
Making social protection work for gender equality: What does it look like? How do we get there?
Abstract
Attesting to feminist interest in social protection, there exists today a voluminous and growing literature, produced by academics, international organizations, civil society and think tanks, examining the gender content and impacts of social protection policies. The added value of this paper is that it is the first time that the ILO’s Universal Social Protection Department has produced a consolidated message on its perspective and approach to enhancing the gender-responsiveness of social protection policies, anchored in international social security standards and guided by a life-cycle approach to system-building.
In so doing, the paper underlines the critical interconnections and need for coherence between social protection policies and economic policies, especially employment policies (focusing on all types of employment), on one hand, and social protection policies and public investment and regulation of social services (especially healthcare and care services) on the other. It also both highlights new data and underlines remaining data gaps that need to be urgently closed to enable the monitoring of the impact of social protection policies on gender equality. It intends to encourage social protection policymakers, as well as social partners and other stakeholders, everywhere to think more systematically about the gender content and impact of social protection when they are advocating for or modifying existing policies, and designing and administering schemes, to better promote gender equality.
Executive Summary
Social protection policies are indispensable for enhancing gender equality and realizing women’s rights. Yet in practice, they have insufficiently addressed the gender-specific risks and structural constraints that women face across the life cycle, thereby falling short of their potential to promote gender equality. The added value of this paper is in providing a comprehensive perspective on how to enhance the gender-responsiveness of social protection policies and systems, anchored in international social security standards and guided by human-centred design and a life-cycle approach to system-building.
A good starting point is to underline that all life-cycle benefits are relevant to gender equality, and not only those relating to maternity or parenthood. However, in practice, when it comes to gender-specific risks, policy attention seems to be heavily tilted towards women in their capacity as mothers, especially solo mothers, while other life-cycle risks that women face, such as poverty in old age, unemployment or employment injury, are much less visible. To advance gender equality, both the design and delivery of social protection need to be cognizant of the full range of life-cycle risks and wide-ranging structural impediments women face, permeating through families, economies and societies.
Drawing on diverse country experiences, this paper demonstrates promising policy action for making social protection policies and strategies more gender-responsive and transformative. Social protection can provide women – across diverse economic and employment situations, life-cycle stages, family types and other socio-demographic characteristics – with protection against poverty and a foundation for a decent standard of living, contributing to enhanced capabilities, agency and full participation in economic and social life. Realizing this potential is contingent on creating powerful synergies between social protection and labour protection, between transfers and services, and between social protection and other policies, especially employment, health, care, formalization and fiscal policies.
Gender inequalities in labour markets have important implications for women’s access to social protection and the level of benefits they can expect to receive. This is particularly relevant for social insurance schemes, where the level of cash benefits is often calculated based on past earnings and length of contributing periods. Women’s lower labour force participation, lesser average earnings and limited access to high-quality employment, coupled with broader societal disparities, including the unequal distribution of unpaid care work, limit their opportunities to regularly contribute into social insurance schemes in the way that men often do.
Much of the social protection policy literature has been focused on the gender impacts (and gendered assumptions) of social assistance programmes but, while important, this is also restrictive and risks siloing women into a “charity” mode. This paper takes a broader perspective and explores how women’s access to social insurance schemes can guarantee higher levels of income security, considering that they provide greater policy space for risk-sharing and redistribution compared to private insurance, occupational or sector-specific schemes, or the employer-liability models that are prevalent in many countries.
For these reasons, the paper discusses how countries can build universal social protection systems with a good mix between contributory and non-contributory benefits, to extend social protection coverage to those who are not yet adequately covered. Such a system can compensate for interrupted periods of paid work and low earnings, benefiting women and carers but also others working in short-term, seasonal, part-time and multi-employer employment and self-employment. Employers benefit from a healthier, more productive workforce, delivering dividends for the whole of society. Together, social insurance schemes and non-contributory social protection schemes can plug coverage and adequacy gaps, ensuring that women have at least a basic level of social protection and enjoy social protection rights that are anchored in national legislation and provide predictable and adequate benefits.
The paper also identifies key design considerations that can promote gender equality and ensure responsiveness to gender-specific risks across the life cycle.
Across all branches and risks
-
Universality of coverage. Legal frameworks, policy design and delivery mechanisms ensuring that everyone is covered, by paying attention to barriers that arise from intersectional discrimination.
-
Adequacy. Establishing minimum guaranteed benefit levels for a dignified life (a social protection floor) and ensuring adequate benefits for as many people as possible, as soon as possible.
-
Comprehensiveness. Covering the full set of life-cycle risks to ensure protection over the lifetime and avoid the compounded impact of life contingencies on women’s income, health and well-being.
-
Inclusive delivery mechanisms. Designing and delivering benefits in a way that removes barriers to access and corresponds to women’s (indeed everyone’s) lived realities, including those with disabilities.
-
Disability-inclusive benefits. Designing benefits by taking into account the extra cost of disability, including the opportunity cost of unpaid care work provided; making disability determination and assessments easily accessible and affordable for women, as well as being accurate, reliable and independent; and not conditioning benefits on proof of people’s incapacity to work, especially women with disabilities, who face even greater discrimination in accessing labour markets.
-
Coordination with other policies. Coordinating social protection benefits with a wide range of services, such as education, health, employment services, childcare and long-term care, as well as other social services, such as those addressing violence against women.
Protection against healthcare costs
-
Removing financial barriers to accessing a comprehensive range of healthcare services, something particularly important for women as they are less likely to have an income of their own, or to control how money is allocated within the household, while they also usually take on a disproportionate share of care for sick family members.
-
Ensuring entitlement to a full range of health interventions in social health protection benefit packages, including maternity care and sexual and reproductive services, with special attention to ensuring access for women with disabilities, the rights of women and adolescent girls, and long-term care and interventions for women with disabilities.
-
Instituting supply-side investment in the health sector infrastructure and workforce, to ensure the removal of social and geographical barriers and the delivery of non-stigmatizing and woman-centred health services.
Protection for children and families
-
Harnessing the role of child benefits to address structural gender inequality, while improving children’s development and well-being, thus helping all children, especially girls, to realize their full potential.
-
Paying gender-based increments that offer higher benefit levels for girls than for boys at the onset of secondary school in countries where the risk of girls dropping out of school is highest.
-
Providing child benefits beyond compulsory schooling and well into early adulthood to support the transition from education to work, when young women are often at a disadvantage, as seen in higher Not in Education, Employment, or Training (NEET) rates in many countries.
Protection for persons of working age
-
Moving away from employer-liability provision towards an adequate mix of social insurance and universal provision that ensures collective financing and risk-sharing among employers and workers, and can provide more reliable income protection while avoiding discriminatory effects.
-
Extending coverage to those not yet sufficiently covered, aiming for adequate coverage for workers in all types of employment, including temporary, part-time and self-employment, and facilitating transition from the informal to the formal economy through an integrated approach to social protection, employment and fiscal policy.
-
Allowing for shorter or interrupted contributory periods within social insurance schemes when determining eligibility for benefits, and ensuring that contribution rates are commensurate with contributory capacities while guaranteeing minimum benefit levels that are adequate and effectively support decent living conditions.
-
Ensuring adequate maternity protection as part of a comprehensive family policy portfolio that also includes paternity and parental leave benefits, to combat discriminatory gender norms and encourage more equal distribution of care responsibilities while also recognizing women’s need for income support and rest at the last stages of pregnancy and during and after childbirth; as well as pooling financing for maternity protection across enterprises and sectors to avoid placing an undue burden on female-dominated sectors and prevent discriminatory effects (in the hiring of women).
-
Strengthening access to adequate sickness benefits to protect people’s health and incomes, including when taking care of sick family members.
-
Reinforcing unemployment protection to ensure income security and better job-matching, linked with skills development, public employment services and active labour market policies.
-
Ensuring that employment injury protection and OSH policies respond better to the occupational risks that women workers are more likely to face, especially in care-related service occupations, as well as the risk of violence and harassment across all sectors.
Social assistance
-
Social assistance has an important role to play in preventing and reducing vulnerability among all groups, including women. However, there is considerable scope for making social assistance programmes across the world more gender-responsive and centring them on the human aspects.
-
Too many components of social assistance constrain women’s freedom and can be acutely insensitive to their needs. Moreover, too often its design is punitive, imposing high transaction and compliance costs, and with eligibility and enrolment conditions that make entitlements difficult to access and often stigmatizing as well. Moreover, payment modalities do not take into account women’s individual circumstances when calculating their benefit needs; nor do they always give women direct access to entitlements, as payments sometimes go to male “heads of household”.
-
The following are some of the ways the gender-responsiveness of social assistance programmes can be enhanced:
-
benefits are available on demand and have clear and simple eligibility criteria;
-
benefits are calculated and determined based on women’s financial situation and needs rather than overall household circumstances;
-
benefit administrators are properly trained to deal with women’s different circumstances and needs, especially those who experience domestic violence or discrimination because they are from indigenous communities, for example; such actions would reduce the risk of benefits not being taken up;
-
benefit payments comprise individualized payments to women and not household heads;
-
entitlements that are conditional on the performance of public work should offer decent work rather than the low-quality, low-paid labour often involved;
-
in circumstances of systemic discrimination, gender-based increments are included.
-
-
Conditional cash transfer programmes, a prevalent form of social assistance often targeted at women in their role as mothers, have shown positive results. To move towards rights-based social assistance, it is important that governments carefully assess the need for conditionalities and, where they exist, consider revising them to avoid reinforcing gender stereotypes and exacerbating women’s time poverty related to unpaid work, as well as ensuring that non-compliance does not lead to punitive measures that exclude women and girls.
Protection in old age
-
Ensuring women’s access to adequate pensions through effective measures to extend coverage and ensure adequate benefit levels, including guaranteed minimum benefits, through a combination of well-coordinated contributory and non-contributory schemes that ensure universality of coverage.
-
Recognizing and offsetting the accumulated effects of unpaid care responsibilities on pension entitlements, through care credits, minimum pension guarantees and other measures that promote a more equal sharing of care responsibilities between men and women, and through the provision of public care services.
-
Assuring the provision of good-quality long-term care in a way that protects people from financial hardship, reduces unpaid care responsibilities, and ensures decent work for care workers.
The paper underscores the synergies between social protection policies and investment in accessible, affordable and high-quality services – including health services as well as childcare and long-term care services. This is required as women tend to perform the bulk of unpaid care work, caring for sick family members and accompanying them on medical visits, but are less likely than men to receive spousal care when old and/or frail. Hence, finding alternatives to family care that are affordable, accessible and of good quality is an urgent policy issue, as is the challenge of finding equitable and sustainable financing.
The fact that care services – whether they concern healthcare, childcare or long-term care – are delivered by a predominantly female workforce, often characterized by decent work deficits, draws attention to their working conditions, including access to social protection, and the need for adequate recognition and valuation of the work, considering that there is potential for creating decent employment in a dynamic care sector that is understaffed in many countries.
Given the significant potential that social protection policies show in reducing gender inequality, women’s participation in the design, implementation and monitoring of these policies is crucial. Removing barriers to women’s right to social protection requires legal and policy reforms, decisive action by States, attitudinal and normative shifts, and progressive action by employers’ and workers’ organizations, as well as other civil society actors. To ensure women’s participation in social protection policymaking, it is imperative that they play a strong role both in these organizations and in inclusive social dialogue.
Timely and robust gender data and analysis are critical to inform not only the design and implementation of social protection strategies, policies and schemes but also to monitor and evaluate their performance and outcomes. Effective policymaking requires effective monitoring. This means closing data and knowledge gaps in the provision of social protection. Policymakers can only ensure effective coverage for girls and women if they have access to high-quality data that is disaggregated by sex, age, disability, geographical location and migration status, among other things, to track progress – or the lack thereof – in reducing gender inequalities and intersectional discrimination around key indicators such as legal and effective coverage, adequacy and comprehensiveness, and expenditure, with respect to all benefits and services. Such data and information provide powerful evidence on the discrimination, disadvantages, barriers and injustices women face, and can thereby contribute to changing discriminatory norms and practices.
Fiscal constraints may explain some of the gaps between recognition of gender-specific risks and constraints and putting effective policies in place to address them. Yet the many examples cited in this paper attest to the fact that despite those constraints, policy efforts are under way, while costing studies have also shown that a gender-responsive social protection floor is affordable for most countries.
Ultimately, moving towards a world characterized by greater gender-responsive social protection will enhance women’s freedom, choices and opportunities to maximize their well-being and participation in social and economic life, and will bring multiple social and economic benefits for families, societies and economies.
Introduction
Social protection1 policies are indispensable for enhancing gender equality and realizing women’s rights, but they must be explicitly designed to do so. This potential has been clearly recognized in the Sustainable Development Goals (SDGs), especially target 5.4, which sees social protection policies as pivotal enablers of gender equality. Social protection systems can be designed to challenge rather than mirror gender inequality in the labour market and wider society, and can therefore contribute to transformative outcomes (UN Women 2018; UNDP 2021; ILO 2021j).
Yet in practice, social protection policies have not always addressed the gender-specific risks and structural constraints women face, thereby falling short of their potential. Gender analysis has shown how social policies can impact existing gender inequalities – in labour markets, in the division of unpaid work, and in social norms – to produce divergent outcomes for women, especially through family policies, provision of care services, and public employment (Karamessini and Rubery 2013). While initially concerned with institutionalized welfare states, over the past two decades the analytical scope of this literature has been extended to the rest of the world, showing the challenges social protection policies face in reducing gender inequalities in contexts where labour markets are gender-segregated and extensively informal, where social services are patchy and underfunded, and where social protection systems provide limited coverage. As a result, the onus of social protection is placed on families and communities, invariably placing women at a disadvantage (Razavi and Staab 2018).
The coronavirus (COVID-19) pandemic and its socio-economic impacts exacerbated existing gender inequalities in employment and social protection, as well as in health, care and intimate partner violence (UN Women 2021a; ILO 2021j). And yet social protection responses have remained surprisingly blind to gender-specific risks and inequalities, even as the gendered fallout of the crisis was shown to be enormous.
Research on high-income countries finds that despite the disproportionate impacts of the pandemic on women’s livelihoods and ability to engage in paid work, policy approaches in the form of job retention schemes (JRS), for example, were insufficiently gender-responsive, while lack of a more comprehensive policy package left the gendered division of unpaid work unchallenged (Cook and Grimshaw 2020).2 Evidence from a wider range of countries (UNDP and UN Women 2020), likewise, shows that of a total of 3,099 social protection and labour market measures adopted by 221 countries and territories between March 2020 and September 2021, just 380 (12 per cent) aimed explicitly to strengthen women’s economic security through cash or in-kind support, training or entrepreneurship opportunities. Support for unpaid care was even more limited, with only 225 measures (7 per cent of the total) adopted across 93 countries, mainly in the global North, supporting unpaid care work; the remaining 128 countries and territories did not register any response in this area (Staab and Tabbush 2022).
In addition to discrimination on the grounds of gender, certain women face multiple disadvantages by virtue of falling also into other groups with increased risk of exclusion or vulnerability, such as disability, ethnicity (e.g. indigenous groups), location (e.g. rural populations), age and marital status. Migrant women workers, for example, need access to healthcare without hardship, and protection in cases of maternity and violence. However, they often experience barriers in accessing the benefits they need owing to the under-regulated nature of the sectors in which they work (e.g. domestic service, agriculture), marked by lack of occupational health and safety, and are often excluded from contributory social insurance schemes that provide maternity protection and healthcare, because of regulations on residency requirements and/or duration of employment (UN Women 2020a).
Drawing on diverse country experiences, as well as international social security standards and principles, this paper will show promising pathways for making social protection policies and strategies more gender-responsive and transformative and better able to provide women – across diverse economic and employment situations, life-cycle stages and family types – with a secure route out of poverty and a foundation for a decent standard of living, while enhancing their capabilities and agency. Realizing this potential is contingent on creating powerful synergies: between social protection and employment protection, between transfers and services, and between social protection and other policies, especially care, employment, formalization and fiscal policies.
The rest of the paper outlines the ILO’s perspective and approach to enhancing the gender-responsiveness of social protection anchored in international social security standards and underlines the critical interconnections and need for coherence between social protection policies and other policies. It provides new data and underlines remaining data gaps that need to be urgently closed, and aims to encourage social protection policymakers, social partners and other stakeholders everywhere to think more systematically about the gender content and impact of social protection to promote gender equality.
How and why do gender-specific risks and vulnerabilities matter for the design and delivery of social protection?
To advance gender equality, both the design and delivery of social protection need to be cognizant of the wide-ranging structural impediments that women face, running through families, economies and societies. The structural inequalities are multifaceted and include socio-economic disadvantages that we discuss in this section, as well as lack of bodily integrity and autonomy, and limited voice, agency and participation in decisions that affect their lives. In this section we provide an overview of the key institutional arenas and gender fault lines that hamper women’s income security and access to healthcare and other social services, most notably gender-based barriers to (and segregation in) employment, as well as gender inequalities in unpaid work, including care work. These structural impediments must be seen alongside gender-specific risks and vulnerabilities that need to inform the design and delivery of social protection policies. This means that social protection design needs to take into account women’s life-course risks and vulnerabilities and respond to their specific needs and interests. At the same time, as noted above, gender is highly intersectional with other characteristics: class, rural/urban location, ethnic grouping, and migration and disability status, among others. While these intersecting inequalities are increasingly recognized in the policy literature, they are not adequately captured through data sources, nor do they systematically inform policy design and implementation.
