitlement to benefits is available.
14.3 Decentralization of functions in the scheme before 2015
As already pointed out, CBHI is a highly centralized system today, managed by the RSSB and with no delegation of functions. Therefore, to look into a possible delegated management mechanism, you would have to turn to the system in place between 2006 and 2015, which divided management functions between different stakeholders at the national and decentralized levels.
Legal framework
Law No 62/2007 of 30/12/2007 on the creation, organization, functioning and management of mutual health insurance sets out the legal framework for mutuals in Rwanda, which until then had been governed by the codification of mutual societies in Rwanda dating back to colonial times through the decree of 15 April 1958 on mutual associations.
The 2007 law did not retain the management model proposed in the 2004 policy, which fully involved the community in the various levels of management of the system, including national institutions. Instead, the law greatly reduced the people’s role in the management of mutual resources, which was entrusted to public officials appointed by ministerial decree. The communities therefore found themselves confined to promoting insurance and paying contributions (Musango et al., 2009).
Administrative and financial organization and distribution of functions
With the 2007 law, the organizational structure of mutuals was modelled on the decentralized administration in the country's districts. Decentralized administrative entities include the City of Kigali, districts, sectors, cells and villages. Each district is an "autonomous" administrative entity, with the district mayor having broad administrative and management autonomy, although the various national authorities still have a significant presence.
CBHI organization was therefore based on a group of district mutuals and their mutual branches, coordinated at the national level by a technical support unit for mutual health insurance organizations.
-
District mutuals: A mutual has been set up in each of the country's 30 districts, with a legal status as a not-for-profit legal entity. Under the 2007 law, the role of the local population in the governance of district mutuals has been greatly reduced. They are now administered by a management committee composed of five members, including two persons elected by the mutual branch committees and three state officials appointed ex officio (the district health director, the deputy mayor responsible for district social affairs and the officer responsible for district mutual health insurance). Day-to-day management was the responsibility of the manager in charge of the mutual, who was a public official paid by the district from district funds or Pooling Risk funds and whose main role was to provide technical support to the branches of his/her mutual health insurance scheme, to sign agreements with district hospitals and to check invoices for healthcare provided from district hospitals. The management committee met at least once a month to approve the invoices received from the district hospitals and their payment, which was made by two other public officials (the district executive secretary and the district assets manager) who were joint signatories on the mutual's account, but were not members of the committee.
It was therefore not a mutual health insurance scheme in the usual sense of the term, but rather a national health insurance scheme with community participation. It should be noted, however, that management committees were not all established or in operation in all districts; where they were, administration of the mutual was conducted by the three public officials responsible for it.
-
Mutual branches: Each district mutual was subdivided into as many mutual branches as there were approved health centres in the district. Each branch was administered by a management committee whose members were elected by and from among the mutual’s members; the health centre chief was invited to the committee's monthly meetings but did not have the right to vote. The committee received the contributions collected by the cells, signed the agreements with the health centre and received, approved and forwarded the health centre's invoices to the district for payment. Day-to-day management was carried out by a manager, paid by the branch (not a public official), who was responsible for registering members, collecting contributions and paying health centre invoices.
These branches had no clearly identified legal status. They were authorized to "exist" as branches, with the agreement of the mayor of each district, and were located within the health centre from where they targeted the population of the intervention area.
Mutual branches were supported by a mutual committee in each cell. This committee was composed of four members, all of whom were mutual members, and one of whom had to be a woman. It was involved in information and awareness-raising activities for memberships and renewals, registration of memberships and collection of contributions.
The cell committee chairpersons and the public officials responsible for social affairs formed a mutual society committee at the branch level, separate from the mutual committee, which was involved in awareness-raising activities and monitored the cell committees.
-
Cellule Technique d'Appui aux Mutuelles de Santé (Technical Support Unit for Mutual Health Insurance Organizations, CTAMS): District mutuals were coordinated by the CTAMS, which reported directly to the Ministry of Health. The CTAMS was responsible for supporting the development of mutuals by disseminating management tools and providing technical training. It also contributed to the development of strategies, the formulation of policies and the monitoring and evaluation of mutual society bodies. The unit worked in close collaboration with these bodies and with the district and provincial authorities. However, it had a small staff (just six people in 2008) funded by the Ministry of Health and external partners (mainly the Global Fund project).
Mutual health insurance scheme coverage included all the services and medicines offered by health centres (minimum package of health services – "PMA") and all hospital services and procedures (complementary package of health services – “PCA”), with the exception of cosmetic surgery (excluding accidents) and prostheses. From 2007 onwards, 90 per cent of healthcare expenditure for both the PMA and the PCA was covered by third-party payment. Funding for this cover was shared between annual household contributions and subsidies from the State and external partners. The total contribution was set by the Ministry of Health, as part of the Mutual Health Insurance Policy in Rwanda (2004), at 2,000 Rwandan francs (US$3.4 at the time) per person per year. This amount was broken down as follows.
-
A contribution of 1,000 Rwandan francs per person per year, paid by households and intended to cover the minimum package of health services in health centres and branch operating costs (managers' salaries, rental costs, electricity, travel, and so on). This contribution was collected by the branches, which kept 90 per cent of it and paid 10 per cent to the district mutual.
-
A subsidy of 1,000 Rwandan francs per person per year, financed by the State and external partners. This subsidy was divided between a Health Solidarity Fund at the district level (district risk pooling) and a Health Solidarity Fund at the national level (national risk pooling).
-
District risk pooling was financed by the 10 per cent paid by the branches, district contributions, contributions from the national pooling risk and subsidies from external partners. It financed the services provided to beneficiaries as part of hospitals' complementary package of health services, as well as the attendance fees paid to participants at management committee meetings and, in part, the salary of the mutual’s manager.
-
National risk pooling was financed by a contribution from the RAMA (health insurance for employees in the public and private sectors) and the MMI (health insurance for military personnel), state subsidies and contributions from external partners. This fund financed healthcare provided to beneficiaries by the country's referral hospitals and support for loss-making district mutuals (for reasons other than poor management of contributions).
Before implementation of the Ubudehe categorization system from 2010, local and national NGOs and associations were involved in financing the contributions of poor and vulnerable people, for the same amount and with the same distribution as the contributions of other households.
Distribution of functions
The concept of delegated management does not appear in the official texts or in the documents on the various phases in the development of the CBHI system in Rwanda. Like the experiences of Senegal and Ethiopia, which share an initial approach with Rwanda inspired by the same external partner, the system was based on a distribution of functions between stakeholders at the national level and the decentralized administrative entities; the terms "decentralization" and "separation" of functions are also used in some descriptions.
Distribution of functions in the CBHI system (before transfer of CBHI to the RSSB)
|
Functions |
Distribution |
||||||
|
cell |
section |
district |
CTAMS |
MISANTE |
|||
|
Definition of the healthcare package |
X |
||||||
|
Agreements |
X |
X |
X |
||||
|
Education and promotion |
X |
X |
X |
||||
|
Enrolment, membership and renewal |
X |
X |
|||||
|
Contribution collection |
X |
X |
|||||
|
Pooling of risks covered |
X |
X |
|||||
|
Payment of benefits |
X |
X |
|||||
|
Healthcare services |
|||||||
|
Follow-up and steering |
X |
X |
|||||
14.4 Impact and lessons learned
CBHI is considered to be one of the main factors that have contributed to raising living standards in Rwanda. The rate of health service use has risen from 0.3 contacts per person per year in 1999 to 1.56 in 2019 (Uwaliraye and Hitimana, 2022), and maternal and infant mortality rates have fallen by two thirds since 2000 (from 107 deaths per 1,000 live births in 2000 to 32 deaths in 2015) (Chemouni, 2018).
The success of CBHI in Rwanda, which now has the highest rate of health coverage in sub-Saharan Africa, cannot be linked to the role of mutuals or to a system of delegated management:
-
The progressive development of CBHI since the first pilot projects in 1999 has called into question the community approach. Although the initial approach was based on mutuals, the 2007 law greatly reduced the involvement of communities in the management of the system, which was entrusted to decentralized administrative bodies. The 2015 law finally erased this community aspect, arguing that the technical and financial management of an insurance system requires solid skills, which community initiatives cannot provide. In this respect, it should be emphasized that Rwanda has chosen its own evolutionary path, moving away from the pure CBHI model, based on voluntary enrolment and community management, which is nevertheless promoted by external partners. This evolution should be compared with the experiences of Ethiopia and Senegal, which started from the same point.
-
The system put in place from 2007 onwards was based on the decentralization of management functions, modelled on a decentralized administration, with no delegated management mechanisms or agreements with the CTAMS, which primarily played a support and coordination role. In contrast, the CBHI scheme now managed by the RSSB is based on fully centralized management.
References
Chemouni, B. 2018. "The political path to universal health coverage: Power, ideas and community-based health insurance in Rwanda". In World Development 106: 87-98. https://doi.org/10.1016/j.worlddev.2018.01.023.
Hitimana, R. 2022. "Universal health coverage in Rwanda – Contribution of community-based health insurance scheme". Presentation at the international conference “Social Health Protection: a path to fight against inequalities”, Niamey, May 2022.
Kalisa I. R., Musange S. F., Collins D., Saya U. and Kunda T. 2016. "The Development of Community-Based Health Insurance in Rwanda: Experiences and Lessons”. University of Rwanda College of Medicine and Health Sciences – School of Public Health, Kigali, Rwanda and Management Sciences for Health, Medford, MA, USA, March 2016. https://msh.org/wp-content/uploads/2016/04/the_development_of_cbhi_in_rwanda_experiences_and_lessons.pdf.
Kamwenubusa T., Nicobaharaye N, Niyonkuru D. and Munyandekwe O. 2011. "Étude comparative des systèmes de protection sociale au Rwanda et au Burundi". Wereldsolidariteit-Solidarité Mondiale (WSM), March 2021. https://www.issuelab.org/resources/19849/19849.pdf.
Louis dit Guérin O. 2018. "Rwanda, Explorer les options publiques d’assurance-maladie et de services de santé pour les réfugiés". UNHCR/ILO, August 2018.
Musango L., Doetinchem O. and Carrin G. 2009. "De la mutualisation du risque maladie à l'assurance-maladie universelle, Expérience du Rwanda". Discussion Paper No. 1. WHO, 2009.
Uwaliraye P. and Hitimana R. 2022. "Universal health coverage in Rwanda – Contribution of community-based health insurance scheme". Presentation at the international conference “Social Health Protection: a path to fight against inequalities”. Niamey, May 2022.