Although many of these elements will become clear in the following sections, it is useful to begin with a more overarching analytical discussion on why we need a gender lens, and why social protection policies, even if they reach women, cannot be assumed to be gender-responsive by default, highlighting the need for much better data than is currently available. At the international level, there are serious gaps in the availability of sex-disaggregated data on effective coverage, as shown in figure 1.1. Especially in the area of healthcare, only 18 per cent or 23 of 128 countries have sex-disaggregated data on effective coverage. If we are to better understand the nature of provision for women, these stark data gaps need to be addressed, requiring new methodologies and data collection efforts.
Figure 1.1. Availability of data on social protection effective coverage, disaggregated by sex, by social protection function and by number of countries and territories, 2023
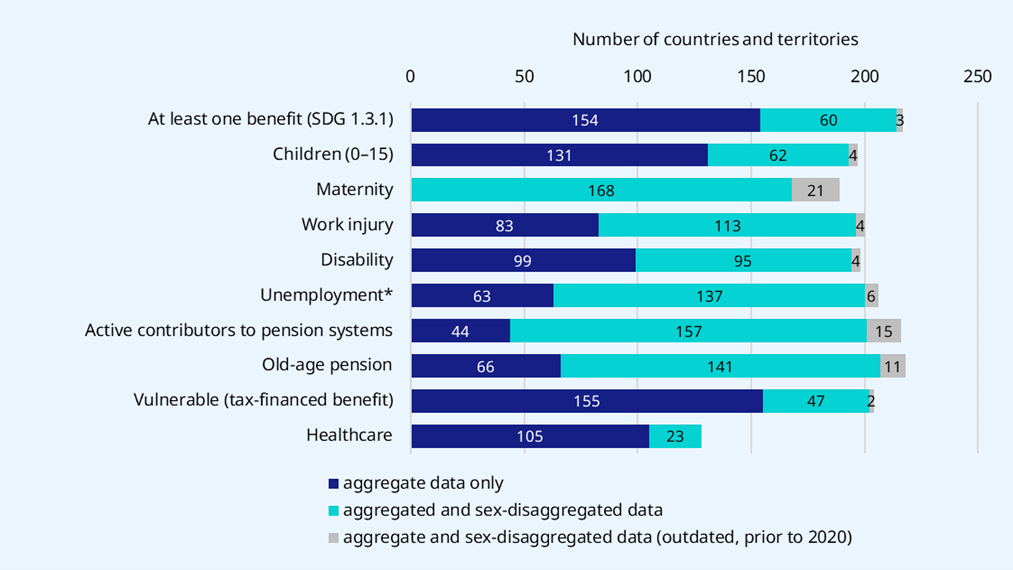
* Including 104 countries with no unemployment protection programmes, where the coverage was estimated as "0" for both men and women.
Source: ILO World Social Protection Database: https://www.social-protection.org/gimi/WSPDB.action?id=15.
1.1 Gender-specific risks and vulnerabilities
Social protection systems are built “to assist the population with a series of life contingencies or risks” (Cichon et al. 2004, 1). How well do they respond to gender-specific risks, for example the risk of child marriage that scars the lives of millions of young girls by compromising their fundamental freedoms and sexual and reproductive health and rights, and their chances of completing schooling? In some cases (e.g. Bangladesh, Mexico), child-related transfers have been used to redress the disadvantages that girls face in terms of secondary school attendance, by providing higher transfers for them than for boys at the start of secondary school, when the risk of girls dropping out is at its highest.
The transition from school to work can also be difficult for young women. Young women aged 20–24 are more likely than young men in the same age group to be Not in Education, Employment or Training, referred to as NEET status. There is good reason, therefore, to extend child benefits to young people aged 18 and older if they are enrolled in further education or vocational training, and even if they are in part-time work, to provide some income support to help them acquire the skills and experience needed to navigate the school-to-work transition. Particularly in contexts where social norms reinforce domestic and caring roles for women, such a policy, together with some income support, would send a signal to young women that they can pursue different life choices through higher education and training, which improves their employment prospects.
Intimate partner violence, which is experienced by one in three women across their lifetime, is another gender-specific risk that blights the lives of millions across the world. It has serious and enduring impacts on women by detrimentally affecting their health, well-being, educational outcomes and economic prospects (UN Women 2019a). Women’s ability to engage in paid work may be limited where there is violence and abuse, and if they are engaged in paid work, experiences of violence can lead to employment instability and lost earnings (Duvvury et al. 2013).3 At the same time, economic insecurity and women’s financial dependence on intimate partners can in turn become a driver of intimate partner violence.
Despite the interconnections between intimate partner violence, violence and harassment in the world of work, and income insecurity, efforts to make labour laws and social protection systems responsive to the risk of violence are few and far between (e.g. Uruguay’s 2017 law on gender-based violence,4 Albania’s social assistance scheme). These can, for example, give survivors of violence the right to receive full payment of their wages or cash transfers for the time spent attending hearings or other administrative or judicial proceedings related to their case, and seeking healthcare (UN Women 2023a). Women also tend to be disproportionately victims of forced labour and trafficking. Undoubtedly, adequate social protection can play an important role in reducing, ex ante, the risk that vulnerable groups face in being pushed and pulled towards the purveyors of forced labour (for example, unscrupulous moneylenders). However, it is also crucial for the survivors of forced labour to have access to mainstream social protection systems and additional support in countries in which they have sought protection, as is the case in the United Kingdom (Government of the United Kingdom, 2022).
Another risk that women face is having young children in their household in the absence of a partner who can contribute to the children’s care and financial upkeep. Indeed, the majority of single-parent households are headed by women, and they are also more likely to be poor than those where mothers live with a partner or spouse, reflecting the difficulty of combining family responsibilities with earning an adequate income. As shown in figure 1.2, without social transfers more than half of single mothers and their children would be living in poverty across a range of countries. What the figure also shows is that without exception, social transfers are essential for reducing poverty among single mothers in all countries, although the impact varies.
Figure 1.2. Poverty rates among single mothers, pre- and post-transfers: Percentage of single mothers, persons aged 18 or above, 2018–20
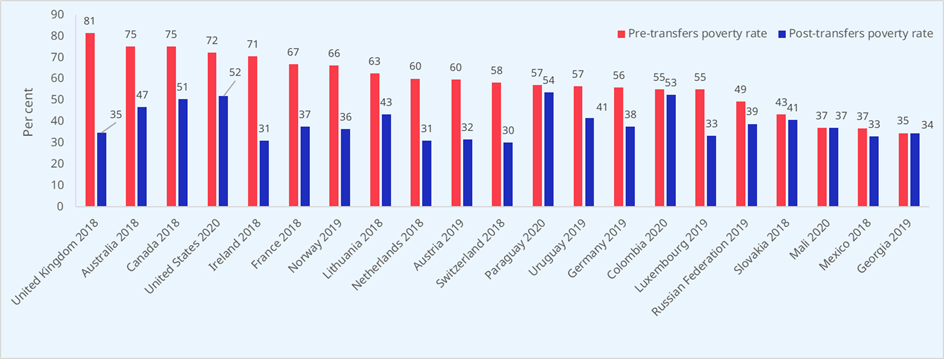
Note: Pre-transfers poverty rates are calculated using adjusted market income. Post-transfers poverty rates are calculated using adjusted disposable income. Adjusted market income includes income from earnings and occupational pensions. Adjusted disposable income includes income from earnings, occupational pensions and social transfers (e.g. state old-age and survivors’ benefits, unemployment benefits, short-term sickness and injury benefits, child-related benefits and family leave benefits). The adjusted income equals the unadjusted income divided by the square root of household size. Both market income and disposable income are net of income taxes and social security contributions. The poverty line is set at one half of national median equivalent disposable income among all persons aged 25–54.
Source: ILO calculations, based on the Luxembourg Income Study (LIS) Database: https://www.lisdatacenter.org/our-data/lis-database/.
Finally, ageing has specific implications for women, as they tend to live longer than men, experience greater morbidity, and have lower income and fewer assets, such as land, to their name. In view of persistent gender wage gaps and women’s typically lower lifelong earnings, linked to differences in their life courses and employment histories, the type and design of pension systems matters hugely for whether they are able to enjoy income security in old age. Income security in old age through a pension should be complemented by access to appropriate healthcare and long-term care services without financial hardship. Models of long-term care that rely exclusively or predominantly on families and volunteers are likely to be both inequitable and unsustainable, given changes in family structures and employment patterns. Affordable and good-quality long-term care services provide an alternative to unpaid care provided by family members, predominantly women, who form the invisible backbone of long-term care systems. Social protection systems need to assume greater responsibility so that those who need long-term care can access it without hardship.
In addition, women and men have both common and specific health needs throughout their life course. Women have specific sexual and reproductive health needs and are also more at risk of certain conditions, such as HIV transmission or dementia in old age. While removing financial barriers (in the form of out-of-pocket payments) to access healthcare is critical for both women and men, social health protection is particularly important for women as they are less likely to have an income of their own and more likely to face costly health conditions related to pregnancy, childbirth and other sexual and reproductive health needs. In addition, they often bear responsibility for seeking and often financing the healthcare of their children. Making the necessary health services available to women requires an array of policies, including reinforcing service availability, quality and acceptability, but also addressing the many barriers to access they can face, including the lack of female healthcare providers, and staff who may not be adequately trained to deliver services in a non-coercive manner while respecting privacy and confidentiality (see section 6).
1.2 Gender segregation and inequalities in employment
Across the world, labour markets are marked by persistent gender segregation and inequalities which constrain women’s access to earned income and impair their income security and effective access to healthcare and other social services. Even before the COVID-19 pandemic, progress in closing the global gender gap in labour force participation rates had stalled, and occupational segregation and gender wage gaps were pervasive.
The pandemic dealt a heavy blow to women’s employment prospects and income security. Globally, women were disproportionately hit in terms of job losses, largely because lockdowns affected sectors in which they were highly represented, most notably manufacturing and services, aggravated by their role as default care providers for their families. Between 2019 and 2020, the employment-to-population ratio for women declined by 2.5 percentage points, which is unprecedented (ILO 2021c), with serious implications for their economic security and access to adequate social protection for years to come. Workers in the informal economy, among whom women are disproportionately represented in most regions, were hit particularly hard by the pandemic and associated containment measures, due to their lack of access to income and health protection (ILO 2020c).
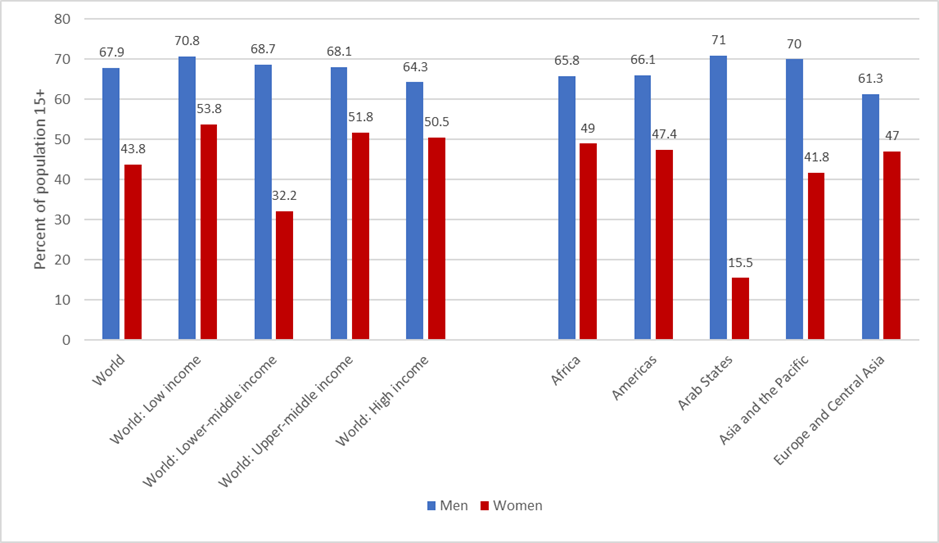
While women have gained greater access to labour markets and decent employment in many parts of the world over the past decades, data from 2022 shows that employment rates for women have still not yet fully recovered to pre-pandemic levels (ILO 2023f) and their participation in employment still lags more than 20 percentage points behind men: on average, employment-to-population ratios for women stand at 43.8 per cent compared to 67.9 per cent for men, with significant variations across world regions and country income groupings (see figure 1.3). Women’s participation in employment is particularly low in the Arab States (15.5 per cent of women compared to 71.0 per cent of men), and in lower-middle-income countries (32.2 per cent of women compared to 68.7 per cent of men), resulting in a large gap between women and men, which has implications for women’s current and future income security. Women with disabilities are less likely to be employed than men with disabilities and persons without disabilities in all regions. The gap between women and men with disabilities varies from 6 percentage points in Europe to 26 percentage points in Central and Southern Asia (UN 2019).
Figure 1.3. Employment-to-population ratio by sex, 2022
Source: ILO modelled estimates.
In addition to their lower participation in employment than that of men, women are also structurally disadvantaged in terms of their employment situation, with lesser lifetime earnings and a lower opportunity to affiliate and contribute to social insurance, which together compromise their current and future income security. Occupations and industries with a high concentration of women are characterized by low wages (ILO 2018c). Across the world, women continue to earn 18 to 22 per cent less than men, and in many countries the largest part of the gender pay gap cannot be explained by differences in the attributes and characteristics of women and men, such as their levels of education (ILO 2018c; 2022c). These labour market disadvantages are aggravated in the case of mothers – the “motherhood penalty” (see subsection 2.2 for more detail). The presence of young children in the household lowers women’s employment rates considerably, while fathers’ employment rates are either unchanged or even higher (UN Women 2019a; ILO and OECD 2020). Mothers also bear a significant penalty in terms of wages while, for most men, fatherhood results in a wage “bonus” (Budig 2014; Budig and England 2001).
At the same time, in all G20 economies with available data, the share of employed women who are working part-time is much greater than the corresponding share for men; this should be seen alongside the fact that women are more likely than men to be working fewer hours than they wish to, indicating that part-time employment may not always be voluntarily chosen (ILO and OECD 2020). Temporary employment is also more common among women than among men in many of these countries (ILO and OECD 2020). As will be seen later, while social protection coverage gaps tend to be more significant for those working part-time and on temporary contracts, this is not always the case; the design of social protection policies makes an important difference (see section 2).
Considering labour market characteristics in a wider range of countries, while informal employment is a greater source of employment for men than for women (63 v. 58 per cent) at the global level, in developing countries the proportion of female workers who are informally employed (92 per cent) is substantially higher than that of male workers (87 per cent) (ILO 2018c). This is because women are more often found in the more vulnerable situations than their male counterparts, for example as contributing family workers, for different reasons, including lack of adequate childcare services. The predominance of informal employment, especially for women, places considerable constraints on their access to social protection as well as the adequacy of their benefits, while creating gaping holes in social protection systems.
However, as sections 2 and 3 will show, these existing impediments are not insurmountable. In fact, many governments have extended social protection to workers in the informal economy through both contributory (typically social insurance) and non-contributory mechanisms. This includes reforms to extend social health protection to all (e.g. Rwanda, Thailand, Viet Nam), efforts to simplify tax and social security contributions for micro enterprises and own-account workers (e.g. so-called monotax mechanisms in Uruguay and Argentina, comprising a single payment covering both taxes and contributions), and extending unemployment protection through social insurance schemes to domestic workers (e.g. Mexico, South Africa) (ILO 2022e). Given that, in developing countries, most women are employed as own-account or contributing family workers in farms and businesses (representing 82 per cent of all women in informal employment), particular attention needs to be paid to decent work deficits, low and volatile incomes, limited contributory capacity, and lack of an obvious employer, which imposes a double contribution challenge (ILO 2021h).
1.3 Unpaid care work: Feminized, invisible and yet essential
The above-mentioned gender stratifications in labour markets are closely intertwined with gender inequalities in unpaid care work. All human beings need care to grow, flourish and become productive workers and members of society, to preserve and restore their health, live with chronic illnesses or disabilities, or enjoy healthy and dignified ageing. Care encompasses all the activities that develop and preserve a recipient’s human capabilities (such as physical and mental health as well as cognitive and emotional skills) through face-to-face interactions with a care provider. Beyond these nurturant relations, also called direct care, other indirect activities that support caregiving, such as preparing meals, housekeeping or other forms of unpaid work, also take up a considerable amount of time (Razavi 2013).
The social, religious and cultural designation of women as carers has powerful normative traction, shaping social expectations as well as concrete practices that are “sticky” and often difficult to renegotiate and change. Across diverse contexts, the primary responsibility for the care of children and adults is routinely assigned to women and girls, as an activity and a preoccupation seen as quintessentially feminine. It is often a non-negotiable part of being a mother, wife or daughter. Globally, women do three times as much unpaid care work as men do, though gender inequalities vary across countries and are particularly stark in developing country contexts (UN Women 2019a). Living in a rural area, in a poor household, being married, and having young children, all increase women’s unpaid care workloads (UN Women 2019a). This is because the burden of underdevelopment (i.e. lack of access to clean water, lack of health and education facilities, lack of reliable energy sources, etc.), including in crisis situations, falls disproportionately on women and girls. While data on unpaid care work performed by women with disabilities is scarce, evidence suggests that they are more likely to be engaged in unpaid care work than women without disabilities (UN 2019).