15. Senegal
15.1 Background
Implementation of the couverture maladie universelle (universal sickness coverage, CMU) scheme in Senegal began in 2013 with the drafting of the Stratégie nationale de développement économique et sociale 2013–2017 (National Strategy for Economic and Social Development 2013–2017, SNDES), which sets out the Government of Senegal's policy guidelines for extending social protection in general and health risk coverage in particular. This is accompanied by the Plan stratégique de développement de la couverture maladie 2013-2017 (Strategic Development Plan for Health Coverage 2013–2017, PSD-CMU) drawn up by the Ministry of Health and Social Action, at the instigation of the President of the Republic. The aim of the PSD-CMU is eventually to extend and group together the current health coverage schemes and programmes, with a view to achieving coverage of 75 per cent of the population by 2017. The PSD-CMU strategy is based on three main pillars:
-
Free healthcare for vulnerable groups (children, older persons, disabled persons, and so on).
-
The promotion of community mutuals, seen as the best way of extending basic health coverage to the rural and informal sectors.
-
Strengthening health insurance institutions for private-sector employees (PSD-CMU, 2013).
In 2013, the Senegalese government also formulated the Stratégie nationale de protection sociale 2013– 2017 (National Social Protection Strategy 2013–2017), which has been revised and updated to cover the period 2016–2035. This strategy includes CMU among its priorities, extending the target of population coverage to at least 80 per cent by 2025. This priority is also reiterated in the Plan national de développement sanitaire et social 2019–2028 (National Health and Social Development Plan 2019–2028, PNDSS), one aim of which is to accelerate progress towards UHC.
The CMU scheme is broadly in line with priority 2 on human capital, social protection and sustainable development of the Plan Sénégal Emergent (Emerging Senegal Plan, PSE), which is Senegal's economic and social development policy reference framework for the period 2014–23.
Implementation of the CMU scheme is overseen by the Ministry of Health and Social Action, and its operationalization has been entrusted to the Agence de la couverture maladie universelle (Universal Sickness Coverage Agency, ACMU), created in January 2015. 117 However, the CMU scheme is based on an older process that began in the early 2000s, with the adoption of Law No. 2003-14 on mutuals, which set out a legal framework for mutuals and, in 2004, the Plan stratégique de développement des mutuelles de santé (Strategic Development Plan for Mutuals). The latter was updated in 2008 with the drafting of the Stratégie nationale d’extension de la couverture du risque maladie des sénégalais (National Strategy for the Extension of Health Risk Coverage for Senegalese People), which lays the foundations for the CMU scheme, including regarding the development of mutuals. This development was to take place through the implementation of the "projet de démonstration de l’extension de l’assurance-maladie sur la base des mutuelles de santé dans le contexte de la décentralisation (demonstration project on the extension of health insurance based on mutuals in the context of decentralization)", better known by its acronym DECAM. With the PSD-CMU, the DECAM became "Décentralisation de l’assurance-maladie (Decentralization of Health Insurance)" and is at the heart of the current strategy for implementing CMU. The DECAM is based on a partnership between community mutuals, local authorities and the State to drive progress towards CMU, with a strategy that can be summed up in the project's slogan: "One local community, at least one mutual" (Deville et al., 2018).
In 2020, the Government of Senegal, through the Ministry of Community Development and Social and Territorial Equity, commissioned an evaluation of the CMU scheme for the period 2013–2019. The aim of this evaluation was to carry out an in-depth diagnosis of the programme with a view to significantly improving its effectiveness, efficiency, sustainability and social inclusion (Diagne and Sylla, 2021). The results of this evaluation, scheduled for release in early 2022, should feed into a process of CMU reform. This case study is based on the CMU situation prior to the development and implementation of these reforms.
15.2 The national social health protection system
Architecture and governance
Senegal's national SHP system combines a range of insurance, assistance and social action mechanisms aimed at different categories of the population, the addition of which should provide cover for all. However, coverage is fragmented and the various mechanisms are compartmentalized. They are each aimed at specific groups of the population, with no solidarity between them or offering a basic guarantee common to all:
-
Health coverage for civil servants is governed by Decree No. 72-215 of 7 March 1972 on social security for civil servants. Healthcare costs for civil servants are partially covered by the national budget; this is a form of State self-insurance. Civil servants and retired civil servants continue to benefit from this cover under the same terms and conditions and according to the same procedures as those in active employment.
-
Health coverage for employees in the formal sector is provided by a compulsory insurance scheme managed by the Institutions de prévoyance maladie (Health Insurance Institutions, IPM). 118 A total of 129 IPM were in operation in 2020 and have been supported since 2017 by the Institution de coordination de l'assurance-maladie obligatoire (Institution for the Coordination of Compulsory Health Insurance, ICAMO), under the technical supervision of the Ministry of Labour, Social Dialogue and Relations with Institutions. The ICAMO's objective is to support the strengthening of the management, functioning, governance and overall effectiveness and efficiency of the IPM.
-
The CMU scheme provides various forms of coverage for the rest of the population. The CMU scheme does not yet have a legal basis and currently operates using a programme approach. A draft law on the CMU scheme had been under consideration since 2017 and was intended to define the arrangements for implementing the CMU scheme's insurance and assistance systems. This bill has been abandoned in favour of integrating CMU into the new Social Security Code, which is was due to be adopted in 2022 and would lay the foundations for the construction of a general scheme for all Senegalese people (in other words, extended to the IPM and other schemes). This integration, combined with the process of reflection under way following the evaluation of the CMU scheme as outlined above, should provide a legal framework for the CMU scheme and redefine its organization and functioning, including the role of mutuals within the system.
CMU covers:
-
CBHI schemes, or community mutuals, designed mainly for rural areas and the informal sector;
-
free programmes for children aged under 5, pregnant women, the poorest people, persons with disabilities, persons on dialysis, and so on; and
-
the Plan Sésame, which guarantees access to healthcare for all people aged over 60.
The CMU scheme is managed by the ACMU, 119 which was set up in 2015 to "ensure the implementation of the national strategy for the development of universal sickness coverage". It is responsible for overseeing the CMU schemes, excluding those under the compulsory health insurance scheme for salaried workers, and for the technical supervision of the provident societies that make up these schemes. The ACMU promotes mutuals and other social mutuals as part of the extension of health insurance coverage to the informal sector and rural areas.
Under the DECAM, the ACMU mobilizes the funding needed to implement CMU and acts as a regulatory body, with the technical functions of managing memberships, collections and benefits provided by mutuals and their umbrella organizations.
Target populations and healthcare packages
The current national SHP system is based on a fragmented architecture and a wide range of schemes, including 676 community mutuals and 129 IPM, each aimed at specific groups. The table below summarizes the different schemes and their target groups. Under the CMU scheme, some services (for non-poor households, persons with disabilities, beneficiaries of the Programme national de bourses de sécurité familiale (National Family Social Security Grants Programme, PNBSF) are provided via mutuals, which receive state subsidies for this purpose and to which these beneficiaries are automatically enrolled as members. For other schemes (children from birth to age 5, pregnant women, older persons), healthcare providers invoice the ACMU directly, which acts as the purchaser.
Healthcare packages and target populations for social health protection schemes
|
Schemes |
Services |
Target population |
|
Formal-sector schemes |
||
|
Régime des fonctionnaires et Fonds national de Retraite (Civil servants' scheme and National Retirement Fund (FNR) |
80% of the cost of hospitalization, consultations, examinations and tests in public health facilities and some approved private facilities is covered. Medicines supplied outside of health facility pharmacies are not covered. |
State employees and civil servants, working and retired, and their dependants |
|
Social security Health insurance institutions (IPM) |
Each IPM covers part of the cost of medical treatment for non-occupational illnesses suffered by workers and their dependants, between 50% and 80%, in approved public and private health facilities. |
Private-sector employees and their dependants |
|
Social security Institution de Prévoyance Retraite du Sénégal (Social Insurance Institution for Old-Age Pensions in Senegal, IPRES) |
Although this was not part of its original remit, the IPRES covers 100% of the healthcare costs of its beneficiaries (pensioners and survivors) in its medical and social welfare facilities. Health expenses for patients referred to other health facilities are covered at 100% by the IPRES (with certain exclusions). |
IPRES pensioners and their dependants |
|
Complementary health insurance |
A complementary system that covers the portion of medical care and some pharmaceutical costs not reimbursed by the civil servants' scheme, or even the IPM. |
Employees in the formal sector |
|
Universal sickness coverage (CMU) scheme |
||
|
ACMU |
Free healthcare for children from birth to age 5 in public health facilities |
Children from birth to age 5 |
|
ACMU (Community mutuals) |
80% of healthcare costs covered, 50% for specialist drugs at public health centres |
Pupils and talibé children |
|
ACMU (Community mutuals) |
CBHI: 80% of healthcare costs covered at primary, secondary and tertiary levels; 50% for specialist drugs. Contribution of 7,000 CFA francs per year per beneficiary, 3,500 CFA francs of which is subsidized by the State. |
Non-poor informal and agricultural sector households |
|
ACMU |
Medical treatment in public health facilities are available free of charge to Plan Sésame beneficiaries: consultations, essential and generic medicines, additional tests, medical and surgical procedures and hospitalization. There are exclusions, but these are not observed). |
People aged 60 and over (excluding the IPRES and FNR) |
|
ACMU (Community mutuals) |
The State provides free services for people in need suffering from a duly recognized severe disability, in health facilities run by the State, local authorities and public bodies. The same services are provided at a reduced price in private health services. |
Persons with disabilities eligible for the Carte d’égalité des chances (Equal Opportunities Card, CEC) |
|
ACMU |
100% coverage of an operation, pre- and post-operative check-ups, a kit of medicines and consumables, a hospital stay not exceeding five (5) days, resuscitation products and medicines and associated check-up, in the country's public health facilities able to perform caesarean sections, namely hospitals, health centres, SONU (emergency obstetric and neonatal care), health centres with operating theatres and health facilities that provide emergency obstetric and neonatal care. |
Any Senegalese woman in pregnancy whose state of health or that of the foetus requires a caesarean section |
|
ACMU (Community mutuals) |
100% reimbursement by mutuals based on a state subsidy covering the contribution, membership fees and co-payment. |
Persons identified as vulnerable or in the poorest category who are in receipt of the PNBSF |
|
ACMU (Community mutuals) |
Coverage of haemodialysis sessions and haemodialysis kit or peritoneal dialysis kit in public facilities; sessions at reduced rates in private facilities under CMU agreement. |
Patients suffering from chronic renal failure |
|
Other |
||
|
“major" social mutuals |
Health coverage from the first franc. Contributions and benefits vary from one mutual to another. |
Informal and agricultural sectors |
|
University centres |
University centres cover students for day-to-day care (consultations, medicines, tests, dental care and hospitalization). |
Senegalese students |
Source: ILO, 2021
The level of population coverage varies depending on the method of calculation. According to the ACMU, 49 per cent of the population was covered by a health insurance scheme or system, including free health insurance initiatives and CBHI, by the end of 2018. A review of social protection carried out by the ILO and the Délégation générale à la protection sociale et à la solidarité nationale (National Office for Social Protection and National Solidarity, DGPSN) estimated the level of coverage at 38 per cent for the same year, counting only insured persons who were up to date with their contributions to mutuals.
This coverage has risen sharply, from an estimated 18 per cent in 2012, but remains below the targets set, in particular by the PSD-CMU 2013–2017, which aimed to reach 75 per cent of the population by 2017.
Financing of universal sickness coverage
Insurance schemes are financed by contributions from policyholders, with contributions ranging from 4 to 15 per cent of salary subject to contributions in the case of IPM, and varying amounts in the case of major mutuals. Community-based insurance is based on a contribution from policyholders (3,500 CFA francs per person per year), supplemented by a subsidy of an equal amount from the State.
Other CMU mechanisms are financed by the State. In 2020, it was estimated that less than 40 per cent of CMU beneficiaries paid their own contributions and 60 per cent received benefits without contributing to the financing of the system, which is heavily dependent on state funding (Ridde et al., 2022), the vagaries of which hamper the functioning of mutuals and their ability to offer continuous quality services.
According to ACMU data, subsidies paid to community mutuals (subsidies for contributions from traditional members, pupils, and PNBSF and CEC beneficiaries) rose from 558.6 million CFA francs in 2016 to 750.1 million CFA francs in 2017, then fell to 169.2 million CFA francs in 2018. In the latter year, the State accumulated significant delays in the payment of its subsidies, resulting in a cash flow crisis in many mutuals, forcing some to suspend their services for several months. The benefits provided by CMU mutuals are therefore precarious and not guaranteed, including for members who pay their share of the contribution (ILO, 2021).
15.3 Mutuals
The development of mutuals began in the 1960s, with the first mutuals set up within enterprises, public administrations and the army. Mutuals for the informal and agricultural sectors appeared in the 1990s, initially in the Thiès region. They gradually spread throughout the country with the support of national and international development organizations, and then expanded significantly with the establishment of the DECAM from 2012. As mentioned above, there are three main groups of mutuals today:
-
Mutuals in the formal sector, especially within public administrations, to complement the cover provided by the civil servants' scheme; these mutuals often also offer other types of services to their members.
-
The so-called "major" or "socio-professional" mutuals, which are aimed at specific target groups (workers in a particular sector of activity, members of a savings/credit network, and so on) within the informal economy and the rural sector. They operate outside the DECAM, so their membership fees are not subsidized by the State, although they are recognized and approved by the ACMU. The functioning and performance of these mutuals is poorly documented. Four major mutuals were listed in 2018 with an estimated coverage of 316,200 beneficiaries, equivalent to 23 per cent of the large group of beneficiaries covered by functional community mutuals in 2018. However, it is not possible to tell from the available data whether these are registered beneficiaries or actual contributors (ILO, 2021).
-
Community health mutuals promoted under the DECAM. The mutual societies developed under this national initiative are coordinated around three complementary levels:
-
at least one community mutual in each local authority (commune and rural community)
-
a departmental union of mutuals in each department
-
a regional union in each region
This architecture is complemented by the Union nationale des mutuelles de santé communautaires du Sénégal (National Union of Community Health Mutuals of Senegal, UNAMUSC) created in January 2014, with regional unions as members. The UNAMUSC's role, with the support of the State, is to support the roll-out of CMU, health promotion activities and partnerships between the unions, the State, technical and financial partners and local authorities.
Although it is a parastatal agency, the ACMU can be considered as the umbrella body for this architecture of DECAM's mutuals.
In 2018, there were 676 community mutuals spread across the country's 552 municipalities (Schwettman, 2022).
In 2017, only 55 per cent of mutuals were in operation (CARES, 2018). A recent evaluation shows an improvement, but there are still recurring weaknesses, particularly with regard to the qualifications of managers of community mutuals, the production of information and risk management (Diagne and Sylla, 2021).
-
Departmental health insurance units (UDAM). This approach was tested in the departments of Koungheul and Foundiougne, with support from Belgian technical cooperation (Enabel development agency) from 2013 to 2017. UDAM are departmental-level mutuals, approved by the Ministry of Health and Social Action – but not subsidized by the State – and managed by permanent salaried staff.
Membership of UDAM is either family or group-based, with a minimum of five beneficiaries per member. Membership fees vary according to the number of beneficiaries: for example, the annual fee is 2,500 CFA francs per person for a membership of between five and ten people, and 2,300 CFA francs for a membership of 11 or more people. A particular feature of UDAM is the contractual arrangement with the healthcare provider, based on a lump-sum fee. The UDAM healthcare package includes the public health outpost and health centre levels, with the level of coverage varying (75 per cent for an outpatient consultation and 80 per cent for childbirth and emergency care at the health outpost, over 90 per cent for care provided in the health centre) (Deville et al., 2018b).
15.4 An effective partnership between the ACMU and community mutuals rather than a formal system of delegation
The partnership system
The CMU scheme does not have a formal delegated management mechanism. The CMU, and more specifically the DECAM strategy, is based on "the establishment of an effective partnership between community mutuals, local authorities and the State to drive progress towards universal sickness coverage" (Deville et al., 2018).
This partnership is achieved:
-
first, by all mutuals, even though independent and self-managed, adopting the same healthcare package, the same insurance parameters and the tools developed by the DECAM;
-
second, through the government's policy of subsidizing contributions by 50 per cent (in other words, 3,500 CFA francs payable by the beneficiary and 3,500 CFA francs payable by the State) and 100 per cent for persons identified as being in the poorest category (households benefiting from the PNBSF programme and holders of the CEC card) and beneficiaries of free insurance programmes.
-
In addition, in order to support the professionalization of the DECAM scheme, the ACMU funds the staff of the technical management units set up at the departmental union level (two employees per department, financed for two years) as well as ”incentives” for the managers of the mutual. All mutuals participating in the DECAM are required to join the regional unions, which are themselves affiliated to the regional unions.
With regard to these last two points, the mutuals promoted by the DECAM are largely dependent on state funding, both in terms of contribution subsidies (partial or total) and for some of their operating costs, with all the risks of dysfunction observed in recent years when the State does not fulfil its obligations, or only partially.
Existing community mutuals wishing to join the DECAM scheme and those set up by the ACMU must comply with the terms set by the ACMU. This agreement does not prevent the creation of autonomous mutuals outside the DECAM scheme, but these do not benefit from subsidies or other support from the State, although they do receive approval.
Distribution of functions within the DECAM
At the ACMU level
-
The healthcare package is determined by the ACMU, which sets all the parameters (contributions, services covered, rates of reimbursement).
-
All the management tools for mutuals, as well as the model agreements with healthcare providers, are developed by the ACMU and used by the mutuals.
-
The ACMU conducts awareness-raising campaigns and supports mutuals so that they become more professional and trustworthy.
-
One of the ACMU's key missions is to mobilize resources to finance 50 per cent of contributions and to provide full coverage for beneficiaries of free healthcare policies.
-
The ACMU keeps the national register of mutuals, checking that they are properly set up and functioning, as well as their financial situation and solvency.
At the mutual and union level
-
Community mutuals and unions are responsible for raising awareness among the population and lobbying local authorities.
-
Community mutuals sign agreements with primary healthcare structures, based on the ACMU's standard agreement, which they can adapt to meet the specific needs of the health outposts and health centres in their commune or rural community. The regional unions support the introduction of framework agreements between the departmental unions and the hospitals in the department, to harmonize contractual practices with healthcare providers.
-
Departmental unions maintain contractual relations with the hospitals serving the department and manage services at the hospital level.
-
Community mutuals are responsible for registering and enrolling households in their intervention areas. They work with leaders of grassroots community organizations, neighbourhood and village chiefs, and local authority officials to identify the poorest people and vulnerable groups eligible for free healthcare services. They create membership books for insured contributors and those benefiting from assistance programmes.
-
Community mutuals collect household contributions directly (50 per cent of the total contribution).
-
The risks covered by the basic package are pooled at community mutual level. The risks covered by the complementary package are pooled at departmental and regional union level. Consequently, the cover offered is limited to the administrative areas where the mutuals and their unions are located. Beneficiaries are thus covered for primary healthcare in their mutual’s intervention area, which generally corresponds to a commune, and in the secondary and tertiary public structures in their department and region.
-
Community mutuals and departmental unions play a complementary role in the purchasing of healthcare.
-
Regional unions monitor the mutuals, reporting at least quarterly, and provide technical support to mutuals in difficulty. They also help to draw up an annual action plan for the development of mutuals. Furthermore, they act as social intermediaries between the departmental unions, regional and national hospitals, the regulatory body and other development actors at the regional level.
|
Functions |
Distribution |
|
|
ACMU |
Mutuals and unions |
|
|
Definition of the healthcare package |
X |
|
|
Agreements |
X |
|
|
Education and promotion |
X |
X |
|
Enrolment, membership and renewal |
X |
|
|
Leveraging government subsidies |
X |
|
|
Contribution collection |
X |
|
|
Pooling of risks covered |
X |
|
|
Payment of benefits |
X |
|
|
Healthcare services |
||
|
Follow-up and steering |
X |
X |
15.5 Impact and lessons learned
Overall, Senegal's national SHP system is fragmented, with a wide variety of IPM and community mutuals. With regard to the latter, the evaluation carried out in 2020 highlighted a number of achievements, including the roll-out of CMU throughout the country, but also a number of technical and financial weaknesses. The proliferation of community mutuals makes it difficult, if not impossible, to regulate and steer the system as a whole, and to provide sufficient technical support. As a result, only 55 per cent of community mutuals were actually in operation in 2017.
Senegal's decision to rely on the promotion of community mutuals, located in communes throughout the country, has ruled out the so-called major mutuals in the DECAM plan. However, these have shown that they can cover a large population (316,000 beneficiaries for just four major mutuals) with centralized management and local representation.
Furthermore, the high degree of fragmentation of health risk cover mechanisms in Senegal has led to limited solidarity, with obvious weaknesses in the redistribution of resources between mechanisms and between target populations (Diagne and Sylla, 2021).
On the specific question of the delegation of management, there are several possible ways of looking at the partnership mechanism that has been in place since 2010 under the DECAM. It can be likened to:
-
a system of delegated management currently under construction; the priority for the ACMU is initially to build a mutual network that operates throughout the country so that it can then formally delegate a range of functions. However, there is still a long way to go because although all municipalities now have at least one mutual, some of them, as already pointed out, are experiencing operating difficulties and are not offering quality services to their beneficiaries (CARES, 2018);
-
the deployment of a network of CMU branches in which the mutuals and unions have no autonomy and follow ACMU procedures. This reading of the system is not correct, however, as it would imply that the ACMU manages health insurance, whereas today it acts more as a regulator, with insurance management being carried out by the mutuals and their unions. However, the decision to build up a mutual network in the municipalities is questionable, as it means that major support and monitoring efforts have to be deployed and dispersed. Following the example of UDAM, departmental or even regional mutuals could centralize the management of health insurance and focus technical support on a limited number of entities. Under this approach, the close relationship with the target populations could be ensured more efficiently by decentralized structures managed directly by the ACMU, in partnership with local authorities, or even in coalition with other social protection programmes such as the PNBSF. The ACMU seems to be moving increasingly towards this approach, given the positive UDAM results;
-
or, if we consider the autonomous nature of the community mutuals affirmed in the DECAM, as a form of social franchise, in which the ACMU is the franchiser, the mutuals and unions are the franchisees and the CMU scheme is the "social brand" that the mutuals have the right to exploit. A social franchising system is defined as "a method of collaboration that enables a socially useful organization with proven know-how to deploy its social impact by transferring this know-how to independent structures so that they can reproduce it in their territory". 120 This interpretation of the partnership between the ACMU and community mutuals would lead us to recommend that the ACMU, as franchisor, should focus on strengthening the quality of the "CMU" product, as well as technical and information flows and resource mobilization. At the same time, it should impose rigorous specifications on mutuals wishing to become franchisees, offer them training, provide media support and, above all, propose a high-quality and attractive social brand, the CMU scheme. Seen from this angle, Senegal could be considered not as an example of delegated management, but as an alternative approach to it.