Typically, unpaid care has been treated as a free resource, and not considered to have economic value in conventional economic thinking, or counted in measures such as GDP (Folbre 1994). However, unpaid care generates immense value – affecting people’s well-being and society’s economic prospects – without which the global economy would grind to a halt (Heintz 2019). According to UN Women (2020b), the actual value of this work amounts to 9 per cent of global GDP – equivalent to US$11 trillion. Although the provision of care is essential for human well-being and economic prosperity – constituting the invisible foundation on which all economic activities stand – its performance imposes costs on those who provide it, in the form of financial obligations, lost opportunities to determine the nature and content of one’s life, and forgone earnings.
The fact that women carry a disproportionate share of this work impacts their employment prospects, including the type of work they are able to take on, especially when they have young children. New ILO estimates show that in 2023, 748 million people aged 15 and above were outside the labour force due to care responsibilities, of whom 708 million were women and 40 million were men (ILO 2024f). A five-country study on the impact of childcare responsibilities on the earnings of informal workers showed that women were more likely to take on insecure, flexible and irregular work so that they could care for their children while trying to earn an income (Alfers 2016). This constrained the choices available to them, often entailing significant knock-on effects on their lifetime earnings and entitlements to adequate social protection.
As the feminist economist Diane Elson (2005) puts it, the fact that much unpaid care work “is done for love, does not mean that we always love doing it”. The context and conditions under which people care for each other, and the types of support they can rely on – from partners and other household members, social protection benefits and services, and basic infrastructure such as tap water, clean energy and public transport – are of enormous significance.
Pivotal questions with respect to gender-responsive social protection rights include: Do social protection systems take into account people’s responsibilities for the care of others? And do they do so in a way that recognizes care as a shared responsibility of women and men, for example by proactively reserving a non-transferable portion of parental leave for fathers, or by providing paternity benefits alongside maternity benefits? Do pension systems recognize the time that is allocated to caring for children or others who need care, through care credits in social insurance for both women and men, as called for by the International Labour Conference in its General Discussion on Decent Work and the Care Economy (ILO 2024e)? Likewise, are sufficient investments made in affordable, accessible and high-quality healthcare, long-term care and childcare services that are adapted to the needs of working parents, which research shows can vastly improve women’s employment prospects?
How can social protection systems deal with gender-based inequalities in labour markets and employment?
Social protection systems need to respond to gender-based inequalities in the labour market and in employment, and contribute to redressing them. While social protection policies alone cannot offset all inequalities produced through the functional distribution of income between labour and capital and the functioning of labour markets, they are an essential element of a broader policy package to address these inequalities in a more structural and transformative way. This section will therefore look in greater detail into employment patterns and their impact on women’s access to social protection and discuss the policy implications for creating more gender-responsive social protection systems.
2.1 Implications of unequal employment patterns for women’s access to social protection
Gender inequalities in the labour market have important implications for women’s access to social protection and the level of benefits they can expect to receive. This is particularly relevant for social insurance schemes, where benefit entitlements often depend on past work and earnings trajectories and contributions. Women’s lower labour force participation, lower average earnings and limited access to high-quality employment, coupled with broader societal disparities, including the gendered distribution of unpaid care work, limit their opportunities to regularly contribute into social insurance schemes (if these are available). This in turn prevents them from accessing income protection and healthcare when needed. Research on women’s unequal access to social protection has focused on pensions (e.g. Arza 2012; 2015), for which comparatively good gender-disaggregated data is available, as further elaborated in section 5. Recent evidence shows that while, globally, 40.9 per cent of working-age men contribute to an old-age pension scheme, this is the case for only 29.1 per cent of women (see also section 5 and in particular figure 5.2 below).
The combined effect of shorter or fragmented contribution histories and lower earnings often results in lower pensions for women than for men. For example, a recent ILO report finds that the gender gap in the level of pension benefits in Viet Nam is 19.8 per cent (ILO 2021a). Across selected OECD countries, pension transfers to women aged 65 and over were, on average, 25.6 per cent lower than for men, with differences above 40 per cent in Japan, Mexico and Austria (OECD 2021) (see also section 5 below).
In a similar way, women’s access to unemployment, maternity and other benefits also depends on employment patterns, including high levels of labour market informality, weak employment policies and services, and a lack of coverage for those in short-term, seasonal, part-time and multi-employer employment and self-employment. Policies and services need to explicitly address women’s labour market risks, which are often aggravated by their family responsibilities, making their connections to the labour market tenuous.
2.2 The case for gender-responsive social insurance
Although social insurance mechanisms are often criticized for mirroring gender inequalities in the labour market and employment (see Arenas de Mesa and Montecinos 1999), they do play a very important role in ensuring women’s access to adequate social protection, especially when they are designed and implemented in a gender-responsive way.
In addition to lower labour force participation (see section 1), gender inequalities in employment patterns have implications for women’s access to social insurance. As employees are generally considered to have relatively good access to social protection compared to self-employed workers, a nuanced analysis is necessary to capture the heterogeneity of this group and assess the impact of policy design (see below). The proportion of women in wage employment (employees) varies from 12 per cent in low-income countries (half the rate of men) to 90 per cent in high-income countries (slightly higher than for men) (figure 2.1).
Figure 2.1. Employed population by status in employment and by sex, 2021
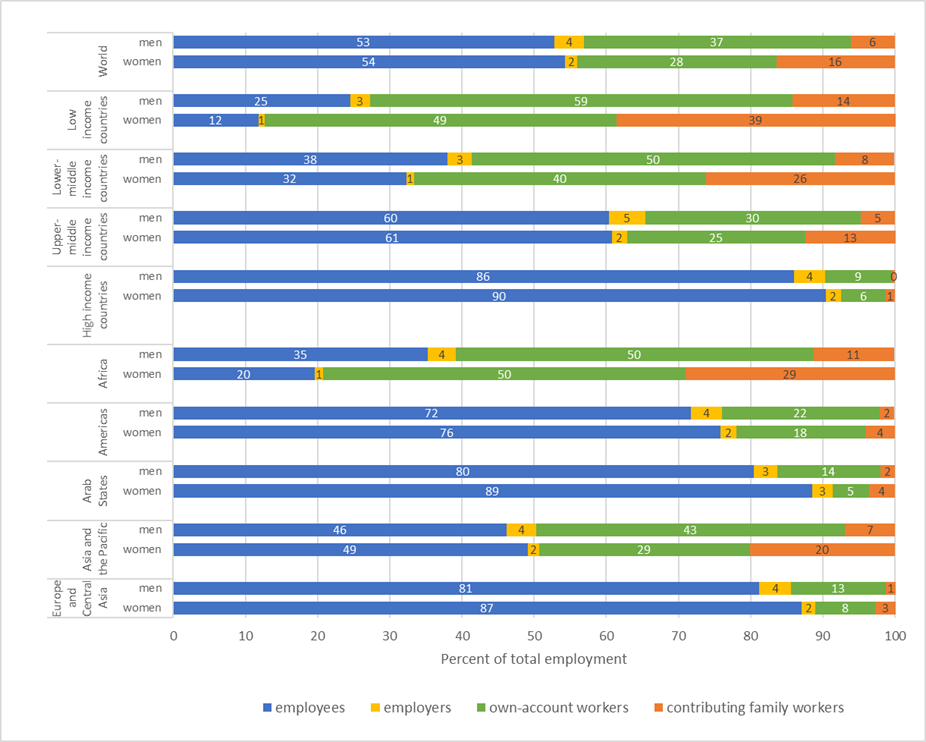
Source: ILO modelled estimates.
As far as self-employment is concerned, economically active women in low- and lower-middle-income countries are more likely to be self-employed than men; the opposite is true in high-income countries. In low-income countries, as many as 88 per cent of economically active women are self-employed; of these, 49 per cent of the total are own-account workers, 39 per cent are contributing family workers and only 1 per cent are classified as an employer (figure 2.1). Across all country groupings, women are more likely than men to work as contributing family workers, who, as they usually neither enjoy labour and social protection nor are fully recognized as business co-owners, are generally categorized as being in informal employment (ILO 2023d). Women with disabilities are less likely to be in employment and, relatedly, more likely to work in the informal economy and to be self-employed. Also, they tend to earn lower wages than persons without disabilities.
In addition, due to the disproportionate share of unpaid care work that they take up, women are more likely to have interrupted or shorter careers, to engage in part-time work and to be compelled to undertake more precarious work so as to combine paid with unpaid work.
Part-time work is more common among women than men in the majority of countries, with only few exceptions. In some countries, such as Pakistan, part-time employment is almost nine times more common among working women than working men. In a number of countries, such as the Netherlands and Afghanistan, more than 70 per cent of women are in part-time employment, but their situation in terms of labour and social protection can be very different. While part-time employment is considered to increase labour market flexibility, its more precarious forms, particularly on-call and zero-hours work, can challenge income security and result in precariousness.
All of these factors have major implications on women’s lifetime earnings and their capacity to pay social contributions. Motherhood in particular, as already mentioned in subsection 1.1, often imposes a motherhood penalty on women in terms of both their employment rates and levels of pay (ILO 2019a; Budig 2014; Budig and England 2001). Mothers of young children are less likely to be employed than women without children, fathers, and men without children. Women with children also receive lower wages and are less likely than men, and women without children, to work in managerial or leadership positions (ILO 2019a). The motherhood wage penalty varies significantly across countries. The motherhood pay gap ranges from as little as 1 per cent or less in Canada, Mongolia and South Africa, to as much as 30 per cent in Turkey (ILO 2018c). In the United States and the United Kingdom, for example, as much as 40 to 50 per cent of the gender pay gap can be explained in terms of motherhood. Overall, on average, women earn about 20 per cent less than men across the world, with large variations between countries (ILO2018c). Ironically, low-income women, who can least afford it, bear the largest proportionate penalty for motherhood, while the fatherhood bonus largely accrues to men at the very top of the income distribution (Budig 2014). The trend is troubling. Between 2005 and 2015, the motherhood employment penalty increased by 38.4 per cent, and while mothers earn lower wages than women without children, fathers are more likely to receive higher pay than men without children: a fatherhood bonus (ILO 2019a). Employers can make a contribution to lessening the motherhood penalty by providing more family-friendly working conditions (flexitime, part-time, teleworking, etc.) as well as return-to-work policies for both women and men.
A recent ILO analysis of employment and social protection coverage patterns in Brazil, India and South Africa sheds an interesting light on how gendered employment patterns translate into access to contributory social security mechanisms (ILO and ISSA 2023; ILO 2024g, section 3.2.2).
Based on labour force survey data, the analysis identifies significant differences in social security coverage across different types of employment, using contributions to a pension scheme as a proxy for coverage (see figure 2.2). As could have been expected, pension coverage of full-time employees is higher than for part-time employees, and that of those on open-ended contracts is higher than for those on temporary contracts. What is surprising is that within each category of workers, gender differences are smaller than might have been expected, and in some cases, women are more likely to contribute than men. This is, for example, the case for both full- and part-time employees in Brazil and South Africa. This suggests that gender differentials in labour force participation may be a more important driver of inequalities in access to social security than gender differences within each category of workers.
Another important insight is that social protection policies matter. Brazil, which has undertaken major efforts to cover self-employed workers, reaches significant coverage rates for both part-time and self-employed workers, with more than one third of female and male self-employed workers covered. Further analysis could assess in more depth the impact of occupational segregation patterns and differences in the structure of employment, taking into account variations in overall labour force participation among the three countries (ILO and ISSA 2023; ILO 2024g, box 3.4).
Figure 2.2. Share of persons in employment who contribute to a pension scheme, by status and type of employment, selected countries, latest available year
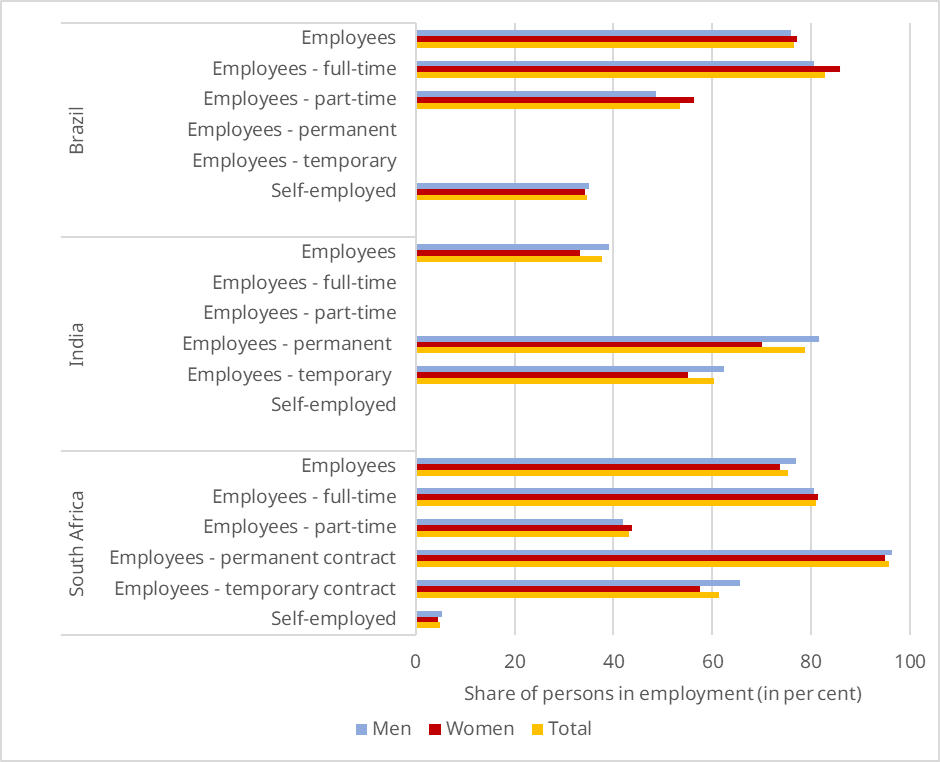
Notes: Data by contract type (permanent, temporary) was not available for Brazil or India.
Source: ILO and ISSA (2023), using own calculations based on ILO Harmonized Microdata, https://ilostat.ilo.org/, drawing on the following national sources: Brazil’s Continuous National Household Sample Survey, India’s Periodic Labour Force Survey and South Africa’s Quarterly Labour Force Survey.
Analysing the data from a life-course perspective provides further insights into the impact of employment patterns on access to social protection by age (see figure 2.3). Looking only at persons in employment, gender differentials in social security coverage are smaller than might have been expected. In India and South Africa, coverage rates for young women are higher than for men up to a certain age, yet their coverage rates drop below men’s after around 30 years in India and around 40 years in South Africa, which may point to a risk of dropping out of formal employment because of care responsibilities or cohort effects (ILO and ISSA 2023). In contrast, Brazil displays higher and relatively stable coverage rates for both women and men that are prime-age workers, and women are more likely to contribute than men for almost all age groups.
Figure 2.3. Share of persons in employment who contribute to a pension scheme, by sex and age, selected countries, latest available year (percentage)
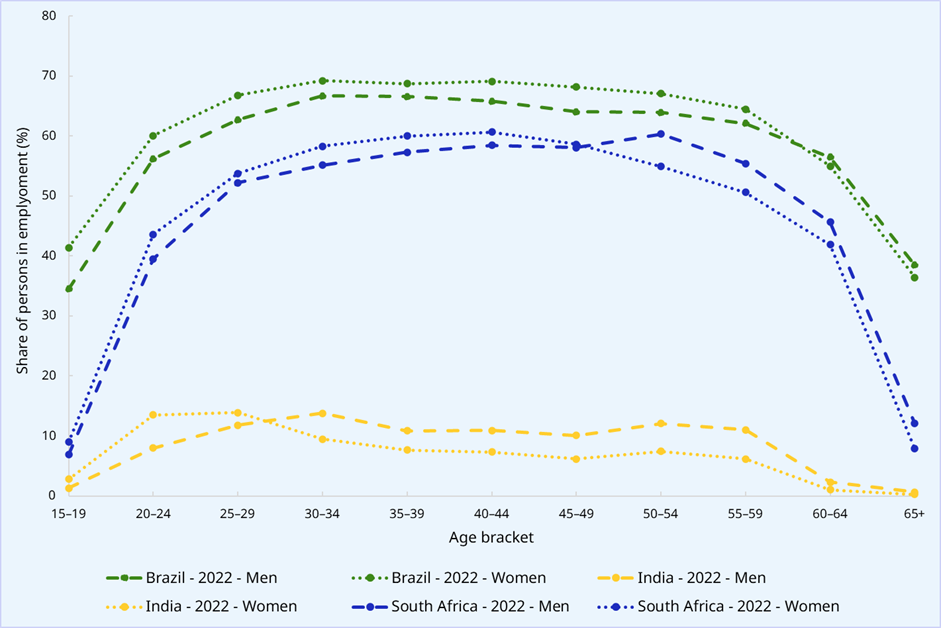
Source: ILO (2024e, box 3.2); ILO and ISSA (2023); own calculations based on ILO Harmonized Microdata, https://ilostat.ilo.org/, drawing on the following national sources: Brazil’s Continuous National Household Sample Survey, India’s Periodic Labour Force Survey and South Africa’s Quarterly Labour Force Survey.
The evidence for the three countries demonstrates the importance of a comprehensive and nuanced analysis of gender inequalities in employment and access to social insurance. It also highlights the importance of gender-responsive policy reforms to extend social insurance coverage to those who are not yet covered, across all types of employment (ILO 2024g, section 3.2.2; 2021h).