In any case, the implementation of the CMU scheme in Senegal still faces many challenges, with membership rates remaining low and financial and information flows slow. Among these challenges, the deployment of a large number of community mutuals (676 mutuals plus their unions) raises the question of the capacity to provide sufficient technical support and to manage a particularly large flow of information. In the light of the above, another challenge may be to accurately define the CMU roll-out strategy, in order to use the right organizational methods and apply the appropriate strategy and tools
References
CARES (Comité d'Analyse et de Recherche Syndicale du Sénégal). 2018. "La problématique de la couverture maladie universelle au Sénégal: état des lieux, bilan et perspectives". CARES-SENEGAL, November 2018. https://www.ituc-africa.org/IMG/pdf/rapport_recherche_sp_econ_inform_senegal.pdf.
Deville C., Fecher F., Poncelet M. 2018. "Les mutuelles de santé subventionnées comme instruments de la Couverture Maladie Universelle au Sénégal". During the conference on the theme "Rencontre des Etudes Africaines en France (REAF)". Marseille, July 2018. Panel "Les chantiers de la santé en Afrique: répétition de scénarios déjà vu ou véritables dynamiques nouvelles?". July 2018. https://orbi.uliege.be/bitstream/2268/226717/1/Les%20mutuelles%20de%20sant%C3%A9%20subventionn%C3%A9es%20comme%20instruments%20de%20la%20CMU%20au%20S%C3%A9n%C3%A9gal.pdf.
Deville C., Hane F., Ridde V. and Touré L. 2018b. "La Couverture universelle en santé au Sahel : la situation au Mali et au Sénégal en 2018". Ceped Working Paper No. 40 (UMR 196 Université Paris Descartes IRD), October 2018. https://www.ceped.org/IMG/pdf/wp40.pdf.
Diagne A. and Sylla F. N. unpublished. "Evaluation du programme de Couverture Maladie Universelle, Rapport de synthèse de l'évaluation de la Couverture Maladie Universelle". Consortium pour la Recherche Economique et Sociale (CRES), Dakar, December 2021.
ILO (international Labour Organization. 2021. "Revue globale et analyse du système national de Protection sociale : Revue générale du système de Protection sociale au Sénégal et appui à la mise en œuvre de la Stratégie nationale de Protection sociale". International Labour Organization, ILO Country Office in Dakar (ETD/BP-DAKAR), Dakar, 2021. https://socialprotection-pfm.org/wp-content/uploads/2021/04/WEB-Revue-globale-du-systeme-de-protection-sociale.pdf.
Ndiaye P. and Ouattara O. 2017. "Potentiel des mutuelles de santé à la mise en œuvre de la Couverture maladie Universelle au Mali et au Sénégal". MASMUT, June 2017. https://bit.ly/3guBo0a.
PSD-CMU. 2013. Plan stratégique de développement de la couverture maladie 2013–2017. Ministry of Health and Social Action, 2013.
Ridde V., Antwi A., Boidin B., Chemouni B., Hane F. and Touré L. 2021. "Les défis des mutuelles communautaires en Afrique de l’Ouest". In Vers une couverture sanitaire universelle en 2030? Editions science et bien Commun: 2021.
Schwettmann J. 2022. ""Vers une couverture sanitaire universelle : Les cas du Bénin, de la Côte d'Ivoire, de l'Éthiopie, du Kenya, du Sénégal et de la Zambie". Friedrich Ebert Stiftung, January 2022.
16. The United Republic of Tanzania
In 2023, metropolitan United Republic of Tanzania 121 and Zanzibar 122 adopted national health insurance schemes. This case study traces the historical use of CBHI under the system preceding this reform. The reform follows a fragmented system that relied in part on voluntary schemes and achieved a low level of coverage in 2020.
16.1 Background
The process of implementing a national health insurance system in the United Republic of Tanzania began in the 1990s with the introduction of two public systems, the Community Health Fund (CHF) and the National Health Insurance Fund (NHIF), in 1996 and 2001 respectively. The aim of these systems was to protect the population in the face of ever-increasing health costs and to achieve universal health coverage in the long term.
The CHF was introduced by the Ministry of Health, initially as a pilot project in the Igunga district before being gradually extended to other regions and districts in the country. Each district CHF was a voluntary scheme, managed by the district council, which set the amount of household contributions and issued insurance cards. These were renewable each year and gave entitlement to a package of basic healthcare services in the district's health facilities throughout the year (Tungu et al., 2020).
The Community Health Fund Act enacted in 2001 123 set the following key objectives for the scheme:
-
To mobilize the community's financial resources to enable its members to access basic health services.
-
To provide quality, affordable healthcare services through a sustainable financial mechanism.
-
To improve the management of healthcare services in communities by decentralizing and empowering communities to participate in decisions that affect their health (Mtei and Mulligan, 2007).
The CHF was aimed at people living in rural areas. In 2009, the government introduced the Tiba Kwa Kadi (TIKA) with the same objectives as the CHF but focused solely on urban areas. 124 Another notable difference was that membership of the CHF was by household, whereas membership of the TIKA was individual (Kigume and Maluka, 2021).
At the same time, in 2001 the government introduced the NHIF as a compulsory health insurance scheme for central government employees. It was then extended to the formal private sector and, from 2013, to individuals, including those in the informal economy, willing and able to pay contributions. For the latter, the NHIF is a voluntary scheme operating in parallel to the CHF/TIKA, with no pooling of resources or risks within the districts (Tungu et al., 2020). The extension to the informal economy was prompted by the CHF's poor performance in enrolments, fund management and benefit coverage. This observation led to the Ministry of Health and Social Affairs in 2009 to start thinking about transferring the management of CHF operations to the NHIF. As this transfer was delayed, initiatives were taken in various regions to strengthen district CHFs by pooling funds at the regional level. These improved CHFs (iCHFs) also offer more comprehensive services and benefit from technical and financial support from external partners.
With just under a third of the population covered and a fragmented system of cover in the mid-2010s, the Ministry of Health, Community Development, Gender, Elderly and Children proposed a Single National Health Insurance (SNHI) scheme in its draft Health Funding Strategy 2016–2020. This scheme, which is still being studied, aims to consolidate the funds of the various existing systems and promote uniformity in all benefits, contributions and payments, including a set of minimum benefits for all. Its implementation should also be accompanied by strategies to increase enrolment and subsidies for the poor and ensure a greater role for private healthcare provision in order to widen access to care (Prabhakaran and Dutta, 2017).
Despite strong political support, implementation of the SNHI scheme has been delayed by lengthy consultations and multiple stakeholder reviews on the single pool of benefits and the financing of the scheme. The latter is designed to be funded mainly by member contributions and additional resources from general taxation to ensure SNHI sustainability. An actuarial study taking into account the merger of the current schemes is planned to support the final policy decisions and further stakeholder consultations should lead to the development of the Single National Health Insurance Scheme Act (SPARC, 2021; SPARC, 2021b; Prabhakaran and Dutta, 2017).
16.2 The national health insurance system defore 2023
Architecture and governance
The United Republic of Tanzania's national health insurance system is fragmented, with several schemes targeting different segments of the population and with different characteristics:
-
National Health Insurance Fund (NHIF): The NHIF was set up through Law No. 8 of 1999 125 and began operating in June 2001. The contribution of members employed in the public and private sectors, who make up the bulk of the insured persons, is 6 per cent of the basic monthly salary and is shared equally between the employer and the worker (Kuwawenaruwa, 2020). The scheme covers the principal member, their spouse and up to four dependants under the age of 18. Coverage has increased steadily, from 2 per cent of the total population in 2001/2002 to around 8 per cent in 2020 (Kuwawenaruwa, 2020). Funds are centralized and managed by the NHIF governing board, which is overseen by the Ministry of Health, to purchase health services from a range of accredited public and private health providers and facilities.
-
Social Health Insurance Benefit (SHIB): The SHIB was introduced in 2007 and is one of the seven benefits provided by the National Social Security Fund (NSSF). The SHIB offers health cover to contributors to the NSSF pension fund who choose to join (SPARC, 2021b). They have access to medical care at a public or private facility of their choice, to which they must be affiliated. This benefit is included in the workers' overall contribution to the NSSF, which amounts to 20 per cent of salary, shared equally between employee and employer (Mzee, 2013). Although it is a component of NSSF benefits, enrolment in the SHIB requires a separate procedure and few NSSF beneficiaries have enrolled in the SHIB, either because their employer already provides health cover or because they are unfamiliar with the scheme. Another reason is that the SHIB has agreements with only a very small number of health facilities, which limits access for policyholders spread across the country. NSSF pensioners are also entitled to join the SHIB, with a contribution rate of 6 per cent of gross pension. The SHIB makes capitation payments to approved health facilities and providers for health services rendered to members. This approach requires each member to choose a single facility where they will be covered, which then receives a lump sum per year for providing health services to that member. The amount of the capitation is not based on any specific information as the SHIB does not collect information on the costs incurred by members or on utilization rates. Special fee-for-service agreements are concluded with these facilities, particularly in Dar es Salaam, which refuse to take the capitation fee. The health services provided by the NSSF include a wide range of services, including outpatient services (consultations, basic and specialized diagnostics, medicines, and so on) and hospitalization (Haazen, 2012).
-
Improved Community Health Fund (iCHF): The iCHF is a voluntary community funding programme targeting persons on low incomes, mainly in the rural and informal sectors, which accounts for most of the national population. The iCHF is the result of a reform of the CHF conducted by the NHIF from 2018. The CHF, which has been in place since 2001, has been plagued by a number of failings, including poor management of funds by district councils. This reform aims to strengthen the scheme by pooling funds at the regional level and extending benefits to include health services at the regional level (Afriyie et al., 2021):
-
The NHIF is responsible for administration and marketing and takes on the risk of medical insurance.
-
Day-to-day management of the scheme has been moved from district to regional level (a region has several districts), by the Regional Administration, under the supervision of the Ministry responsible for local authority planning and sectoral interventions and the NHIF.