Social insurance coverage is particularly important for women, as it provides a much greater policy space and potential for broad risk-sharing, redistribution and measures to offset gender inequalities in the labour market compared to contributory mechanisms offered by the private sector (private insurance), occupational- or sector-specific schemes or employer-liability mechanisms (ILO 2021j; 2024g, section 3.2.2). For example, the link between contributions and benefits is particularly strong in defined-contribution schemes that are based on individual accounts (public or private), which do not provide scope for risk-pooling and redistributive elements, or may even include discriminatory features such as sex-specific life tables; nor do they always provide a guaranteed minimum pension should there be poor market performance which compromises future income security (Arza 2012; Behrendt and Woodall 2015; Behrendt 2000). Employer-liability mechanisms in the areas of maternity protection, sickness and employment injury, as well as severance pay, do not provide for broad risk-sharing among employers and workers, often exclude more vulnerable categories of workers, and are often riddled with non-compliance and discriminatory effects (ILO 2021j).
For these reasons, and in line with international social security standards, it is essential that social insurance schemes, together with tax-financed schemes, constitute the core of public social protection systems, while other forms of protection can play a complementary role (see also subsection 4.5). Hence, blanket calls for the decoupling of social protection from employment, resulting in the weakening of social protection mechanisms, offer a bad deal for women. Efforts would be better directed at addressing weaknesses in certain social insurance schemes for more equitable results.
How can social insurance schemes be designed in a more gender-responsive way for workers in different types of employment, given that social insurance coverage is particularly important for women?5
-
Although full-time employees with open-ended contracts tend to be relatively well covered compared to other categories of workers overall, this is not necessarily the case for all workers in this category (ILO 2023e). It is therefore essential to close remaining coverage and adequacy gaps, particularly for workers in certain sectors or occupational categories (such as agricultural or domestic workers, many of whom are women), ensure adequate coverage also in micro-enterprises, address gender wage gaps and enhance compliance with legal frameworks, including the under-declaration of wages.
-
For part-time workers, legal minimum thresholds regarding hours of work play an important role in determining social security coverage, taking into account gendered employment patterns. Typically, those with only a few hours of work per week or month (marginal part-time work) and those working on zero-hours contracts are least likely to be covered, while those with regular working time or more hours (at least 20 or more hours per week) are often covered on a pro-rata basis. Policy reforms should therefore focus on bringing in more part-time workers under social security coverage by lowering or abolishing legal thresholds regarding minimum hours of work, while at the same time removing administrative barriers that hinder the registration of part-time workers in social insurance. Additional measures might be necessary to address the specific challenges for categories of employees who often work for several employers, such as domestic workers (ILO 2022e; 2021f).
-
For workers on temporary contracts, legal thresholds regarding the minimum length of contract required for mandatory social insurance coverage are essential. While those on contracts of several months or longer benefit from social security coverage in many countries, those on very short contracts (especially casual workers) are often excluded. Extending social insurance coverage to these workers by reviewing those legal thresholds and facilitating registration is essential. Special attention needs to be given to adapted mechanisms for seasonal and casual workers.
-
For self-employed workers, the extension of social insurance faces specific challenges, which can be addressed through adapted measures. In fact, more and more countries have extended social insurance coverage to self-employed workers, at least for some sectors and types of occupations, to ensure their access to healthcare and income security (ILO 2021g; Spasova et al. 2021). Sometimes governments decide to extend coverage on a voluntary basis, yet many country experiences show that voluntary coverage rarely leads to a significant expansion of effective coverage, especially for categories of workers with limited contributory capacities. In addition, particular attention needs to be given to vulnerable categories of self-employed workers, such as own-account workers and contributing family workers.
-
For dependent contractors, preventing misclassification of their employment relationships is critical. In some countries, specific regulations exist to ensure, where necessary, that dependent contractors are covered in a comparable way to employees. In other cases, there are no regulations differentiating between dependent contractors and independent workers in terms of social protection coverage.
While social protection schemes alone cannot remedy the entrenched gender inequities in the labour market and within the household, social insurance schemes can be designed in ways that help to narrow the gender gap (Arza 2015).
-
Comprehensiveness. The types of risks that are covered and the eligibility conditions to benefits can shape gender outcomes. Many social insurance schemes around the world still do not include the full range of contingencies. In many countries, available schemes are limited to employment injury protection, old-age, survivors’ and disability benefits and health insurance, whereas sickness and maternity benefits, child and family benefits and unemployment benefits are less common, notwithstanding their essential role for women (ILO 2021j). Despite their importance for redressing gender imbalances at home and at work, paternity leave and benefits are still only provided in a small minority of countries around the world (ILO 2021j; Addati, Cattaneo, and Pozzan 2022).
-
Coverage. Social insurance schemes with broad coverage are particularly important for women, referring to the covered population and to the eligibility criteria and related conditions. Women’s access to social protection benefits depends on the types of employment included in mandatory coverage and the conditions for inclusion, the required years of contributions to receive a benefit, and the retirement age in the case of pensions. Particular attention should be paid to addressing discrimination and disadvantages intersecting with gender, including removing barriers women with disabilities face in accessing social insurance (ILO 2024g, section 4.2.5).
-
Benefit calculation and adequacy. The way in which benefits are calculated and entitlements are defined is essential to determine the level of protection that individuals get. In earnings-related social insurance systems, benefits are calculated as a percentage of past earnings, and in some cases that percentage also depends on contribution years (for instance, in many old-age pension systems). Key features of the benefit calculation rules from a gender perspective include the reference salary, the replacement rates applied, and the rules for benefit indexation (especially for long-term benefits such as old-age and survivor pensions), as well as policies to recognize and compensate periods of care or care-related leave, and other redistributive elements for low-income contributors, such as minimum benefit guarantees (see section 4). In addition, periods of maternity, paternity and parental leave and unpaid care work are often not considered in determining the eligibility and level of benefits; yet this is essential for the full range of benefits, including health protection, unemployment benefits and old-age pensions.
Social insurance schemes that are designed in a gender-responsive and inclusive manner and include design features that aim at offsetting gender inequalities in the labour market and the gendered distribution of unpaid work in families, such as minimum benefit guarantees or pension care credits, can achieve much better results for women and society at large (see sections 3 to 7).
2.3 Are non-contributory (tax-financed) benefits a complete solution for gender equality?
In view of the gender inequalities in access to contributory forms of social protection, as illustrated by the discussion of pensions above, non-contributory (usually tax-financed) social protection mechanisms6 have attracted more interest as mechanisms to close gender gaps in access to benefits and enhance women’s income security and access to healthcare. In fact, rights-based tax-financed social protection schemes play an essential role in guaranteeing a basic level of social security for those who are not eligible for – or lack capacity to pay into – contributory schemes, among whom women are disproportionately represented (Kidd 2009; ILO 2021j; 2024g).
For example, universal or means-tested non-contributory pensions play a key role in ensuring universal coverage for pensions (ILO 2016c; 2021j; Arenas de Mesa and Robles 2024), contributing to access to personal income for older women (UN Women 2017b). However, the capacity of non-contributory schemes to fulfil their potential depends significantly on their coverage and adequacy, especially benefit levels.
While universal or categorical schemes are an effective and simple way to provide a basic level of protection to specific categories of the population (e.g. older persons), many countries provide only programmes that are narrowly poverty-targeted and often cover only a minority of the vulnerable population (UNICEF 2020; Arza 2017). Moreover, many recipients perceive the application processes for poverty-targeted benefits as opaque and stigmatizing (Walker 2014). In addition, several of these benefits are provided at the household level and, by ignoring the intra-household distribution of resources, fail to reach women who live in households classified as non-poor, even if they have no personal income and therefore lack income security. It is for this reason that schemes that provide individualized entitlements, yet are collectively financed, are better placed to protect the autonomy and income security of the individual than household benefits, whose distribution among household members is left at the discretion of the primary recipient.
In terms of benefit levels, non-contributory benefits, regardless of whether they are universal or poverty-targeted, often provide very modest benefit levels that are often insufficient to meet women’s needs, particularly in low- and middle-income countries. In many countries, the minimum level of non-contributory pensions remains well below the national poverty line (ILO 2024g, fig. 4.38). Furthermore, the eligibility criteria of poverty-targeted benefits can often result in these entitlements being difficult to access, for instance due to strict conditionalities and other requirements.
When it comes to accessing benefits in kind, such as healthcare services and social care services, some countries provide their entire population with rights-based entitlements on a non-contributory basis. When such systems are adequately financed from the government budget, they can provide financial protection against the costs of healthcare and social care services and ensure effective access for all. Malaysia, Brunei Darussalam and others have demonstrated that such efforts can contribute to the overall goal of reducing inequalities, including in accessing essential healthcare, with positive impacts on women’s health (ILO 2021e). Other countries have adopted universal national health insurance systems that pool both social security contributions and government budget subsidies in order to ensure that all are covered, based on broad risk-sharing across the population. However, many countries still rely on fragmented social health protection entitlements, relying on non-contributory mechanisms targeted at the poorest, based on proxy means tests that often provide lower-quality services and inadequately capture the social determinants of women’s health (ILO 2021e; 2024d).
Hence, when it comes to non-contributory schemes, their design and implementation and how they interact with other pension schemes within national social protection systems are key to how they impact gender outcomes. Design features, such as the target population, benefit size, duration and frequency, whether a household or individual entitlement is provided, whether or not it is subject to conditionalities, as well as delivery modalities, are all important to take into consideration when assessing the extent to which non-contributory schemes are inclusive of women (UNICEF 2020). Rights-based tax-financed schemes, whose eligibility conditions and benefit parameters are anchored in national legislation, which can rely on sustainable and equitable financing through the government budget in line with international social security standards, and which take into account gender-specific risks and vulnerabilities, provide a better deal for women than ad hoc “safety net” programmes that can lack the predictability of legally anchored schemes. At the same time, non-contributory benefits alone are often not sufficient to provide adequate protection throughout the life cycle. For this reason, national social protection systems should also include social insurance mechanisms (see subsection 2.2) to ensure women’s access to adequate social protection.
2.4 Policy design matters for gender equality
It is clear from what has already been said that well-designed and -implemented social protection systems play a key role in enhancing gender equality and women’s empowerment and opportunities, with positive impacts on their families and communities. For this, both non-contributory and contributory social protection provision needs to become more responsive to gender-based risks and needs, and work together in a more integrated way, including also by recognizing the intersection with disability. If the two operate in isolation, their ability to tackle gender inequality will be weakened.
Social protection systems and schemes that are designed on the basis of the guidance provided by international social security standards are likely to get the best deal for women in terms of their enjoyment of the right to social security (see box 2.1). This applies to social insurance schemes that include a number of features recommended by these standards, such as collective financing and risk-sharing, minimum benefit guarantees, progressive formulas for calculating benefit amounts that benefit those on low incomes, coverage of dependants in health insurance schemes, and the recognition of and compensation for periods without contributions, such as through care credits in pension systems (Fultz 2011). It is encouraging that many countries have introduced policy measures to extend contributory coverage to women and men in diverse employment situations, such as the extension of maternity and unemployment insurance coverage to domestic workers in South Africa, the extension of sickness benefits to all residents in Finland, the extension of pension coverage to a large share of the population through a mix of contributory and non-contributory pensions in the Plurinational State of Bolivia, Cabo Verde and South Africa, and the adaptation of the national health insurance scheme to self-employed workers in Kazakhstan (ILO 2021j).
When it comes to securing at least a basic level of income security in particular, non-contributory (tax-financed) social protection schemes have an important role to play. At the same time, extending social insurance coverage to hitherto unprotected categories of workers is indispensable in providing access to adequate levels of social protection for women (ILO 2021h). Contributory and non-contributory schemes should each recognize the contributions that women make to society, through both paid and unpaid work. Moreover, schemes should not be seen in isolation, but rather as constituting a system that secures universal protection across a comprehensive range of risks. When this is not the case, women tend to disproportionately fall through the cracks.
It is worth noting that social protection systems that are designed in a way that compensates interrupted periods of paid work and low earnings benefit not only women and carers but all workers. In fact, the adaptability of social insurance becomes increasingly relevant in view of ongoing labour market transformations, including for those who are outside an employment relationship. In this sense, gender-responsive social protection systems will also promote greater inclusion of workers in different types of employment as well as of different genders.
Social protection alone cannot remedy persistent inequalities (re-)produced in the labour market and in the economy. In parallel to ensuring gender-responsive design of social protection systems, urgent action is therefore needed in other areas, notably employment policies, labour protection policies and family policies more broadly, to address discriminatory practices, such as unequal pay and unequal access to labour markets and good-quality employment, as well as unequal distribution of care responsibilities within families. At the same time, social protection policies also need to pay greater attention to the availability, accessibility and quality of public services (e.g. healthcare, childcare, long-term care) to produce better outcomes, especially in supporting women’s access to decent employment opportunities and equal pay and promoting their autonomy.
Box 2.1. Why is ILO Convention No. 102 important for women’s access to adequate social protection?
Among international social security standards, the Social Security (Minimum Standards) Convention, 1952 (No. 102), stands out as the only Convention that offers a comprehensive and systematic framework of internationally accepted principles and benchmarks for national social protection systems. Yet this Convention has often been criticized for reflecting outdated labour market and family structures which existed at the time of its adoption (i.e. the male breadwinner model). While the language of this instrument may appear antiquated, a closer look at its normative substance shows that it is perfectly capable of supporting governments in designing social protection systems that are gender-responsive and transformative. The ILO Committee of Experts on the Application of Conventions and Recommendations (CEACR)7 emphasized that “the standards of this Convention are perfectly suited to an implementation based on gender equality not only due to their exhaustiveness and relevance, but also because of the universality of the right to social security” (ILO 2024a, 944). Three elements stand out:
-
The Convention addresses women’s social protection coverage in two ways: as persons protected in their own right on an equal footing with men (as workers or members of society), and as dependants with derived rights, which complement (but do not substitute for) protection in their own right.
-
The Convention refers to “breadwinners” not to promote a particular family model, but to ensure the protection of non-working spouses, taking into account the diversity of family structures. Accordingly, four fifths of ratifying States provide survivor benefits also to widowers (ILO 2024a, 944).
-
Among several options for evaluating the adequacy of benefits (most of which are formulated in a gender-neutral way), the wage-related options refer to a “skilled manual male employee” or an “ordinary male labourer”. Given persistent gender pay gaps and gender inequalities in the world of work, using men’s wages as a reference wage results in a higher minimum level of protection (i.e. higher benefit levels) applicable to all – both men and women.
While Convention No. 102 would most certainly have been worded differently if drafted today, together with other up-to-date international labour standards, it continues to provide a useful normative framework for building strong social protection systems that achieve universal, adequate and sustainable social protection, contributing to the fundamental objective of gender equality (ILO 2021d; 2019a; 2024b).
Social protection for children, tackling inequality from the start
Awareness of the need for gender-responsive social protection is increasing, yet significant protection gaps remain, particularly in lower-income countries. Sections 3, 4 and 5 consider how social protection systems that cover the full life cycle can better address women’s needs, combat discrimination and empower them. Full life-cycle systems are especially important for gender equality given the fungibility of different benefits and their tendency to be redistributed between different household members, which can be freedom-enhancing for women.
Increasing the gender-responsiveness of social protection involves tackling gender-specific life-cycle risks (see subsection 1.1) and the systemic discrimination faced by women and girls. Policymakers must also consider how crises and increasing covariate shocks worsen gender inequalities, compelling women to act as shock absorbers, skip meals, or increase unpaid work to cut expenses (Kabeer, Razavi, and van der Meulen Rodgers 2021; Fukuda-Parr, Heintz, and Seguino 2015).
3.1 Social protection for children to provide a good start in life
Making social protection for children more gender-responsive means addressing discrimination against girls and young women and recognizing the impact of childcare on adult women’s labour participation and autonomy, especially those with multiple vulnerabilities. However, the prevalence of social protection for children remains woefully low – only 23.9 per cent of children aged 0–18 are covered, leaving 1.8 billion without a child cash benefit, with sharp regional disparities in coverage. Fewer than one in ten children (7.6 per cent) in low-income countries receive a child cash benefit (see figure 3.1). Public expenditure on social protection for children needs to increase. On average, 0.7 per cent of GDP is spent on child benefits globally (ILO 2024g).
Given the well-recognized poverty reduction properties of social protection (in terms of both monetary and multidimensional child poverty), this protection gap prompts deep concern, considering that children make up more than half of the world’s extreme poor population. Today, 333 million children are still living below the extreme poverty line, 1.4 billion children are living below the higher international poverty line (Salmeron-Gomez et al. 2023) and almost 1 billion children live in multidimensional poverty (UNICEF 2021). And poverty risks tend to differ depending on family composition. For instance, they tend to be higher for children growing up in larger families or in sole-parent households.
The positive impacts of social protection for children are beyond question. Extensive evidence shows that child-sensitive social protection reduces child poverty and protects well-being (see box 3.1) while also contributing to income security in households and protecting against child labour, and it has broader significance for child health, early childhood development, education and food security (see section 4.1 in ILO 2024g). However, in the absence of social protection, these basic conditions for well-being are less likely to be met during childhood, creating lasting conditions that are difficult to rectify in later life.
Figure 3.1. SDG indicator 1.3.1 on effective coverage for children and families: Share of children receiving child or family cash benefits, aged 0 to 15 (2015 and 2023) and aged 0 to 18 (2023), by region, subregion and income level (percentage)
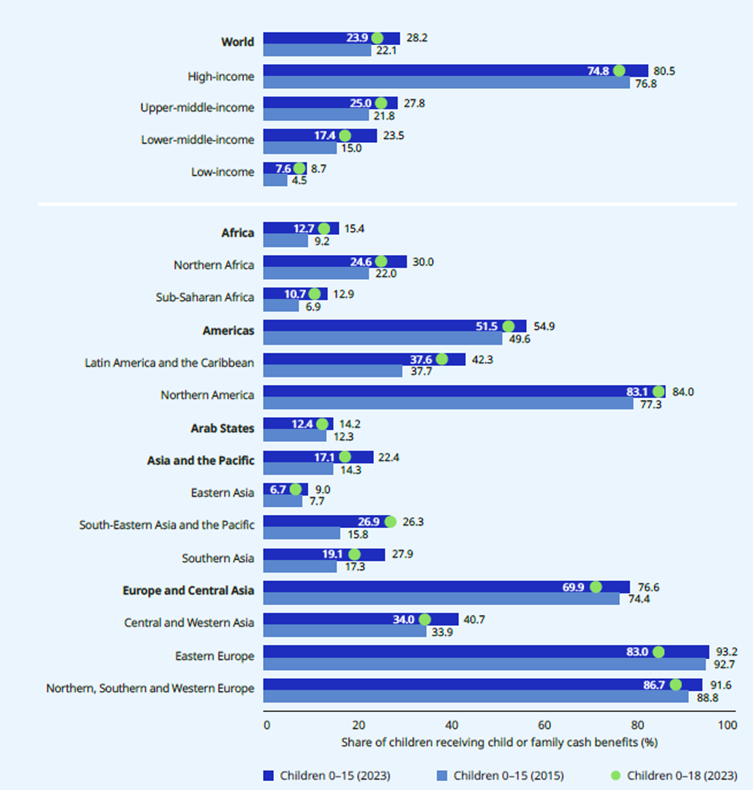
Notes: See Annex 2 of ILO (2024g) for a methodological explanation. Data for coverage of children aged 0 to 18 is available for 2023 only. Global and regional aggregates are weighted by population aged 0 to 15 and 0 to 18.
Source: ILO (2024g).
Moreover, discrimination against girls in some settings can result in lower access to nutritious meals and education for them than for boys. While access to education had begun to improve significantly for girls over the past decade, the COVID-19 pandemic is likely to have undermined some of this progress (UN Women and UNDESA 2021; ILO and UNICEF 2023). Furthermore, discrimination against adult women, contributing to a perceived lower status, also has adverse implications for child well-being and poverty (manifested through women’s lower access to education, income and household resources). The interconnections between gender inequality on one hand and child poverty and child well-being on the other are bidirectional.
Box 3.1. The power of social protection to reduce child poverty and protect well-being (selective examples)
-
Reducing child poverty. Evidence from the European Union shows that the reduction in child income poverty after taxes and social protection benefits falls into the range 36–41 per cent of market income (ILO and UNICEF 2023). And for groups that are especially at risk of poverty, such as single mothers and larger families, it contributes to significant inroads into poverty reduction (see figure 1.3 in section 1).
-
Preserving lives. Social protection can literally be a lifesaver for children and their mothers – such policies are associated with significant reductions in mortality among children under 5 and women, as well as higher life expectancy (Richterman et al. 2023; and see fig. 1 in UNICEF and Learning for Well-Being Institute 2024). Similarly, a 15-year study on Brazil’s social pension and Bolsa Família (family grant) programme shows a significant reduction in infant and child mortality (Aransiola et al. 2023), underscoring how the fungibility of life-cycle social protection is good for children.
Social protection systems interrupt the drivers of child poverty and address structural gender inequality, while improving children’s development and well-being, so helping all children, especially girls, attain their full potential. However, if social protection is to perform these functions, policymakers must get the basics of social protection right – providing protection across the child’s life course along with the wider range of services (see figure 3.2) and ensuring systems become more gender-responsive. This will better address the structural disadvantages that girls and young women face and the adverse impact the care of children has on adult women. Below, policy reform and design recommendations are advanced, with the twin objective of ensuring the general well-being of all families with children and specifically improving girls’ and young women’s well-being. These include the following:
-
Getting the basics of social protection right through core policies and principles that are good for all children and therefore girls too.
-
Closing coverage gaps with inclusive child benefits, ideally through universal child benefits (ILO and UNICEF 2023; ILO 2024g). Inclusive child benefits connect children to state institutions and ensure fairer resource distribution. Inclusivity also means undoing clearly harmful policy design – for example, problematic targeting, hard/punitive conditionality, complex eligibility criteria – that hinders children’s access to social protection.
-
Guaranteeing adequate benefit levels. For coverage to be transformative, it must deliver benefits set at values high enough to generate meaningful change in children’s lives and well-being. Higher adequacy at the right time is also crucial (for example, the first two years of life). A vast array of evidence demonstrates that adequate child benefits improve many human development indicators for girls (Bastagli et al. 2016).
-
Providing a comprehensive range of benefits covering all stages of a child's life course and different household circumstances. Examples include birth grants, tax breaks, single-parent supplements, and childcare leave. Beyond cash benefits it also means securing universal health coverage to ensure families have access to high-quality healthcare without hardship. In their absence, harmful protection gaps will persist in the child’s life course.
-
Increased expenditure, filling financing gaps and front-loading social protection spending in the early years of children’s life course to deliver the best results, through maternity/paternity benefits, parental leave, and childcare services, supported by a child benefit from birth to adulthood (ILO and UNICEF 2023; Richardson et al. 2023).
-
-
Gender-based increments can counteract discrimination against girls, correcting for gender inequality and parental bias in resource allocation. For example, higher stipends or benefits for girls can close education gaps, as seen in Bangladesh’s Female Secondary School Stipend Programme, which boosted girls’ schooling, delayed early marriage, enhanced contraceptive use thus reducing fertility, and improved employment prospects among working women. It also improved boys’ educational outcomes through sibling spillover effects (Rahman Khandker et al. 2021). Similar initiatives, like Bihar’s universal child benefit for girls, have reduced early marriage and teen pregnancy (ILO and UNICEF 2019; 2023; Kaushik et al. 2023). Such measures send a strong message to households and communities that girls are worth investing in and can be a catalyst for the long-term realization of gender equality. Better educational opportunities for girls enhance their self-esteem and life prospects.
-
Extending the upper age range of child benefits supports the formation of young women’s capabilities and their access to decent work. Currently, 123 countries8 provide statutory child benefits beyond 16 years of age,9 and 51 of these provide child benefits well into young people’s early to mid-20s. Such age-extended child benefits provide modest income security to help young women transition from school to further education or training and then work. This is especially important for young women, who face higher NEET rates than men – 31.5 per cent compared to 13.5 per cent globally in 2020 (ILO 2022b: see table 1.2). With lower employment rates coupled with social norms often pushing young women into caregiving roles, child benefits extended beyond age 16 would provide young women with vital income security to pursue education and training, improving their economic prospects and expanding their life choices.
-
Gender-responsive social health protection, including sexual and reproductive services, is essential for young women to control their bodies and life choices (see section 6). This requires confidential, respectful care for adolescent girls and their parents, and ensuring access to postnatal care, immunization and essential services. Girls and women with disabilities face higher unmet needs for sexual and reproductive care due to barriers and discrimination, including forced sterilization. Providing these services helps prevent death, disability and lifelong illness. Additionally, ensuring girls who give birth can continue their education, as in Sierra Leone, is vital for their long-term opportunities.
Getting the basics right will allow gender-specific measures to have greater traction and ensure a fairer start in life. Social protection represents an investment in girls’ and young women’s rights and potential. It can elevate their social status, autonomy and control over household resource allocation, and ultimately help maximize their full participation in socio-economic life.
Figure 3.2. A broad range of publicly provided family policies are available to improve income security and children’s well-being across the life course
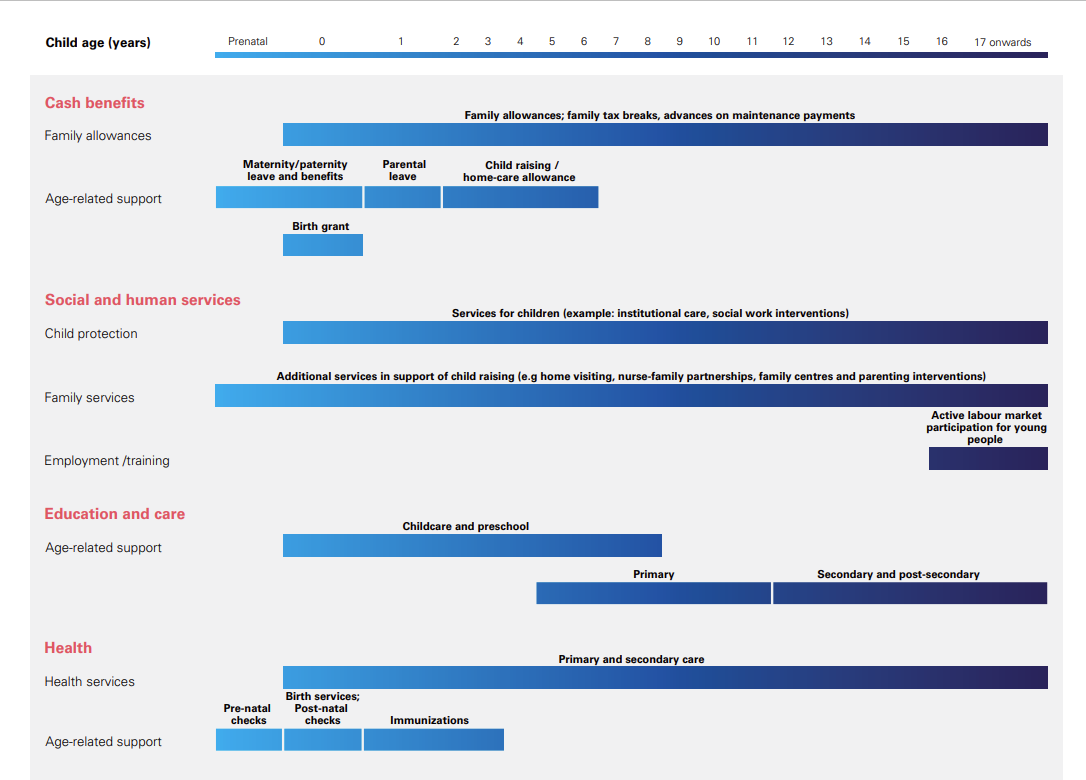
Source: ILO and UNICEF (2023).
3.2 Social protection that works for children must also work for women
The income security and well-being of children are inseparable from those of their caregivers and families. Children’s presence and care needs have a particular impact on the opportunities adult women and mothers have for participation in the labour market and in wider social life. Adults with children are more likely to experience extreme poverty than those without. Women aged 25–34 are at a higher poverty risk, as they tend to bear the opportunity costs and lower earnings synonymous with child raising. Single-parent households are especially vulnerable, balancing caregiving with limited time for paid work, further strained by the lack of affordable childcare.
Policies that focus on children have insufficiently reflected on the implications for women as mothers, caregivers or childcare workers (Razavi 2020; Staab 2019). For instance, conditional cash transfers have been criticized for reinforcing traditional gender roles while adding to women’s unpaid workloads (Bastagli et al. 2016; Cookson 2018; Fultz and Francis 2013; Molyneux 2007). There is evidence that family benefits, conditional and unconditional, can empower women and girls (Davis et al. 2016; Hunter, Patel, and Sugiyama 2021; Perera et al. 2022). However, the positive impacts of cash transfers and family benefits will not happen without incorporating the further design features discussed here into such schemes to render them more effective in combating the structural inequalities women experience.
Enhancing gender equality presupposes a corresponding investment in public services. Globally, there are significant childcare gaps affecting women. Only 32 per cent of 178 countries offer statutory early childhood educational development (ECED) programmes for children aged 0 to 2, meaning only two in ten parents have such a right (Addati, Cattaneo, and Pozzan 2022). While some countries heavily subsidize childcare, others charge fees that may be unaffordable for many. Most high-income countries provide some free childcare, but usually not before age 3, with exceptions like Belgium and Denmark (Gromada and Richardson 2021). Additionally, limited childcare hours, often suited only for part-time work, restrict parents’ ability to work full-time, increasing their poverty risk. Access is crucial for informal economy workers too (ILO and WIEGO 2020a; 2020b; 2020c).
Depending on their design and delivery, social protection schemes directed at families with children can either reinforce traditional gender roles and responsibilities or promote both children’s development and women’s economic security and empowerment, with positive implications for their households and wider society. The ultimate key ingredient in child development is the quality of parenting. Policies that enable effective parenting, free of income insecurity and with a more equally shared care burden, will promote child development.
It is no coincidence that the top 20 countries/territories in the UNDP’s gender equality index all have comprehensive social protection for families with children in the form of high-coverage and adequate child benefits, and provide maternity provision, substantial parental leave and childcare policies and comprehensive health systems too (UNDP 2022, table 5). These countries offer an important demonstration effect of the policy direction that needs to be followed to develop gender-responsive social protection systems and wider approaches to care and services.
Social protection must work both for children and for women. This requires guaranteeing the income security and well-being of families with children without imposing a further burden on women. Key recommendations that could support more equitable caregiving include:
-
Reforming contributory family and child benefit schemes to address legal exclusion and unequal treatment. Contributory family benefits in some countries still discriminate against women. This occurs through direct legal exclusion of working women, partial coverage or different treatment. Some countries insure fewer children for women contributors than for male ones, or require spousal consent to claim benefits (ISSA 2017). Legal reforms to ensure women enjoy equal treatment in terms of benefit coverage and adequacy with male contributors or other categories of workers should be a priority. Individualizing entitlements and removing partner consent criteria are also important reforms to undertake.
-
Implementing child benefits that cover all children and support women’s engagement in formal employment. Child benefits are not automatically “empowering” for mothers and women. However, when schemes are designed to minimize exclusion, stigma and non-take-up, and benefit levels are adequate and predictable, this can make a huge difference to women’s lives. Universal child benefits10 are particularly effective, as they cover all children without creating poverty traps or disincentivizing employment, since they are not tied to parental earnings or employment status (ILO, UNICEF, and Learning for Well-Being Institute 2024). This can promote women’s income security and encourage labour market participation. Universal coverage can also be achieved through “mixed system, coordinated” child benefits, combining contributory social insurance and non-contributory means-tested schemes, as occurs in Argentina and Switzerland. If carefully designed, these mixed schemes can incentivize formal employment by offering a contributory child benefit which is set at a higher level than the tax-financed one. This can incentivize both parents to affiliate with social insurance, and thereby defuse disincentives that may occur with some means- or work-tested child benefits, which impede women from fully participating in the formal economy (see McClanahan and Gelders 2019).
-
Investment in accessible, affordable and high-quality social and care services to complement social protection provision. Some countries coordinate social protection with care policies, offering either public childcare services or childcare allowances in addition to child benefits. High-income countries often provide both, distinguishing child benefits (for child-raising costs) from childcare benefits (for care services). This distinction ensures income security for child raising while care services or allowances address care needs. Investing in inclusive childcare can create win-win scenarios both for mothers and for society at large (see box 3.2)
-
Formulating social protection policies that encourage equal sharing of care responsibilities. Ensuring fathers have the possibility to take paternity leave is one element of shared care responsibilities, as are measures to ensure that both women and men have access to adequate parental leave benefits and that their children have access to good-quality early childhood education and care services. Incentives like “daddy quotas”, which reserve a non-transferable portion of the leave for fathers on a use-it-or-lose-it basis, can encourage fathers to take paternity leave (OECD 2016). From virtually no paternity leave 50 years ago, some 62 per cent of countries now provide it, and the length and quality is improving, though more needs to be done (Gromada and Richardson 2021; Addati, Cattaneo, and Pozzan 2022).
-
Adopting family-friendly workplace policies, such as flexible hours, breastfeeding breaks and teleworking, can help parents better balance work and family responsibilities (ILO 2016c). These measures are crucial for expanding women’s employment options and promoting a more equal distribution of childcare. Children’s well-being is linked to that of their caregivers, so ensuring adequate social protection and access to decent work, especially for women, is vital in addressing gender inequalities and preventing women from being trapped in low-paid, informal jobs without social protection, which impacts their income security into old age (Alfers 2016; Moussié 2016).
-
Enforcing compliance with child maintenance support/alimony payments. While not a social protection benefit, child maintenance support in the context of family separation is crucial for helping sole parents – often women who typically have custody of children – avoid poverty. However, UN Women found that in 27 of 33 countries examined, most lone-mother families did not receive this support (Cuesta 2022). Ensuring better compliance by men is critical to ensure that sole caregivers receive child maintenance. Moreover, its receipt should not exclude sole parents from receiving other family benefits essential for child-raising costs. Ideally, the State ought to act as an intermediary and pay the child maintenance directly to mothers and then recoup the payments from fathers (Cuesta 2022). This would ensure predictable support while sparing mothers from direct engagement with ex-partners, particularly in cases of intimate partner violence.