-
The system has dedicated staff at regional and district levels.
-
The scheme's coverage, previously limited to public facilities, has been extended to private healthcare providers. Beneficiaries now have access to all public and private healthcare facilities under contract with the region.
-
The annual fee is set at 60,000 Tanzanian shillings. Households pay half, with the remaining 50 per cent financed by the State through the NHIF (iCHF, 2021).
-
-
Micro health insurance: Micro health insurance schemes in the United Republic of Tanzania are underdeveloped and cover less than 1 per cent of the total population. These micro health insurance schemes are implemented, with the support of external partners, and administered by informal sector groups, such as the UMASITA (Tanzania Informal Sector Community Health Fund) and the VIBINDO (an umbrella organization for informal sector operators in the Dar es Salaam region). These schemes seek to strengthen informal sector communities by offering them better access to healthcare, improved quality of care and the means of promoting comprehensive healthcare services at affordable prices. Other schemes are promoted by religious-based organizations in different parts of the country, generally with the aim of alleviating the funding problems of church-run health facilities and helping the poor to gain access to healthcare. Overall, these microinsurance schemes face difficulties in target group communication and understanding and fragile financial viability, with separate risk pools and escalating costs (Haazen, 2012).
-
Private insurance schemes: These are company plans and voluntary individual schemes aimed at high-income households (SPARC, 2021b). Private health insurance companies, both national and international, are mainly concentrated in urban areas, with a low rate of coverage of the national population.
Population coverage
The detailed data available in 2020 indicated the following breakdown of population coverage by the health insurance systems described above, with all these systems together covering around 15 per cent of the national population:
Breakdown of coverage (2020)
|
NHIF |
SHIB |
CHF/TIKA |
Microinsurance |
Private insurance |
|
8% |
0.1% |
6% |
<1% |
1% |
Source: Binyaruka et al (2024)
Extending the iCHF was a priority objective of the United Republic of Tanzania's Health Sector Strategic Plan IV 2015–2020. However, despite the efforts made, coverage is currently stagnating at 7 per cent of the national population. This limited coverage is explained through studies and evaluations undertaken, including by the government, by problems linked to demand, such as poor understanding of the system, and factors linked to supply, including a limited package of services and poor quality of care in public health facilities, as well as weaknesses in governance (Afriyie et al., 2021).
Healthcare package
The Ministry of Health, Community Development, Gender, Elderly and Children has set out, and regularly reviews, a National Package of Essential Health Interventions (NPEHI), which groups together a set of priority services based on the population's health needs.
This national package contributes to the development of guidelines but is not a minimum benefit package for public and private insurance schemes, which use the NPEHI and the Ministry's guidelines as a basis for developing their own benefit packages (SPARC, 2021b).
Benefits under the various schemes
|
NHIF |
SHIB |
iCHF |
Microinsurance |
Private insurance |
|
Inpatient and outpatient care (with exclusions) provided by accredited public, religious-based and private facilities and pharmacies throughout the country This package is being reviewed based on comments from policyholders obtained through public consultations |
Care package similar to the NHIF (inpatient and outpatient care) in a limited number of approved facilities (around 300 facilities) |
Broad coverage of primary and hospital care with no specific exclusions; no clear process for reviews |
Primary healthcare coverage and hospitals |
Selective contracts with certain private service providers |
Source: SPARC, 2021b; Borghi et al., 2012
The NHIF reimburses services on a fee-for-service basis and uses the third-party payment system; it has an electronic system for monitoring the registration, verification, processing and reimbursement of health services to healthcare providers. More than 7,700 public, religious-based and private health facilities are covered by NHIF nationwide, including dispensaries, health centres, district hospitals, regional referral hospitals, area referral hospitals and national referral hospitals. Depending on the service, between 90 and 95 per cent of services are covered by third-party payment (Haazen, 2012). The NHIF also supports health facilities in improving the quality of service provision by granting loans to purchase medical equipment and improve facilities. Several health facilities, from primary to tertiary level, have thus been able to provide services that were previously unavailable. Other facilities have been readapted to improve the quality of care, both for NHIF members and for other users who visit the facilities (Kuwawenaruwa, 2020).
The services offered by the SHIB are similar to those of the NHIF, with the difference that inpatient expenditure is capped at 80,000 Tanzanian shillings. The SHIB has agreements with a limited number of healthcare providers with which it uses capitation to pay for health services. The SHIB oversees services through routine monitoring of healthcare providers.
All iCHF beneficiaries are entitled to the public and private contracted health services available up to regional hospital level, with some exclusions mainly for specialist services and medicines. Access to district and regional hospitals requires referral through a primary health facility (Lee et al., 2018). As administrator of the iCHF, the NHIF reimburses public and private health facilities by capitation, based on the number of registered households using them. The capitation amounts for private healthcare providers are 50 per cent higher than for public providers. This practice is intended to compensate for the fact that public providers receive government support to cover fixed costs such as rent or staff salaries (Wagenaar et al., 2016). The iCHF overseas benefits by tracking usage rates of the services covered (Kuwawenaruwa et al., 2022).
Financing
NHIF and SHIB funds are pooled at the national level, while iCHF funds are pooled and managed at the regional government level, which acts as purchaser. The NHIF budget is approved annually by parliament and is based on 6 per cent employee contributions paid by employees and employers. When the contributions collected are insufficient to cover claims, the deficit is covered by reserves built up from previous years' surpluses. The Fund faces a series of operational difficulties, including fraudulent attempts by members who do not contribute; this problem is largely the result of some employers not complying with the contribution rules laid down in the 1999 law, which requires them to pay their employees' contributions monthly (ISSA, 2017; Tungu et al., 2020).
For the SHIB, the annual budget is based on the previous year's budget and enrolment trends. Even though budget overruns may have not occurred, the law on the NSSF authorizes a supplementary budget subject to the approval of the Minister for Labour and Employment (SPARC, 2021b).
The iCHF is funded by household contributions and national government contributions. The annual contributions are set according to the geographical location of households (rural or urban area). In 2018, these contributions were as follows (Lee et al., 2018):
-
Dar es Salaam: 45,000 Tanzanian shillings (US$20) per individual or 150,000 Tanzanian shillings (US$65) per household of six people
-
Other urban areas: 30,000 Tanzanian shillings (US$13) per person
-
Rural areas: 30,000 Tanzanian shillings per household of six people. A household may contribute for additional members with a contribution of 30,000 Tanzanian shillings per adult and 10,000 Tanzanian shillings per child. Households of more than six people can opt to join as several households. These iCHF membership fees represent a significant increase on the CHF fees, which ranged from 5,000 Tanzanian shillings to 10,000 Tanzanian shillings per household.
The government contributes 30,000 Tanzanian shillings for each household of six people. The total contribution for a household is therefore 60,000 Tanzanian shillings (household contribution and government contribution) per year (Lee et al., 2018). Households deemed too poor are exempt from paying contributions. The collected contributions are deposited in the bank account of the NHIF regional office, which reimburses healthcare providers directly using the capitation system. These reimbursements are strictly monitored: the regional iCHF is supervised by the NHIF, which in turn reports to the Ministry of Health (Wagenaar et al., 2016).
The use of resources is fixed in advance:
-
80 per cent of household contributions are allocated to the payment of capitation to hospitals and primary healthcare facilities, 10 per cent to the commission of the agent who registers a household, 9 per cent to administrative costs and 1 per cent to reserves.
-
State funding is allocated 80 per cent to health facilities on a per capita basis, 15 per cent to administrative costs and 5 per cent to reserves (Afriyie et al., 2021).
16.3 The Community Health Fund: health insurance fully delegated to the districts before the transition to iCHF
Legal and organizational framework
The CHF and the TIKA targeted the informal economy population in rural and urban areas respectively. Both schemes were governed by the Community Health Fund Act 2001 and managed at the district level by district councils, council health service boards (CHSBs) and health facilities governing committees (HFGCs), which determined the benefit package, set contributions, provided outreach and supervised the operation of the CHF (Amani et al., 2021). Given the way they were set up, CHFs were somewhere between community mutuals and health insurance managed by a healthcare provider (the management of the Fund being integrated into the tasks of the CHSB). Overall, they fall within the definition of CBHI systems.
The district was the centre of the CHF's activities, with the CHSB having primary responsibility for introducing the CHF programme to the community, including village development committees (VDCs), village councils, households and healthcare providers. The CHSB was also responsible for the financial management and functioning of the health facilities. These functions were in fact entrusted to the local government authorities, which had major responsibilities in the provision of health services, and so there was no separate division between the purchasing function and the management and governance of the health sector at the district level, in the scheme set up in 2001. However, one of the CHF's objectives was to involve the community in questions of management and financial planning for the CHF; the 2001 law defined the organization needed for the CHF to function as follows:
-
At the district level, the CHSB was responsible for managing the programme. The CHSB included service provider representatives, four community members, including two women, and local authorities (Mtei and Mulligan, 2007), with the role of overseeing programme activities in the district and monitoring the use of funds.
-
CHF district coordinators oversaw the running of the programme and reported on the number of households registered and the contributions collected.
-
At the neighbourhood and village level, the VDC and village health committee, together with the HFGC and health workers from the facilities, mobilized the community to sign up to the programme.
The legal framework did not provide clear guidelines on implementing the CHF, and the districts had considerable autonomy. However, the communities took little ownership of the CHF, the statutes of which were drawn up by the district authorities. These statutes defined important aspects of implementation, such as contribution amounts and the criteria used for poor people who were exempt. This autonomy also led to a high degree of heterogeneity among district CHFs across the country; it also posed multiple challenges for the generalization and management of the programme (Wang and Rosemberg, 2018). Another consequence was the fragmentation of the system and the lack of equalization between CHFs with coverage that was limited to their respective districts.
Distribution of functions within the CHF and iCHF frameworks
In each district, the CHSB was responsible for the CHF and, as such, carried out the following functions:
-
Supervision of the scheme's activities in the district
-
Mobilization and management of funds
-
Purchasing services provided by healthcare facilities
-
Definition of exemption criteria for poor households
-
Monitoring the collection of contributions and expenses
-
Drawing up an annual plan
Household registration operations were based on health facilities where users could register with the CHF when seeking care – with a significant risk of encouraging adverse selection. In some districts, registration was also based on public-private partnerships with local associations and cooperatives for group registration. Other districts carried out registration campaigns during school enrolment in local secondary schools.
The CHSB was also responsible for awareness-raising and communication through the community representatives who were members of the CHSB. They were responsible for disseminating information to CHF beneficiaries on the functioning of the scheme, with the aim of involving them in CHF operations (Mtei and Mulligan, 2007).
At the neighbourhood and village level, the VDC, village health committee, together with the HFGC and health workers from the facilities, mobilized the community to sign up for the CHF. It should be pointed out that the Community Health Fund Act 2001 did not require members of the CHSB, village councils or VDCs to be members of the CHF.