Box 3.2. Policy design choices matter if inclusive childcare is to be ensured
The introduction of universal childcare (with negligible fees) in Quebec over the past 20 years demonstrates how inclusive childcare policy generates numerous positive outcomes. Evaluations show that it performs better than childcare targeted at lower-income families; has boosted mothers’ labour force participation – 3.8 per cent higher than it would have been without the policy – thus improving women’s economic security; and has mitigated the financial risks associated with separation from partners. Moreover, the scheme has had multiplier effects and increased Quebec’s GDP by 1.7 per in 2008 (Fortin 2017; Fortin, Godbout, and St-Cerny 2013), demonstrating the economic payoffs of investing in childcare.
The United Kingdom is expanding public childcare, offering 30 hours of free childcare per week for children aged 9 months to 2 years in working families from 2025 (United Kingdom 2024), doubling spending by 2026–27 (Institute for Fiscal Studies 2023). However, this policy excludes many in the bottom 30 per cent of income distribution, as out-of-work caregivers cannot access free childcare. These families face a “triple bind” of less generous income support, increased targeting, and limited childcare access (Institute for Fiscal Studies 2023). Equitable and just social policies should not worsen the insecurity of the least secure (Rawls 1999). In this case, vulnerable families are adversely affected, highlighting the need for careful investment decisions to protect the most vulnerable also.
Making social protection work for women of working age
The need to make social protection work better for women of working age should be obvious. As highlighted in section 2, most women, with and without children, face discrimination in the labour market in accessing decent work, and encounter barriers to acquiring productive assets. As one of the key “institutional filters” that shape opportunities and constraints for addressing gender inequality (Holmes and Jones 2013), social protection systems play a critical role in addressing, and to some extent also offsetting, inequalities in labour markets and employment, facilitating women’s access to decent work and contributing to more gender-equitable outcomes.
The unequal sharing of care responsibilities and the lack of access to care services make it difficult for women to combine paid work and caring for children and other dependants – challenges which culminate acutely during their prime productive and reproductive years (ILO 2024b). While poverty rates decrease for both women and men upon attaining adulthood, for women aged 20–34 they are 2 percentage points higher than for men (Muñoz Boudet et al. 2021; UN Women and World Bank 2018). It is no coincidence that these differences in poverty rates occur in the prime reproductive (and productive) years, when women are most likely to be caring for young children.
The well-being of women of working age cannot be dissociated from the quality of social protection they enjoy. Ensuring that women can access adequate social protection during working age is indispensable to their well-being and enjoyment of rights. However, there are large gaps in effective coverage for benefits that women of working age should be protected by, such as maternity benefits, work injury benefits, unemployment benefits and, in case of need, social assistance. These shortcomings relate to gender-based inequalities in paid employment and unpaid work, including care work, the design of benefits being insufficiently informed by gender-specific risks and vulnerabilities, and pervasive discrimination (see section 1). To address these inequalities and discrimination, a comprehensive policy approach ensuring that women are better covered by all social protection functions is essential.
4.1 Maternity protection: Access to healthcare and income security
Pregnancy and childbirth are uniquely female experiences, meaning that women require a period of leave to ensure physical recovery from childbirth. In contrast, caring and parenting can and should be shared between parents. Effective maternity protection is one of the key social protection elements for improving the lives of mothers, supporting the health and nutrition of women and newborns alike, and contributing to gender equality. Yet too many women across the world do not enjoy adequate levels of maternity protection. Moreover, pregnancy, childbirth and parenting usually involve both a substantial loss of income and increased costs, which in the absence of effective social protection can put women’s and men’s income security at risk.
Maternity protection includes income security (cash benefits) and effective access to good-quality maternal healthcare without hardship, as well as leave and workplace policies to support pregnant women and mothers of newborns (ILO 2021j; 2024g; Addati 2015). For instance, employment and labour market interventions, such as employment protection and non-discrimination, childcare solutions after return to work, adequate occupational health and safety measures and breastfeeding facilities in the workplace, are important complements to maternity benefits in protecting the well-being of mother and child and supporting women’s continued labour market engagement, as highlighted in the Maternity Protection Convention, 2000 (No. 183).
Access to maternal health services, including pre- and postnatal care as well as skilled assistance at birth, is key for all women. In fact, effective access to skilled assistance at delivery, as well as pre- and postnatal care without hardship, is an essential component of maternity protection and social health protection alike. Particular efforts are needed to ensure effective access for expectant mothers with disabilities, who face additional barriers in meeting their sexual and reproductive healthcare needs, including societal misperceptions and stereotypes around their sexuality, inaccessibility of services and/or information, and fear of abuse. Effective access to needed services for all women is important for achieving progress towards SDG targets 3.1, 3.2, 3.8 and 5.6 on reducing maternal and child mortality, reaching universal health coverage and achieving gender equality. Access to maternity care is part of access to healthcare, as discussed in section 6.
A lack of income security during the final stages of pregnancy and after childbirth forces many women either to keep working into the very late stages of pregnancy or to return to work prematurely, thereby exposing themselves and their children to significant health risks (ILO 2024g, section 4.2.2). This risk is exacerbated when social health protection is not available and the cost of seeking care is paid out of pocket (see section 6). Yet only about 36.4 per cent of women with newborns worldwide receive a maternity cash benefit, which leaves the majority (63.6 per cent) without income security shortly before and after giving birth (figure 4.1). There are also large and troubling regional variations: while coverage is just under 80 per cent in Europe and Central Asia, only 6.7 per cent of mothers of newborns in Africa are covered.
Figure 4.1. Effective coverage for maternity protection: Share of women giving birth receiving maternity cash benefits, by region, subregion and income level, 2015 and 2023 (percentage)
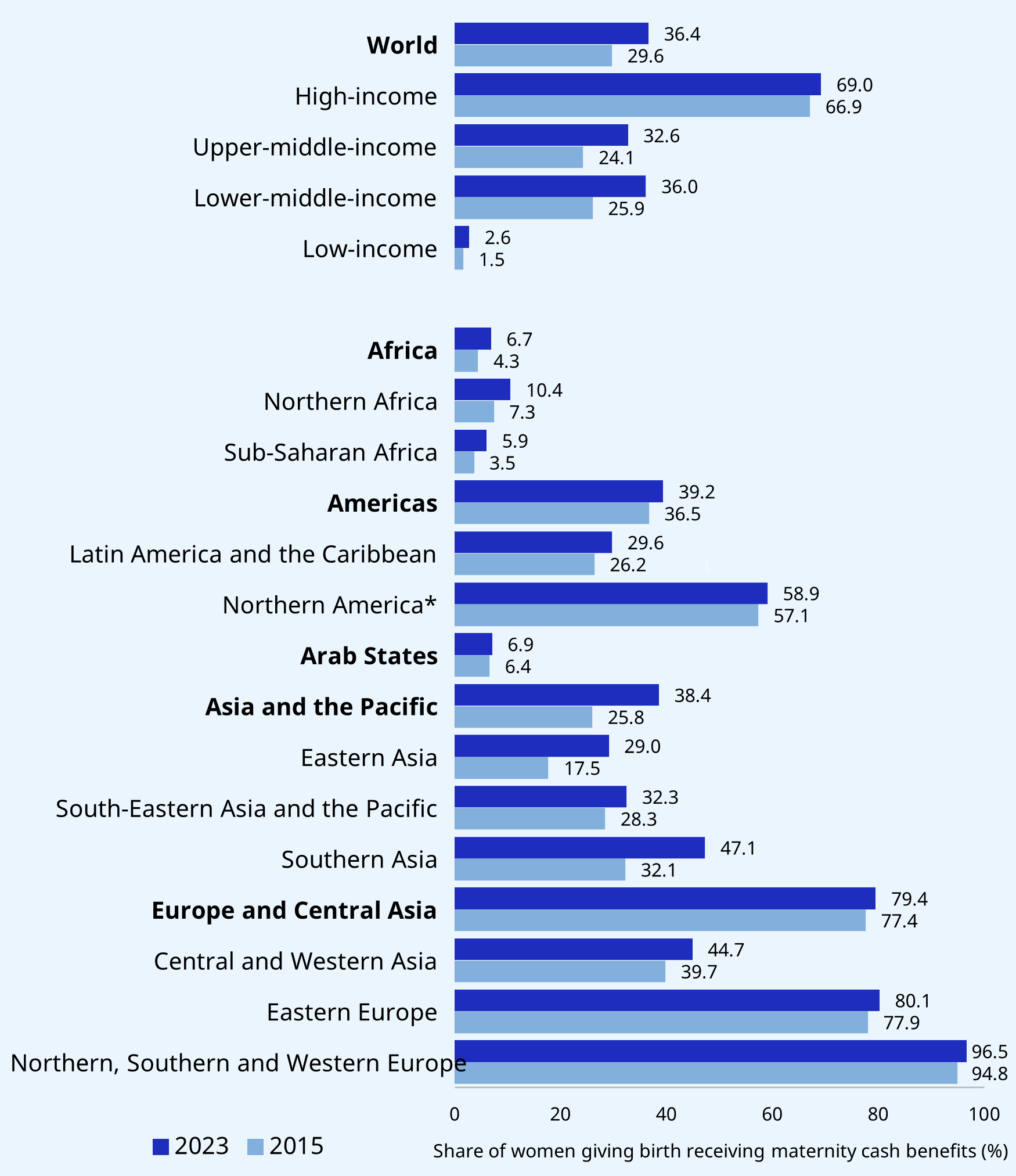
Notes: See Annex 2 of ILO (2024g) for a methodological explanation. Global and regional aggregates are weighted by number of women.
Source: ILO (2024g).
Ensuring maternity benefits are adequate, in terms of both level and duration, is critical for allowing women sufficient time for rest before childbirth and recovery from it, which is critical for their and their children’s health and well-being. The level of the maternity cash benefit, calculated as a proportion of the woman’s previous earnings for a minimum number of weeks of paid maternity leave, as well as the duration of payment, varies widely. Of 210 statutory maternity cash benefit schemes in 173 countries, 190 pay benefits as a share of previous earnings; of these, 124 schemes replace the full earnings, 41 replace at least 66 per cent, as required by Convention No. 183, and 21 replace at least 45 per cent, as required by Convention No. 102 (ILO 2024g). When it comes to the duration of maternity benefits, a total of 121 of the 210 schemes meet the higher standard of Convention No. 183 of 14 weeks or more, and 51 grant the benefit for at least 12 but less than 14 weeks. Thirty-eight schemes provide benefits for less than the 12 weeks recommended by Convention No. 102. Similar gaps in the adequacy of provision for accessing healthcare without hardship during maternity exist and are further illustrated in section 6.
Some countries, such as China, Colombia and Oman, have recently extended their maternity provision, which marks important progress (see box 4.1 on China). Extending maternity protection to workers in the informal economy is particularly important to enhance women’s access to maternal healthcare and income security, which can also contribute to their longer-term transition from the informal to the formal economy (ILO 2016a). For example, Kenya is exploring the extension of maternity benefits to hitherto unprotected women (see box 4.2).
Box 4.1. Incremental extension of maternity protection in China
Since the founding of the People’s Republic of China in 1949, the Government has introduced a series of reforms to improve maternity protection (Liu, Yu, and Wang 2020). Some of the key steps undertaken include:
-
Increasing the duration of maternity leave from an initial 56 days to 90 and ultimately 98 days, in line with ILO standards.
-
Extending maternity protection also into the workplace by ensuring that, during pregnancy, women workers cannot be assigned heavy physical labour, have their working hours extended, or have their labour contracts terminated during pregnancy, childbirth or lactation. Furthermore, time taken to access prenatal care is counted as worktime, women have the right to breastfeeding breaks, and employers need to provide related facilities.
-
Introducing provision for paternity leave and emphasizing the joint responsibility of parents to provide for the child.
The national law is implemented through population and family planning regulations at the provincial level, which vary with regard to the duration of maternity leave. All provincial regulations provide even longer periods of leave than stipulated in the national law: the majority for up to 158 days and the shortest for 128 days. All provinces also provide for paternity leave, the majority offering 15 to 20 days. However, the trend towards extended maternity leave has also received some criticism, since very long spells of maternity leave tend to adversely affect women’s career development. There are also concerns that the extension of maternity leave is sometimes motivated by concerns about China’s low fertility rates rather than being aimed at the protection of women’s (and children’s) health and well-being. While enforcement of the law and a more uniform application across the provinces would be desirable, it is encouraging that China has achieved almost universal coverage with a comprehensive benefits package for pregnant women and nursing mothers.
Box 4.2. Exploring the promise and feasibility of a universal maternity cash benefit in Kenya
In Kenya, women employed in the formal sector have access to maternity healthcare through mandatory social health insurance provided by the National Health Insurance Fund (NHIF). Those outside formal employment arrangements can enrol voluntarily for health coverage. Yet so far only 4.5 per cent of pregnant women in informal employment are enrolled. For others who are uninsured, the Linda Mama (“Caring for the mother”) programme currently offers free maternity health services for one year.
Income security is assured through paid maternity leave provided by individual employers mandated by employer liability, yet these arrangements often create disincentives to hiring women and discrimination in the workplace. Existing maternity leave provision covers only a small proportion of women in the population (6.5 per cent).
Women working outside formal employment arrangements, including those in the informal economy, are particularly vulnerable to income insecurity risks. This often drives them to continue working into late stages of their pregnancy or return to work prematurely after delivery, posing significant health risks to themselves and their children. For this reason, Kenya is considering the introduction of a maternity cash benefit scheme, complementing the free maternity health services for all women. A well-designed cash benefit has the potential to reduce poverty, enhance maternal and infant health and well-being, promote gender equality and advance decent work. The NHIF collaborated with the ILO through a feasibility study to explore policy options for the introduction of a maternity cash benefit for all women in Kenya, including moving towards a social insurance scheme to replace the employer-liability scheme, complemented by a non-contributory cash maternity benefit to reach universal coverage (ILO and NHIF 2023).
Adequate maternity protection is also instrumental in addressing discrimination in employment, contributing to reducing the motherhood penalty (see section 2) as well as promoting women’s (and their children’s) income security and access to healthcare and decent work. As with all social protection functions, achievement of this objective is contingent on the State actively taking it on and finding the fiscal space to ensure all women are covered adequately while attending to other key policy actions; among them:
-
Policymakers should make adequate maternity protection a key component of policies for gender equality, ensuring effective coordination between cash benefits, maternal healthcare and labour protection. States should assume their overall and primary responsibility for ensuring that all women, regardless of their employment status, can access adequate and comprehensive maternity protection. The cost of accessing maternity care, and the importance to the health of both mother and child of physical rest around childbirth and adequate nutrition during pregnancy and when breastfeeding, necessitate a comprehensive approach to maternity protection. Guaranteeing effective access to maternity care and income security for all women can be achieved by a combination of social insurance and tax-financed provision, complemented by appropriate adaptation to workplaces (see below). Cash maternity benefits are cost-effective and “easier” to implement than some other mechanisms like unemployment protection. Hence, for governments, it can be a low-hanging fruit offering a direct way to signal women’s value in society.
-
Transitioning from employer-liability mechanisms to social insurance mechanisms improves women’s income security and reduces the risk of discrimination. Maternity benefits that are financed collectively through employers’ and workers’ social insurance contributions and/or general taxation achieve better outcomes for women than employer-liability mechanisms, in terms of equality of treatment, reducing discrimination in hiring and in employment, averting the risk of non-payment of due compensation by the employer, and facilitating the coverage of women with low contributory capacities and interrupted employment histories (ILO 2021j, 111). For example, in Jordan, the transition to a social insurance maternity benefit from an employer-liability mechanism contributed positively to the retention of women in the workplace and to their income security (ILO 2021b).
-
Pregnancy and childbirth should be systematically covered through adequate social health protection and cash transfer programmes. In addition to effective access to maternal healthcare (see section 6), the specific needs around pregnancy and childbirth need to be taken into account in cash transfer programmes. In conditional cash transfer programmes, particular attention needs to be given to avoiding negative effects on women’s time-use and autonomy (see also subsection 4.5).
-
Maternity protection should be anchored in a comprehensive family policy portfolio that also includes paternity benefits and parental leave benefits to better balance care and work responsibilities between parents. As discussed in section 3, this means implementing social protection policy for children and adopting work-related measures that facilitate a fairer sharing of work and family responsibilities and opportunities for both women and men. Sustained investment in affordable and good-quality childcare services that are adapted to the needs of working parents can be a game-changer: it can support the childcare responsibilities assumed by families – disproportionately by women – and facilitate women’s employment, while also creating decent jobs in the care sector (ILO 2018a). Paternity benefits contribute to transforming gender-stereotypical concepts around parenting.
-
States should actively pursue employment policies that eliminate the motherhood penalty and workplace discrimination against women. This means ensuring that workplaces cater for the needs of pregnant women and mothers with newborns who return to work, including breastfeeding arrangements, occupational safety and health measures, employment protection and non-discrimination. In addition, promoting the more equal sharing of care responsibilities between women and men is essential, including through social protection benefits. Apart from providing affordable childcare solutions, as noted above, this can take in paternity and parental leave policies, sickness benefits for children, and related leave arrangements for both mothers and fathers, as well as the possibility of flexible working-time arrangements, including adequately remunerated and protected temporary part-time employment arrangements. It also presupposes combating masculine corporate cultures and related gender-biased hiring and promotion decisions at the enterprise level. Policy action in these areas can promote gender equality at home and at work.
4.2 Unemployment protection: Income security, skills development and job matching
Unemployment protection schemes (including unemployment insurance, unemployment assistance and related schemes) play a critical role in protecting jobs, incomes and living standards, through unemployment benefits and job retention schemes, especially where they are well connected with active labour market policies (ILO 2024g, section 4.2.6; 2021j, section 4.2.6; 2020g). Adequate unemployment protection can make a marked difference to women’s economic security and autonomy, increasing their bargaining power and career choices, as well as their opportunities for developing their capabilities. With this protection, women are not compelled to take the next best job (often informal employment) but can search for one that better matches their skills and experience and offers adequate pay, protection and benefits. Together with employment services, well-designed unemployment protection schemes also provide access to skills development opportunities, which allow women to upgrade or change their career paths and ultimately have more control over their lives (ILO 2023a; Avila 2021). They can also support women’s reintegration in the labour market after periods of economic “inactivity” for reasons of family care (Peyron Bista and Carter 2017). In short, unemployment protection can bolster women’s employment prospects and the quality of their employment. In this way, social protection can be gender-responsive and even trigger a transformative agenda for women.
However, unemployment protection remains the least developed branch of social protection. A mere 16.7 per cent of unemployed workers worldwide actually receive unemployment benefits. This equates to 157 million unemployed persons who do not have access to unemployment cash benefits (ILO 2024g). While sex-disaggregated data on effective coverage is not available, figure 4.2 shows that in some regions, women in the labour force are slightly more likely than men to be legally covered by an unemployment protection scheme, which may be due to a higher likelihood of being an employee or working in sectors and occupations that are legally covered for unemployment, for example the public sector, even though civil servants are often excluded.
Figure 4.2. Legal coverage for unemployment protection: Share of persons in labour force aged 15+ covered by unemployment cash benefits, by region, subregion, income level, sex and type of scheme, 2023 or latest available year (percentage)
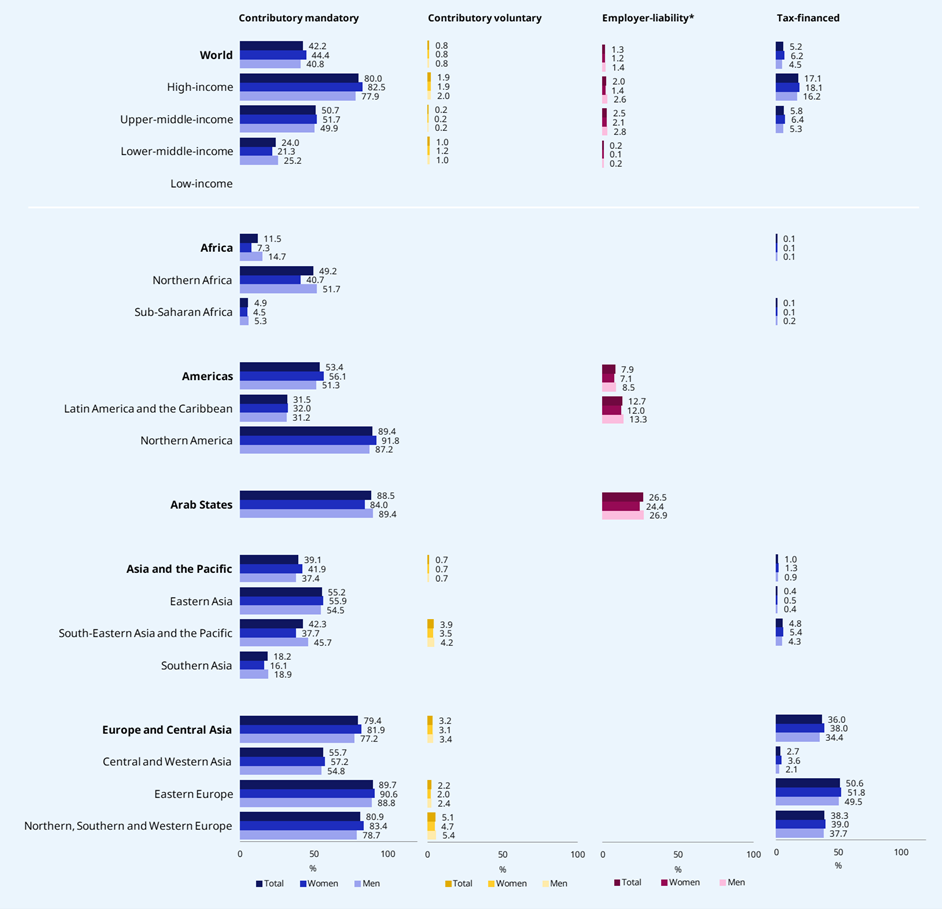
Notes: See Annex 2 of ILO (2024g) for a methodological explanation. Global and regional aggregates are weighted by labour force aged 15+.
Source: ILO (2024g).
Nevertheless, the implementation gap between legal and effective coverage is likely to be large. Women often face greater difficulties in accessing unemployment benefits due to more interrupted employment histories and higher levels of part-time and temporary work, which makes it more difficult to meet the eligibility criteria for unemployment insurance schemes. Removing barriers to access, such as revisiting eligibility conditions with regard to the minimum duration of previous employment and extending coverage to categories of workers not yet covered (for example domestic workers: see ILO (2022e)), enhances protection not only for women but also for many men.
In contexts where unemployment protection schemes are not yet available, employment guarantee schemes,11 such as India’s Mahatma Gandhi National Rural Employment Guarantee Schemes (see box 4.3), can play a somewhat similar role by guaranteeing a wage for work performed or, if no work can be obtained, a cash benefit (which is not the case in most other public employment programmes discussed in subsection 4.6).
Box 4.3. India’s Mahatma Gandhi National Rural Employment Guarantee Schemes (MGNREGS)
India’s Mahatma Gandhi National Rural Employment Guarantee Act provides 100 days of guaranteed work per household per year at the minimum wage to any applicant, or cash benefit for the same period if no work is available. The Act mandates that at least one third of employment should go to women, which is usually exceeded. In August 2022, the monthly female participation rate was 56.6 per cent (Government of India 2023).
Some design features can be considered gender-responsive. For example, wages are set in accordance with the state minimum wage and are often higher than those that women usually receive as unskilled agricultural workers, thereby lifting the wages of women agricultural workers in communities where the schemes are operating, and narrowing gender wage gaps (UN Women 2015b; Ehmke 2015; Gentilini et al. 2020). There is also evidence that MGNREGS increased women’s engagement in financial services and their decision-making power in the household, decreased the incidence of violence and harassment against them (Rodriguez 2022) and improved their mental health (Gentilini et al. 2020). Importantly, the MGNREGS have also paid attention to making the schemes accessible for workers with disabilities, by making efforts to have a stigma-free work environment and offering work opportunities close to their place of residence.
While these impacts are promising, there is still scope for improvement, such as ensuring the mandatory provision of childcare at all worksites, strengthening monitoring and enforcement, and strengthening skills development and social protection coverage for greater gender equality.
Public employment services (PES) can also be vital for promoting women’s employment, preserving their skills, sustaining their connection to the labour market and supporting their return to work. For example, the Republic of Korea’s PES collaborates with third-sector organizations like the Occupational Centre for Women in Ansan City to provide targeted services, including job search support and training, to women facing various challenges such as career interruptions, language barriers or lack of formal qualifications (ILO 2020a).
Several policy recommendations can be advanced to increase women’s access to unemployment protection in a way that enhances the gender-responsiveness of such provision. These include:
-
Facilitating women’s access to adequate unemployment benefits by identifying and removing barriers to their inclusion. This can include allowing for shorter or interrupted contributory periods to be eligible for benefits, extending coverage to workers in temporary or part-time employment, ensuring that contribution rates are commensurate with contributory capacities with contribution subsidies where necessary, making schemes disability-inclusive, and simplifying administrative procedures (ILO 2021h).
-
Closing coverage gaps in unemployment protection for women by also requiring that States actively encourage the formalization of employment through an integrated approach to social protection and employment policy. While the extension of unemployment benefits to those not yet protected can promote formal employment and reduce pressures towards the informalization of jobs, it needs to be accompanied by broader policies to foster the transition of enterprises and workers towards the formal economy (ILO 2021b). Such policies are essential for protecting those who are at risk of being unemployed, and cultivating a virtuous cycle of decent employment.
-
Closing gaps in coverage through non-contributory benefits. While formalization strategies can help expand the coverage of unemployment insurance, this might need to be complemented with non-contributory schemes financed from general taxation, such as unemployment assistance or social assistance to guarantee at least a basic level of income security in the event of unemployment (ILO 2016b; 2021j; 2024g).
-
Linking unemployment protection with employment promotion services and activation measures to enhance women’s economic security, appropriately tailored to the reality of their lives. The close interrelationship between unemployment benefits and employment promotion measures, including active labour market policies (ALMPs), contributes to the better matching of skills and jobs and encourages increased employability. This provides an enabling environment for the promotion of productive and decent employment (McCord et al. 2024). Of particular significance is the coordination of unemployment protection schemes with ALMPs to guarantee income security while at the same time facilitating job search and retraining.
4.3 Disability benefits and other support in case of disability
Throughout this document, we have discussed the extent to which women and girls with disabilities often face greater disadvantages, discrimination and exclusion than those without disabilities, as well as men and boys with or without disabilities. These findings illustrate the importance of not looking at different forms of vulnerability and discrimination in isolation, but focusing on their multiplicity and the intersections between them. In this vein, Article 28 of the Convention on the Rights of Persons with Disabilities calls on States Parties “to ensure access by persons with disabilities, in particular women and girls with disabilities and older persons with disabilities, to social protection programmes and poverty reduction programmes” (emphasis added).
As with other contingencies, women with disabilities are worse off as a result of the discrimination they face in accessing education and the labour market, as well as in accessing social protection across the delivery chain, from having information about the schemes and programmes to being able to access benefits and services, and to lodge complaints and make appeals where needed. Cumbersome and discriminatory requirements for disability determination and assessments create additional barriers to access social protection entitlements for women with disabilities. In countries where women are overrepresented in informal employment and self-employed, temporary or part-time work, they are less likely to have access to social insurance and thus to acquire disability entitlements but also other forms of protection important for women with disabilities, such as health insurance, old-age pensions, and sickness and unemployment benefits. Social insurance is important in case of acquiring disabilities during working age. In addition, non-contributory schemes need to cover those who have not earned entitlements under a social insurance scheme, those born with disabilities or those with disabilities whose disability-related extra costs exceed the earnings-related benefits paid under the insurance. However, in many countries, the coverage of both social insurance and tax-financed disability benefits is insufficient: worldwide, only an estimated 38.9 per cent of people with severe disabilities receive a disability benefit, with large regional variations (ILO 2024g). Coverage ranges from near universal in Eastern Europe to just above 8 per cent in Africa.12
However, the design of existing schemes does not always comply with international standards as regards the level of benefits, the eligibility criteria or the duration of payment. For example, Convention No. 102 (Article 57) and the Invalidity, Old-Age and Survivors’ Benefits Convention, 1967 (No. 128) (Article 11) require a replacement rate of 40 per cent after 15 years or more for receiving a full benefit. Of 66 schemes for which data is available, 31 exceed the 40 per cent benchmark after 15 years of contributions, while the remaining 35 schemes provide less than 40 per cent of the replacement rate even with 15 years of contributions (ILO 2024g).
Women with disabilities are also underrepresented in decision making, in terms of holding public office in general as well as in national coordination mechanisms on disability matters (UN 2019). As with other contingencies, measures that improve the coverage of people with disabilities overall will also benefit women with disabilities, while improving their representation in related forums will also enable them to address gender-specific needs. Measures to improve the inclusiveness of social protection systems include, among others, the following:
-
Social protection systems should fulfil the following functions for people with disabilities, along the life cycle and for all types of disabilities: (1) Ensuring their income security; (2) covering disability-related extra costs; (3) facilitating access to needed services, in particular healthcare but also early childhood development, employment services or support services, including assistive devices and rehabilitation services.
-
To fulfil these functions, a twin-track approach is needed. On one hand, the accessibility of social protection schemes and programmes that are not disability-specific should be ensured so that people with disabilities can benefit from them. On the other, disability-specific schemes are also important, to cater to the specific needs of people with disabilities and support them in achieving maximum participation and autonomy. Accessibility and non-discrimination need to be ensured across the delivery chain, from information about schemes and programmes to registration processes, including disability identification and assessment, and delivery of benefits and services, as well as complaints and appeals mechanisms.
-
Eligibility criteria should be designed to promote inclusion and participation. For example, benefits for people with disabilities should not be conditioned on proof of the person’s incapacity to work. People with disabilities should not be forced to choose between receiving support and entering the labour market. Rather, benefits should be compatible with work to cover the costs of entering employment.
-
Disability determination and assessments should be easily accessible, affordable, accurate, reliable and independent. They should focus on assessing the support needs of the person with disabilities in the person’s environment, and ensure referral as needed.
4.4 Employment injury protection and the right to a safe and healthy working environment
Employment injury protection provides an important – yet often overlooked – element of social protection for women. Prior to the COVID-19 pandemic, 1.9 million people died annually of work-related injuries and diseases, and it is estimated that the societal costs of these amount to 3.9 per cent of global GDP (ILO 2023e). In addition to the prevention of these contingencies, effective responses to the income insecurity and care needs they produce are essential.
Employment injury and occupational disease benefits should consist of medical and allied care for injured workers; and earnings-related periodic cash benefits for disabled workers, or survivors of deceased workers, including funeral grants. However, according to an ILO desk review, only a minority of schemes actually include healthcare benefits, and lump sum benefits seem to be the preferred form of benefit that is disbursed in practice (ILO 2021j; 2024g). Some countries also provide rehabilitation and reskilling to affected workers, while ensuring their income and economic security.
While recognized in 2022 as one of the Fundamental Principles and Rights at Work, the right to a safe and healthy environment is not yet a universal reality. National occupational safety and health (OSH) systems, which include social protection against the risks of employment injury and occupational diseases, remain underdeveloped and under-resourced in many settings. Other challenges exist in the provision of OSH which have adverse implications for women. For instance, in many countries and sectors, the full range of safety and health hazards that exist in the world of work is not comprehensively identified, acknowledged and addressed. At the workplace level, OSH management systems are not always in place and workplace safety and health suffers from low enforcement and compliance, thereby undermining its preventive function (ILO 2023e).
Similarly, effective coverage of workers by employment injury insurance (EII) is still low worldwide, at 37.4 per cent of the labour force. As a result, some 2.1 billion employed persons are not covered should a work-related injury or disease befall them (ILO 2024g). Coverage is significantly lower in most low- and middle-income countries, owing to the prevalence of employer-liability mechanisms with often weak enforcement. While there is near parity for women and men in terms of legal coverage at the global level, there are significant gender gaps in some parts of the world, especially in Africa (figure 4.3).
Too many countries (16, most of them in Africa or in Asia and the Pacific) still depend on an employer-liability model, where the individual employer assumes the total costs of any compensation for the worker without making use of the risk-pooling mechanisms available in social insurance (ILO 2024g, section 4.2.4). Employer-liability models suffer from poor compliance, due to insolvency, bankruptcy or financial constraints, or reluctance to assume responsibility for injuries so as to absolve themselves of liability for compensation. This results in weak effective protection in the event of an injury or disease. Moreover, employer liability is not a solution for the self-employed population, where in many countries women are disproportionately represented. In addition, compensation for permanent disability and survivors’ benefits are often provided in the form of lump sum payments, which do not provide stable income replacement to beneficiaries through periodic benefits. However, a growing number of countries are adopting and implementing EII schemes aligned with the social security principles of both Convention No. 102 and the Employment Injury Benefits Convention, 1964 (No. 121), thereby improving effective coverage, in particular in hazardous occupations and in small and medium-sized enterprises, and enhancing protection levels.
The gender-responsiveness of EII cash benefits is somewhat limited by the fact that they are earnings-related and do not provide minimum payments, which constrains their redistributive effect. They nevertheless are an important part of social protection for women workers and their dependants. In the absence of effective and adequate employment injury protection and related rehabilitation or care services, it is likely that in most societies it will fall to women to take care of the injured worker, in particular in the event of chronic disease or permanent disability.