The districts were responsible for identifying and registering poor households. In the absence of a national directive regulating the criteria that could be used for the CHF exemption policy, the CHSB relied on village councils, neighbourhood authorities and other institutions (Department of Social Work, Department of Social Protection, and so on) to identify poor households. The district authorities were responsible for mobilizing the resources to cover these households through the CHF, including from external partners (Wang and Rosemberg, 2018).
Regulatory oversight of the CHF/TIKA was provided by the Ministry of Health and the NHIF. A number of challenges were identified, including poor capacity to mobilize membership, manage funds and produce reliable membership data. Although the CHSBs played the dual role of "provider" and "purchaser" of health services, membership fees were not used to improve health services in the covered health facilities that were supposed to provide quality healthcare. As a result, CHF members have been faced with an ongoing deterioration in healthcare services, including a chronic shortage of medicines. This discouraged membership and membership numbers fell significantly (NHIF, 2017).
This fact led the NHIF to develop a CHF action plan (2009–12) which laid the foundations for an "Improved Community Health Fund" (iCHF) (ISSA, 2016). As part of this CHF action plan (2009–12), the NHIF proposed a new initiative to promote an "Improved Community Health Fund" (iCHF). To initiate this reform of the CHF, the Ministry of Health and the NHIF also signed an agreement with an external NGO, PharmaAccess, which had set up a CBHI scheme for coffee growers in a fairly successful region.
As detailed above, a number of strengthening measures were introduced:
-
Management of the scheme was transferred to the regional authorities (Regional Administrative Secretariat (RAS)) under the supervision of the NHIF and its regional offices, which is responsible for administration at the national level. This involved the professionalization of management, building the capacity of the regional and district authorities and introducing new mechanisms for registering members, collecting contributions and an information system.
-
Services were reviewed and harmonized between regions, by extending them to regional hospitals and private healthcare providers (Haazen, 2012).
-
Contributions, which varied from 5,000 Tanzanian shillings to 10,000 Tanzanian shillings in the CHF, were increased and harmonized at 30,000 Tanzanian shillings for a household of six people and doubled by a matching fund from the government to reach a total of 60,000 Tanzanian shillings to cover all benefit and administrative expenses.
-
Contributions are deposited into the accounts of the NHIF's regional offices, which administer the scheme and reimburse healthcare providers on a capitation basis, providing them with a stable income.
-
The benefits, which only covered outpatient care, were extended to inpatient care (limited to five days) and the agreement was extended to private healthcare providers, including religious-based ones.
-
Teams of community health workers and iCHF agents were trained and deployed to raise community awareness of the iCHF and carry out administrative functions such as contribution collection.
-
A free telephone number was set up to enable households to obtain information, make suggestions or submit complaints.
These reforms had a significant impact, with an increase in membership from 4 per cent in 2008 to 8.3 per cent in 2011–2012, followed by some stagnation, which was still far from the 30 per cent coverage rate expected for 2015 (Amani et al., 2021).
Distribution of functions in the community-based health insurance system
|
Functions |
Distribution |
||
|
CHF |
iCHF |
||
|
District |
Region |
NHIF |
|
|
Definition of the healthcare package |
X |
Based on the package defined by the Ministry of Health |
|
|
Agreements |
X |
X |
X |
|
Education and promotion |
X |
X |
X |
|
Enrolment, membership and renewal |
X |
X |
|
|
Contribution collection |
X |
X |
|
|
Pooling of risks covered |
X |
X |
X |
|
Purchasing services |
X |
X |
X |
|
Healthcare services |
X |
||
|
Follow-up and steering |
Ministry of Health and NHIF |
Districts and region |
Ministry of Health and NHIF |
16.4 Impact and lessons learned
The introduction of the CHF under the 2001 Act was not accompanied by clear management procedures and came up against weak management capacity at the district level. An evaluation by the Ministry of Health in 2003 showed that a quarter of districts were mismanaging CHF funds, others were not using these funds to reimburse health services and, overall, despite the obligations set out in the Act, councils were not carrying out regular audits or reporting to community members (Mtei and Mulligan, 2007).
The NHIF's involvement in strengthening the CHF has not had the desired effect and, although the proposed measures were ultimately aimed at incorporating the CHF's management structures into the NHIF in order to improve efficiency and supervision, the iCHF remains a system belonging to the districts and regions. Overall, despite the progress made, the United Republic of Tanzania's national SHP system remains fragmented, with a wide range of schemes each catering for different socio-economic groups, small risk pools and a wide range of benefits. Overall, in 2016, the NHIF, the SHIB, the iCHF and private insurance together accounted for only 8 per cent of total health expenditure, with the state financing 54 per cent and direct household expenditure 38 per cent (SPARC, 2021b).
The United Republic of Tanzania now aspires to having a national health insurance system with the implementation of a single national health insurance (SNHI) scheme. However, for now the country lacks a clear framework for how the various current systems will be merged, or for their role in the new SNHI scheme. Studies also point to a lack of institutional and socio-economic capacity to develop an SNHI scheme (Lambrecht, 2017). The collaboration between the NHIF and PharmaAccess, which has led to the promotion of the iCHF, has been highlighted as an area for consideration in extending the scheme to the informal economy and building universal coverage. This would involve establishing a clear legal framework laying the foundations for a public-private partnership between the State and NGOs, or even private for-profit players. The latter could provide the State with innovative and effective approaches, particularly in the area of digital/mobile technology, to the payment of contributions and healthcare.
The experience of the CHF/TIKA, and subsequently the iCHF, is a perfect example of CBHI, promoted as part of a national programme and with parameters that are defined outside of the community. Although the community is involved, it is not a mutual society model, nor is it a system for delegating functions to mutuals or other forms of autonomous entities.
References
Afriyie O., Brady Hooley D., Mhalu G., Tediosi F. and Mtenga S. M. 2021. "Governance factors that affect the implementation of health financing reforms in Tanzania: an exploratory study of stakeholders' perspectives". In BMJ Global Health 6(8). August 2021: e005964. https://doi.org/10.1136/bmjgh-2021-005964.
Amani P.J., Hurtig A., Frumence G., Kiwara A.D., Goicolea I. and San Sebastiån M. 2021. "Health insurance and health system (un) responsiveness: a qualitative study with elderly in rural Tanzania". In BMC Health Services Research 21(1140). https://doi.org/10.1186/s12913-021-07144-2.
Binyaruka P., Martinez-Alvarez M., Pitt C. and Borghi J. 2024. "Assessing equity and efficiency of health financing towards universal health coverage between regions in Tanzania". In Social Science & Medicine 340, 116457. https://www.sciencedirect.com/science/article/abs/pii/S0277953623008146?dgcid=rss_sd_all#:~:text=The%20average%20efficiency%20score%20across,out%2Dof%2Dpocket%20payments.
Borghi, J., Mtei G. and Ally M. 2012. "Modelling the implications of moving towards universal coverage in Tanzania". In Health Policy and Planning 27(1): i88–i100. https://doi.org/10.1093/heapol/czs009.
Haazen D. 2012. "Making health financing work for poor people in Tanzania". World Bank, 2012. https://doi.org/10.1596/978-0-8213-9473-1.
iCHF (Improved Community Health Fund). 2021. ICHF website.
ISSA (International Social Security Association). 2016. "Improved Community Health Funds (iCHF): Third-party relationships improving health service provision and members' recruitment". https://ww1.issa.int/gp/162382.
— 2017. "Strengthening compliance through identity cards rejection: A case of the National Health Insurance Fund – United Republic of Tanzania”. ISSA website. https://www.issa.int/gp/162462.
Kigume R. and Maluka S. 2021. "The failure of community-based health insurance schemes in Tanzania: opening the black box of the implementation process". In BMC Health Services Research 21: 646. https://doi.org/10.1186/s12913-021-06643-6.
Kuwawenaruwa A. 2020. "Strategic Healthcare Purchasing Arrangements within the National Health Insurance Fund (NHIF) in Tanzania". Strategic Purchasing Africa Resource Center (SPARC) (blog), 16 September 2020. https://sparc.africa/2020/09/strategic-healthcare-purchasing-arrangements-within-the-national-health-insurance-fund-nhif-in-tanzania/.
Kuwawenaruwa A., Makawia S., Binyaruka P. and Manzi F. 2022. "Assessment of Strategic Healthcare Purchasing Arrangements and Functions Towards Universal Coverage in Tanzania". In International Journal of Health Policy and Management 11(12): 3079–3089. https://www.ijhpm.com/article_4294.html.
Lambrecht J. 2017. "Universal Health Coverage in Tanzania, Evaluating the Potential of a Public-Private Partnership in Tanzania's Health Financing System". Thesis, KU Leuven University, Belgium, 2017. https://www.issa.int/gp/162462.
Lee B., Tarimo K. and Dutta A. 2018. "Tanzania's Improved Community Health Fund, An Analysis of Scale-Up Plans and Design". Palladium, Health Policy Plus, Policy Brief, USAID, October 2018. http://www.healthpolicyplus.com/ns/pubs/10259-10469_TanzaniaiCHFScaleUpbrief.pdf.
Mtei G. and Mulligan J. 2007. "Community Health Funds in Tanzania: a Literature Review”. Consortium for Research on Equitable Health Systems (CREHS), January 2007. http://www.research4development.info
Mzee A. 2013. "Assessment of the Impact of Social Health Insurance Benefit on Customer Satisfaction: The Case of National Social Security Fund". Thesis, Mzumbe University, 2013.
NHIF (National Health Insurance Fund). 2017. "Improved Community Health Funds (iCHF): Third-party relationships improving health service provision and members’ recruitment – A case of the National Health Insurance Fund”. ISSA, Good Practices in Social Security. https://www.issa.int/sites/default/files/documents/good-practices/233428-en.pdf.
PharmAcces. 2016. "A Closer Look at the Healthcare System in Tanzania". October 2016. https://www.pharmaccess.org/wp-content/uploads/2018/01/The-healthcare-system-in-Tanzania.pdf.
Prabhakaran S. and Dutta A. 2017. "Actuarial Study of the Proposed Single National Health Insurance Scheme in Tanzania: A Summary Brief". Palladium, Health Policy Plus, USAID, November 2017. http://www.healthpolicyplus.com/pubs.cfm?get=7168.
SPARC (Strategic Purchasing Africa Resource Center). 2021. "Developing a Single National Health Insurance in Tanzania Has Been a Long Journey of Incremental Changes and Stakeholder Engagement". SPARC (blog), 10 June 2021. https://sparc.africa/2021/06/developing-a-single-national-health-insurance-in-tanzania-has-been-a-long-journey-of-incremental-changes-and-stakeholder-engagement/.
-
2021b. "Strategic Health Purchasing in Tanzania: A Summary of Progress, Challenges, and Opportunities". May 2021. https://sparc.africa/wp-content/uploads/2021/06/SPARC_Policy_Brief_TANZANIA_L7.pdf
Tungu, M., Amani P.J., Hurtig A.K., Kiwara A. D., Mwangu M., Lindholm L. and San Sebastiån M. 2020. "Does health insurance contribute to improved utilization of health care services for the elderly in rural Tanzania? A Cross-Sectional Study". In Global Health Action 13(1). 31 December 2020: 1841962. https://doi.org/10.1080/16549716.2020.1841962.
Wagenaar C., Marwa H. and Irrgan E. 2016. "ICHF, How a public-private partnership can help make healthcare work in Northern Tanzania". PharmAcces, September 2016. https://www.pharmaccess.org/wp-content/uploads/2016/12/iCHF-How-a-public-private-partnership-can-help-make-healthcare-work-in-Northern-Tanzania.pdf.
Wang H. and Rosemberg N. 2018. "Universal health coverage in low-income countries: Tanzania's efforts to overcome barriers to equitable health service access". Universal Health Coverage study series, no. 39. Washington: World Bank Group, 17 January 2018. https://documents.worldbank.org/en/publication/documents-reports/documentdetail/820591516179637357/universal-health-coverage-in-low-income-countries-tanzania-s-efforts-to-overcome-barriers-to-equitable-health-service-access
17. Uruguay
17.1 The national social health protection system
Uruguay's current SHP system is the culmination of a series of reforms that began in 2005 with the creation of national health insurance. The process continued with the decentralization of the main public healthcare provider, the State Health Services Administration (Administración de los servicios de salud del Estado, ASSE), which was given the tasks of governance and healthcare provision that had previously been the responsibility of the Ministry of Health. The reforms were completed in 2007 with the introduction of a single fund to finance healthcare services, the National Health Fund (Fondo Nacional de Salud, FONASA), and the creation of the National Integrated Health System (Sistema nacional integrado de salud SNIS).
Before the reforms, Uruguay's SHP system was characterized by the strong presence of collective medical care institutions (instituciones de asistencia médica colectiva, IAMC), many of which had cooperative or mutual society status, which provided a significant proportion of private health services, particularly through prepaid medical schemes that they managed themselves. These organizations, most often managed and owned by doctors, were closely associated with the social security system and provided health services on payment of a prepaid contribution. The system was highly fragmented, with different entities covering different population groups, while social security covered only a tiny proportion of the population
Uruguay's SNIS was designed to integrate the various schemes and rectify the fragmentation of the system. The SNIS guarantees "access to comprehensive health services for all persons residing in the country"
17.2 The role of cooperative and mutual organizations after the 2007 reform
National health insurance covers formal workers who pay into the FONASA, as well as their dependants (children aged under 18, adults with disabilities, spouses) and pensioners. The proportion of the population covered by the FONASA is 73.2 per cent.
Care is provided through the ASSE's public delivery network and through private providers (IAMC or private for-profit providers). Beneficiaries of the national health insurance system have a choice of healthcare provider network. They must register with a network (the ASSE, IAMC, other private provider) within the first 180 days of joining the health insurance scheme and may change network every two years.
Thus, under the 2007 reform, IAMC (most often with cooperative or mutual society status) have become healthcare provider networks for FONASA beneficiaries who so choose. They are also entitled to continue collecting additional contributions for complementary cover (in the case of complementary cover, there is usually no separation between the functions of insurer and service provider).
The FONASA remunerates the public and private provider networks on a capitation basis, in other words by paying a lump sum per insured person registered. This amount, adjusted for patient risk (gender and age), is defined jointly by the Ministry of the Economy and Finance and the Ministry of Health. The capitation is also adjusted according to results: around 8 per cent of remuneration depends on the achievement of public health objectives
The organizations providing healthcare services must sign a management agreement, which sets out the service criteria and the compulsory nature of the single package of services determined centrally. In the private sector, the main provider networks are IAMC, not-for-profit organizations, which may be mutuals, health professional cooperatives or assistance services.
17.3 Characteristics of delegation
In Uruguay, IAMC are key players in the SNIS. These private organizations, which have been present in the country since the end of the nineteenth century, have evolved to become the main component of private health service provision
The current legal framework distinguishes between three types of IAMC:
-
Medical care associations, based on mutual society principles, which provide medical services to their members.
-
Healthcare cooperatives, which provide medical services to their members.
-
Healthcare services set up by private companies to provide medical services to their employees
(Ley 15.181, 1981) .
Law No. 15.181 of 1981 modified the regulatory framework for IAMC. The Ministry of Public Health is now responsible for supervising, overseeing and inspecting the technical, accounting and other aspects of IAMC functioning. It is also the Ministry of Public Health, the system's governing body, which delegates functions, particularly in the area of medical care.
Before the SNIS was created in 2007, IAMC were already a key part of the health system, covering half of the Uruguayan population. IAMC were already highly regulated by law. During the reform, IAMC were integrated into the new institutional architecture as healthcare provider networks. Changes were also made to the regulatory framework, one of the main ones being that IAMC are now required to offer all the benefits in the single package of care set out at the national level – the Comprehensive Healthcare Plan (Plan integral de atención a la salud, PIAS), including those they had not previously covered, such as certain types of prosthesis and mental health care.
IAMC derive most of their resources from the lump-sum rate per insured person (capitation) paid by the FONASA. The amount of the capitation is calculated on the basis of the expected average expenditure per patient and adjusted according to risk (age and gender)
Table 1. Composition of IAMC revenue, 2021
|
Revenue |
Share |
||
|
1 |
Deferred revenue |
FONASA capitation |
64.4% |
|
FONASA achievement of public health objectives |
6.3% |
||
|
Inflation adjustment – deferred revenue |
2.8% |
||
|
Group membership fees |
2.1% |
||
|
Contributions from individual members |
2.0% |
||
|
Other |
4.5% |
||
|
Total deferred revenue |
82.0% |
||
|
2 |
Lump sum |
7.3% |
|
|
3 |
Sale of services |
8.4% |
|
|
4 |
Other operating revenue |
2.3% |
|
|
|
Total revenue |
100% |
|
Source: Uruguayan Ministry of Public Health
Delegated functions
|
Function |
Delegated function |
|
Design of the SHP scheme |
|
|
Population coverage |
None. The definition of who is covered is determined centrally by the public authorities. |
|
Definition of services |
The package of benefits is defined in the PIAS and is binding on all healthcare providers, including IAMC. The latter can offer an additional package of benefits as part of their complementary health insurance. |
|
Network of service providers |
Current regulations recognize IAMC as networks of healthcare providers, as well as other providers. Healthcare associations (mutuals), health professionals and healthcare service cooperatives. Of the 44 IAMC in the country (10 in Montevideo and 34 in the regions), more than 30 have a range of first-, second- and third-level healthcare facilities IAMC are first and foremost networks of healthcare providers, and the system of capitation payment per insured person transfers part of the risk management to them (intra-network). They also act as insurers for complementary health insurance. |
|
Implementation |
|
|
Education/promotion |
Pursuant to article 45 of Law No. 18.211, health promotion and prevention activities are among the services that the public and private bodies of the SNIS must provide to their users. As part of the payment made to mutuals for achieving objectives, the FONASA includes indicators on training and promotion. Among the indicators selected in 2020 for payment based on health objectives were training in institutional protocols for dealing with victims of domestic and sexual violence, prevention initiatives against gender-based violence and abuse of older persons, and promotion of childbirth preparation courses. The law also provides for programmes to manage and prevent addictions and to combat smoking. |
|
Membership |
National health insurance beneficiaries can join a healthcare network run by one of the IAMC, which is obliged to cover them. Members sign up for a minimum of two years; however, they can ask to change organization if they move, have problems with coverage or for reasons of geographical accessibility. |
|
Collection of membership fees (or other resources) |
Contributions from employees and employers who are members of the FONASA are collected by the Banco de Prévision Social (Social Security Bank – Uruguay's national social security fund), not by the IAMC. The latter receive a capitation per insured person registered with them, adjusted to the insured person's individual risk profile (age, and so on). |
|
Pooling of funds |
The resources that finance national health insurance are integrated into a single, public and compulsory fund, the FONASA. The various healthcare provider networks, including IAMC, manage the risk at their level on the basis of the amount of the capitation adjusted to the risk profile. This adjustment has been put in place to take account of beneficiaries' risk factors (age and gender), and to avoid membership refusals by the IAMC and other approved networks. |
|
Payment of service providers (contracts, reimbursements) |
IAMC manage their own healthcare networks and allocate resources to their health facilities. |
|
Healthcare services |
Healthcare is provided in accordance with the PIAS and the management agreement. The provision of services is the main function of IAMC. |
|
Dispute settlement |
Pursuant to article 54 of Law No. 18.211, the National Health Board (Junta Nacional de Salud, JUNASA) "may set up a procedure for handling complaints and claims from users of the Integrated National Health System". The Ministry of Health's users' office sets out the mechanisms for filing complaints and deals with claims that have not been settled by the user relations committee that all healthcare providers are required to set up. This committee is responsible for receiving, recording and processing requests and complaints made by members. In addition, as stipulated in the management agreement, the service providers must carry out regular satisfaction surveys on the services provided. |
|
Quality assurance |
Overall control of the quality of care is provided by the Ministry of Health. The Ministry of Health’s Committee on Bioethics and Comprehensive Quality of Healthcare was created through Decision No. 610/005. An honorary and advisory body, it has educational and standard-setting functions. Under Decree No. 274/010, healthcare providers must set up honorary bioethics committees (regulations relating to the law on the rights and obligations of patients and users of healthcare services) with the aim of training medical staff and patients and advising the technical management of each establishment on bioethics issues and the comprehensive quality of care. |
17.4 Impact and lessons learned
IAMC are healthcare networks where 57.7 per cent of the population are members, making them the country's main providers under the national health insurance scheme. A total of 52 per cent of users are women and 48 per cent are men. In total, almost 2.2 million people use IAMC, 70 per cent of whom are associations, 28 per cent are mutuals and 2 per cent cooperatives.
Table 2. Number of IAMC users, 2023
|
FONASA members |
Non-members of FONASA |
TOTAL |
|
|
Women |
1 040 117 |
79 707 |
1 119 824 |
|
Men |
955 284 |
92 133 |
1 047 417 |
|
Total |
1 995 401 |
180 380 |
2 167 241 |
Source:
The number of IAMC users has risen significantly in recent years, from 1.9 million in 2010 to almost 2.2 million in 2023, an increase of 15.1 per cent (figure 2).
The number of IAMC members contributing to the FONASA increased by 43.7 per cent between 2010 and 2021, while the number of voluntary members fell by around 64 per cent over the same period.
The increase in the number of IAMC members is the main reason for the overall increase in health coverage. This upward trend is due primarily to the gradual extension of FONASA coverage to new segments of the population. Spouses of insured persons were included as beneficiaries in 2011, and coverage of people not in work increased in 2012. This development can also be attributed to the decline in informal employment and the inclusion of more workers in the social security system. The long-standing presence of IAMC and the close links they maintain with their users, as well as the positive perception of the quality of the services they provide, also explain why they are succeeding in attracting more members.
Figure 2. Growth in the number of IAMC members, 2010–2021
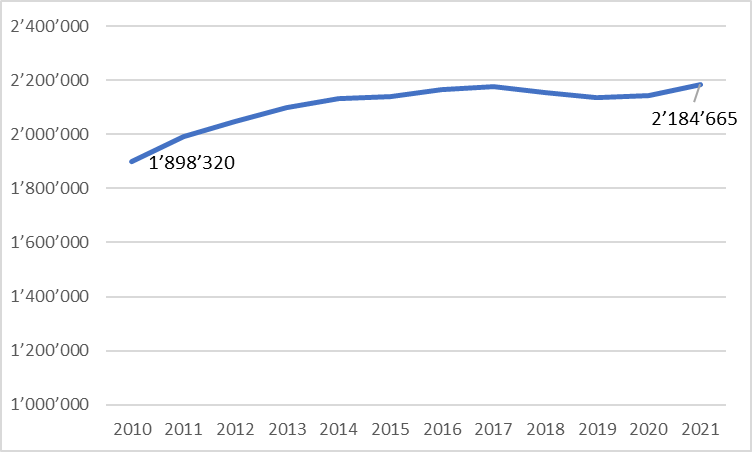
Source: Uruguayan Ministry of Public Health
The health system reforms implemented since 2005 have radically changed the way IAMC operate, with a number of consequences. Before the reforms, IAMC insured persons on an individual basis and drew their resources from contributions paid by households. Since the creation of the SNIS, the FONASA has been financing IAMC, which now only insure individuals who are not covered by the SNIS and can afford or are covered by complementary health insurance. The change in the source of funding has also led to changes in the way the FONASA pays IAMC (capitation) and a fall in the revenue received per insured person. This fall was offset by a sharp increase in the number of users, which undoubtedly helped to avoid tensions during the implementation of the reform
In the years following the reform, the increase in the number of insured persons benefited IAMC, which became the main healthcare providers. This development was accompanied by changes in financial management. The introduction of capitation and a target-based remuneration component has led to an increase in the proportion of revenue from the FONASA (from 30 per cent in 2005 to 60 per cent in 2011)
The reform has also changed the distribution of healthcare provision. IAMC have become the leading providers, ahead of the ASSE. The reform has also made it possible to reduce inequalities in the healthcare provided by the various providers through the centralized definition by the public authorities of a single healthcare package.
References
Aran, D. and Laca, H. 2011. "Sistema de salud de Uruguay". In Salud Pública de México 53(2): S265–S274.
Arbulo, V., Pagano, J. P., Rak, G., Rivas, L., and Jorcin, G. 2012. “El camino hacia la Cobertura Universal en Uruguay: Evaluación y revisión del financiamiento del Sistema de Salud uruguayo", p56.
References
Boyer S., Delesvaux C., Foirry J.-P. and Prieur C. 2000. Le risque maladie dans les assurances sociales : bilan et perspectives dans les PVD. Directorate-General for International Development and Cooperation, Ministry for Europe and Foreign Affairs, Paris, September 2000. https://www.diplomatie.gouv.fr/IMG/pdf/Le_risque_maladie_dans_les_assurances_sociales.pdf.
Burkina Faso, Ministry of Public Service, Labour and Social Welfare. 2022. Inventaire des mutuelles sociales du Burkina Faso – 2020. ILO, 2022.
Coheur A., Jacquier C., Schmitt-Diabaté V. and Schremmer J. 2008. Linkages between statutory social security schemes and community-based social protection mechanisms: A promising new approach. Technical Commission on Medical Care and Sickness Insurance and Technical Commission on Mutual Benefit Societies. 10–15 September 2007. ISSA Technical Report No. 9, 2008. https://www.issa.int/sites/default/files/documents/publications/TR-09-2_en-25427.pdf.
Dreyfus, M. 2017. Histoire de l’économie sociale: de la Grande Guerre à nos jours. Rennes,
Presses universitaires de Rennes.
European Union (EU). 2015. Directive 2009/138/EC of the European Parliament and of the Council of 25 November 2009 on the taking-up and pursuit of the business of Insurance and Reinsurance (Solvency II) (recast). European Union, 31 March 2015. https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:02009L0138-20150331&qid=1434108231040&from=FR.
Grijpstra D., Broek S., Buiskool B.-J. and Plooij M. 2011. The role of mutual societies in the 21st century. European Parliament, July 2011. https://www.europarl.europa.eu/RegData/etudes/etudes/join/2011/464434/IPOL-EMPL_ET(2011)464434_EN.pdf.
International Association of Mutual Benefit Societies (AIM). 2017. “What is a mutual?” https://www.aim-mutual.org/what-is-a-mutual/.
International Cooperative and Mutual Insurance Federation (ICMIF). 2019. Global Mutual Market Share, the global mutual and cooperative insurance sector in 2017. ICMIF, February 2019. https://www.icmif.org/wp-content/uploads/2020/11/MMS-ENG-1.pdf
International Labour Organization (ILO). 2012. The strategy of the International Labour Organization. Social security for all: building social protection floors and comprehensive social security systems.
— 2020. “Social Protection Spotlight. Towards Universal Health Coverage: Social Health Protection Principles”. ILO brief, March 2020. https://www.social-protection.org/gimi/Media.action?id=17242.
— 2020b. “Social Protection Spotlight. 2020. ILO Social Security Standards: Learn, Ratify and Apply”. ILO brief, September 2020. https://www.social-protection.org/gimi/Media.action?id=16565.
— 2021b. "Revue globale et analyse du système national de Protection sociale : Revue générale du système de Protection sociale au Sénégal et appui à la mise en œuvre de la Stratégie nationale de Protection sociale". International Labour Organization, ILO Country Office in Dakar (ETD/BP-DAKAR), Dakar, 2021. https://socialprotection-pfm.org/wp-content/uploads/2021/04/WEB-Revue-globale-du-systeme-de-protection-sociale.pdf.
— 2022. “Cooperatives and the World of Work No. 16 – Legal Compendium on the Social and Solidarity Economy”. ILO brief, May 2022. https://www.ilo.org/publications/cooperatives-and-world-work-no-16-legal-compendium-social-and-solidarity.
International Social Security Association (ISSA). 2013. “Mutual benefit societies: A tool for developing social protection worldwide, particularly in the health sector”. Steering Committee of the Technical Commission on Mutual Benefit Societies. World Social Security Forum, 31st General Assembly, Doha, 10–15 November 2013.
Krajeski, D. 2019. “Assurer l’activité des sous-traitants”. In Sécuriser la sous-traitance : Quels nouveaux défis ? 167–76. IFR seminar proceedings. Toulouse: Presses de l’Université Toulouse 1 Capitole. http://books.openedition.org/putc/7172.
Letourmy A. 2008. “On the development of health insurance in low-income countries: the case of African countries”. Comptes Rendus Biologies 331(12): 952–963. https://comptes-rendus.academie-sciences.fr/biologies/articles/10.1016/j.crvi.2008.08.013/.
Mathauer I., Mathivet B., and Kutzin K. 2017. “Community based health insurance:
How can it contribute to progress towards UHC?” Health Financing Policy Brief No. 3, WHO, 2017. https://www.who.int/publications/i/item/WHO-HIS-HGF-PolicyBrief-17.3.
Niang, M., Gélinas, É., Samb, O. M., Tessier, L., Mailfert, M., Iradukunda, A., and Ridde, V. 2023. ”The role of mutuals and community‐based insurance in social health protection systems: International experience on delegated functions”. International Social Security Review 76(2): 3–29. https://onlinelibrary.wiley.com/doi/10.1111/issr.12323
Scheil-Adlung, X. 2007. “Social Health Protection: An ILO strategy towards universal access to health care”. Issues in Social Protection. Discussion paper 19. ILO, August 2007. https://www.ilo.org/sites/default/files/wcmsp5/groups/public/@ed_protect/@soc_sec/documents/publication/wcms_secsoc_14083.pdf.
Schremmer, J. et al. 2009. “Extending health care coverage: Potential linkages between statutory social security and community-based social protection”, in International Social Security Review, Vol. 62(1).
Sossa T. 2010. “Couverture, financement et exclusion: l’assurance-maladie en Afrique”. 2010. In Finance & Bien Commun 37–38, No. 2–3: 94–103. https://shs.cairn.info/revue-finance-et-bien-commun-2010-2-page-94?lang=fr&ref=doi.
Tessi #Insights. 2022. “Assurance : 3 points clés à connaître pour optimiser sa délégation de gestion”. https://www.tessi-blog.com/delegation-gestion-assurance/.
United Nations Development Programme (UNDP). 2021. Informality and Social Protection in African Countries: A Forward-looking Assessment of Contributory Schemes. UNDP and ILO, 2021. https://www.ilo.org/sites/default/files/wcmsp5/groups/public/%40africa/%40ro-abidjan/documents/publication/wcms_770203.pdf.
Van Rompaey C. 2013. “L’essor des mutuelles de santé: l’exemple de l’Afrique de l’Ouest (II)”. In Revue Démocratie, 3 mai 2013. https://www.revue-democratie.be/index.php?option=com_content&view=article&id=971:lessor-des-mutuelles-de-sante-lexemple-de-lafrique-de-louest-ii&catid=30&Itemid=130.
Acknowledgements
This report was coordinated by Lou Tessier and Olivier Louis dit Guérin. The drafting team is composed of (in alphabetical order): Dramane Batchabi, Marielle Phe Goursat, Olivier Louis dit Guérin, Mathilde Mailfert, Ana-Cristina Mena (Colombia and Uruguay case studies) and Yuta Momose (Japan case study).
The authors would like to thank the national experts who reviewed the case studies: Bouaphat Phonevixay (Lao People’s Democratic Republic), Khim Keo Vathanak (Cambodia), Jairo Humberto Restrepo (Colombia) and Braulio Zelko (Uruguay). The authors would also like to thank all those who provided contributions and comments to improve this publication: Guy Tchami (ILO, Cooperative Unit (COOP)), Giulio Bordon (ILO, Cambodia), Martial Kouakou (ILO, Côte d'Ivoire), Aurélie Klein (ILO, Rwanda).
The authors would especially like to thank the members of the Advisory Council for Social Mutuality of the West African Economic and Monetary Union (WAEMU) at the joint ILO-WAEMU tripartite thematic workshop on the role of social mutuals in national social health protection systems held in Dakar from 11 to 13 October 2023.
The authors are grateful for the support of Valerie Baldwinson in the translation of the working paper into English.
This working paper has been published on the basis of a literature review process initiated following the publication of a scoping review on the same theme: Niang, M., Gélinas, É., Samb, O. M., Tessier, L., Mailfert, M., Iradukunda, A., and Ridde, V. (2023), "The role of mutuals and community-based insurance in social health protection systems: International experience on delegated functions", in the International Social Security Review, 76(2), 3–29.