Figure 4.3. Legal coverage for employment injury protection: Share of persons in labour force aged 15+ covered by cash benefits in case of employment injury, by region, subregion, income level, sex and type of scheme, 2023 or latest available year (percentage)
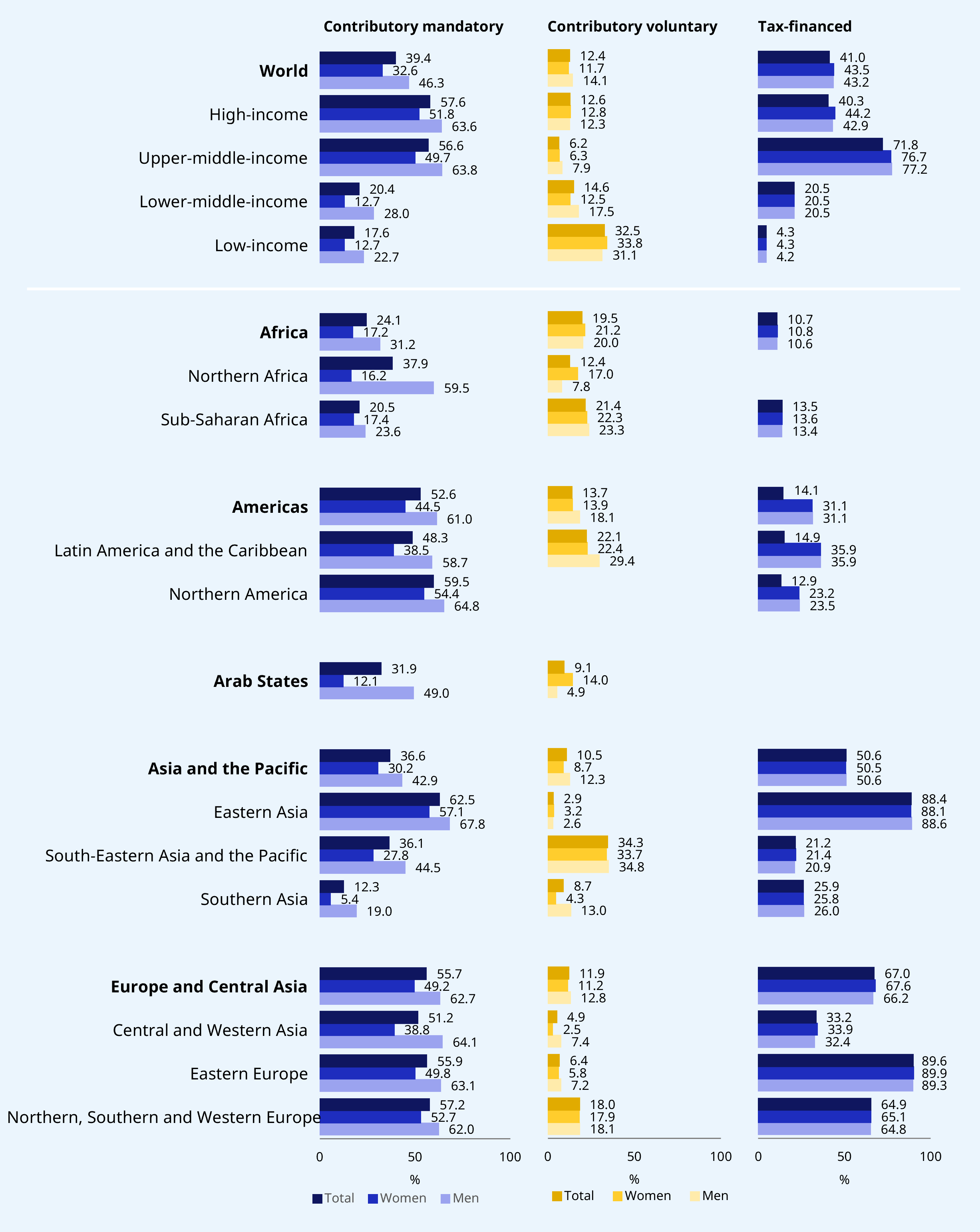
Notes: See Annex 2 of ILO (2024g) for a methodological explanation. Global and regional aggregates are weighted by labour force aged 15+.
Source: ILO (2024g).
To prevent work-related injuries and diseases, policymakers also need to ensure a comprehensive understanding and application of occupational safety and health – one that encompasses not only physical and biological hazards but also psychosocial risks that occur when job demands outweigh the resources available to workers. This also includes psychological forms of violence, such as harassment – including sexual harassment – bullying and mobbing, to which women workers are subject to a greater extent than men,13 and which can be deleterious to women’s mental and physical health and their economic security. For example, care workers – predominantly women – are likely to experience stress and burnout, which may lead to high staff turnover, potentially reducing the availability of greatly needed care services (Dorn et al. 2023; ILO 2023). The recognition of mental stress as an OSH risk raises a broader issue about defining employment injury and disease in a way that is relevant to the service-dominated labour markets of the twenty-first century.
A recognition of the gender dimension of hazards became especially evident during the COVID-19 pandemic. As women constitute 70 per cent of the health workforce, including the large majority of front-line workers, many of them at first had to work without adequate personal protective equipment (PPE), heightening their risk of exposure to the virus before corrective OSH measures were deployed (ILO 2019a; 2020b; 2023e). However, other care workers, including those in old-age residential homes and domestic workers, were often not protected to the same extent, leading to higher COVID-19 contraction risks (in terms of incidence) compared to nurses and other workers in health facilities and certainly the general community (Nguyen et al. 2020).
Even the best prevention efforts do not always ensure that hazards are prevented, and that injuries and diseases do not occur/are not contracted. In this respect, another innovation during the pandemic was that COVID-19 was recognized as an occupational injury or disease in many countries, which is particularly relevant for healthcare staff. This is important, as it can be difficult to determine whether the infection is work-related or not, despite the guidance provided by international labour standards to this effect. In the specific circumstances of COVID-19, at least 50 countries provided compensation to workers infected by the virus, either as work-related injuries (such as Italy and Spain), as occupational disease (such as Belgium, the Republic of Korea, South Africa and the United Kingdom) or with provision for both (such as Germany) (see Nys et al. 2023; ISSA 2020). These cases have been covered in different ways, depending on how work injury is addressed in different countries: through either cash benefits from EII or sickness benefit schemes, wage replacement, and/or the provision of medical care including rehabilitation, and in the event of fatality through survivor pensions and death benefits. Moreover, in many countries, essential workers who ran a high risk of exposure to COVID-19 were, depending on interpretation, compensated or incentivized (i.e. provided with a bonus) to carry on their work, despite its risks, through “hazard pay” (ILO 2021j).
For women, this represented an example of policy progress, enhancing protection against occupational hazards in certain sectors or occupations where they make up a majority of the workforce. It is also important to note that the recognition of COVID-19 as an official occupational disease in many countries constitutes one of the few emergency social protection measures adopted during the pandemic which became a permanent provision. It therefore represents a small gain in gender-responsive policy (ILO 2021j).
Much more can be done to improve the protection of women in contentious and risky forms of work, such as sex work, from occupational hazards (through comprehensive prevention policies, which may also include PPE and other prophylactics), and recognize injuries and diseases (including sexually transmitted diseases) in EII schemes, to provide income security and access to medical care and rehabilitation without hardship.
Aside from the pressing need to close protection gaps, policymakers should give more attention to gender-specific vulnerabilities and the specific risks women face in certain sectors and occupations. This requires that EII schemes be better adapted to the needs and circumstances of women. Steps in a gender-responsive direction could be the following:
-
Dispensing with employer-liability systems and protecting workers through social insurance systems in case of work-related injury and disease would be a move towards fair, timely and effective compensation. Social insurance-based employment injury schemes provide timely, adequate and comprehensive benefit entitlements anchored in national legislation, financed collectively through a large risk pool, and not left to the discretion of individual employers. Adaptations of such schemes that attempt to provide minimum guaranteed levels of benefits may increase gender-responsiveness by ensuring that workers with lower earnings do not receive meagre income replacement levels. Moreover, efforts to extend coverage to self-employed workers can further enhance protection for many vulnerable workers.
-
Both OSH policy and EII must cohere better and aim to prevent and cover a wider range of occupational hazards that are likely disproportionately to affect women workers and certain sectors and occupations. This means policymakers thinking beyond the more traditional risk paradigm of physical and biological hazards covered (e.g. mine collapse or pneumoconiosis in mining industries), and responding to the risks that women workers are more likely to face, such as violence and harassment, mental health issues (rife among health, education and care sector staff) and other injuries and diseases, as well as general wear and tear (e.g. eye injuries from repetitive movements on electronic assembly lines in the garment industry).
-
What is covered under EII and OSH requires frequent revisiting, given the emergence of new hazards and diseases in a constantly changing world of work. For instance, there is a need for better recognition of occupational diseases, including mental health conditions. Greater recognition of neurological diversity at work can protect against ill health for both women and men. Women are more likely to experience depression or suffer from acute anxiety than men, for example, and this can be exacerbated by work factors (harassment, pay inequity and balancing care). This means employers may need to ensure that work is organized in a way that is safer and fairer and does not aggravate such predispositions to mental illness. Moreover, given that the nature of work-related hazards has changed in the context of transformations in the economy, greater attention to work that is performed in public spaces, online or at home is necessary.
-
Policymakers and employers should do much more to reduce the hazards women face at work, including eliminating bullying and harassment and, at its worst, physical, psychological or sexual violence. While men can face such hazards at work too, women tend to encounter some of these risks more frequently, especially sexual harassment. Zero tolerance for such behaviour would contribute to reducing work-related injury and disease for women. Guidance on how to do this can be gleaned from the general principles in the prevention and management of violence and harassment at work in the Violence and Harassment Convention, 2019 (No. 190), and its accompanying Recommendation (No. 206). Beyond the intrinsic and ethical reasons for eliminating such nefarious behaviour, there is also a business case. The elimination of violence, harassment and discrimination at work may also enhance productivity by alleviating the negative impact on workers’ mental health (ILO 2023e). Social security administrations ought to consider extending EII protection to compensate workers for workdays they may lose as a result of workplace violence and harassment, and the need for mental and physical recuperation.
-
Achieving the recommendations above might mean government agencies and social security institutions pursuing gender mainstreaming activities and training for staff to generate better outcomes for women. For example, Austria has followed a gendered strategy in OSH and the training of labour inspectors, and provides guidance related to gender aspects of OSH and gender-sensitive workplace inspection. Moreover, guidance for specific activities and emerging sectors in which women are clustered, such as home care, also now exists (see ISSA 2017).
-
For people with disabilities in employment, reasonable accommodation of the workplace is a key measure that can contribute to preventing work injuries and creating a safe work environment. People with disabilities often consider their workplace to be hindering them or not easily accessible. In other cases, the assistive devices they need for the work they perform are not available. Given that women with disabilities are less likely than men, or women without disabilities, to participate in the labour market, specific measures need to be designed to make work more accessible and the workplace safer for them.
4.5 Ensuring sickness benefits are gender-responsive
Sickness benefits aim at ensuring income security during sickness or quarantine, or the sickness of a dependent relative ILO (ILO 2024g). They allow individuals to stay home until full recovery, thereby protecting their own health and, in cases of communicable disease, the health of others (ILO 2020e). Sickness benefits contribute to the human rights to health and to social security (ILO 2017), more important than ever when facing adverse health events, for individuals and society alike.
The COVID-19 pandemic put sickness benefit coverage gaps in the spotlight, illustrating how such gaps compelled people to work when sick or quarantined and so increasing the risk of contagion (ILO 2020e). The consequent impact on disease prevention has long been documented, both during previous public health crises such as SARS or MERS (Drago 2010) and in the literature on occupational safety and health in the workplace (James 2019). This now became particularly visible, as it is women that make up the majority of health sector workers (ILO 2020b).
The ILO estimates that 56.1 per cent of the global labour force is legally entitled to sickness benefits, whether provided by social insurance or social assistance, or in combination with employer liability (see figure 4.4). This leaves more than four in ten workers without any legal protection or entitlement to sickness cash benefits. There are wide regional differences, with high levels of legal coverage in Europe and Central Asia and in the Arab States, and lower levels in Africa and in Asia and the Pacific.
These figures further hide the large share of voluntary and employer-liability mechanisms, which often do not translate into effective protection (ILO 2020d). Employer-liability provision supposes that an employer can finance such leave, while it provides no solution for the self-employed workforce. Even where women are entitled to sick pay with employer liability, solidarity in financing is limited, as individual employers are left to bear the costs of workers’ sickness on their own. This may lead to both pressure on workers not to take sick leave and discrimination in recruitment against individuals with declared medical conditions or with higher “risks”, including women. Small enterprises in particular may struggle with the financial implications, and therefore have an incentive to employ workers in forms of employment that are not subject to statutory sick leave (ILO 2020d).
As can be seen in figure 4.4, women in the labour force globally enjoy slightly higher levels of legal coverage, with 53.4 per cent, than men. This is largely driven by the fact that women tend to be less represented among the self-employed population in high-income countries of northern America and Europe, therefore enjoying better legal protection. In low- and lower-middle-income countries the picture is different, in terms of both women’s status in employment and the predominance of employer-liability mechanisms in many regions where the formal economy that enforces labour laws is rather small.
Figure 4.4. Legal coverage for sickness protection: Share of labour force aged 15+ covered by sickness cash benefits, by region, subregion, income level, sex and type of scheme, 2023 or latest available year (percentage)
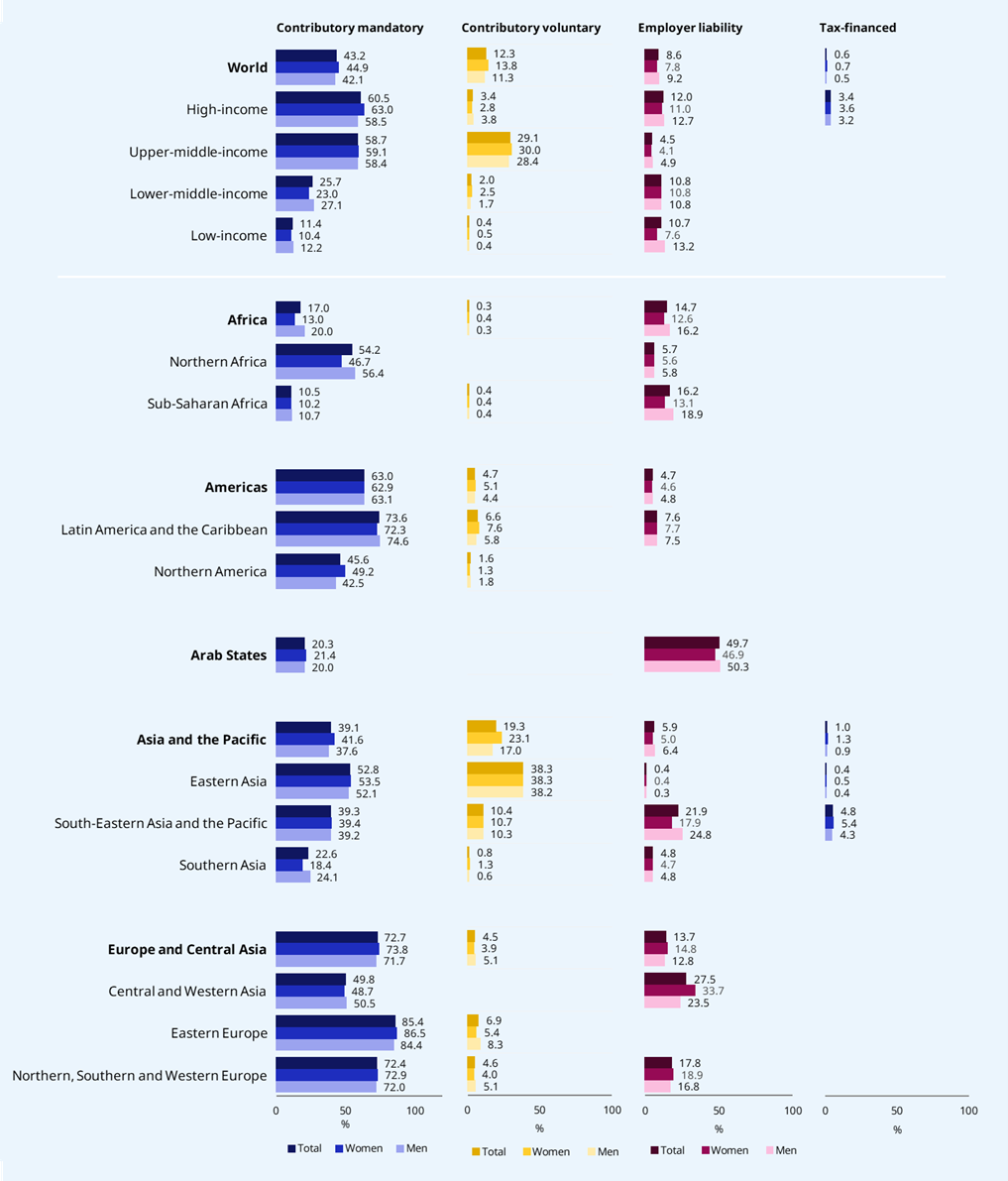
Note: See Annex 2 of ILO (2024g) for a methodological explanation. Global and regional aggregates are weighted by labour force aged 15+.
Source: ILO (2024g)
Link: https://wspr.social-protection.org.
Effective coverage data on sickness benefits is not available at present. While income security in the event of ill health should be monitored under SDG target 1.3, a lack of comprehensive and systematic data collection on the different aspects of effective coverage has led to this dimension currently being excluded from SDG monitoring efforts (Lönnroth et al. 2020).
The adequacy of sickness benefits also has implications for women who can access them. When benefit levels are calculated as a percentage of past earnings, this can result in gender inequality owing to women’s lower benefit levels due to the pervasive gender pay gap. The existence of a guaranteed minimum level is essential for low-income workers and could help redress this risk for working women (ILO 2021c, 253). Of 172 countries for which information is available, 31 have provision for income replacement lower than 60 per cent of past earnings, while an additional six countries offer flat-rate benefits. Without such a guaranteed minimum in place, women are likely to enjoy less adequate benefits as they have lower earnings on average (ILO 2024g).
More can be done not only to extend coverage but also to better adapt sickness benefits to the needs of women. For example, Indonesia, Japan, the Republic of Korea, Spain, Taiwan (Province of China), Viet Nam and Zambia are among the few countries that provide menstrual leave
Sickness benefits can also support care responsibilities, which tend to fall disproportionately on women. Extending this provision so that working people can look after their sick relatives or immediate kin for a short duration is important. For example, Slovakia’s inclusive sickness benefit covers individuals if caring all day for immediate (e.g. parent, grandparent) and non-immediate relatives (e.g. a sick spouse’s parent) (European Commission 2023). However, more typically, sickness benefits are paid for one or both parents caring for a sick child (e.g. ten days in Estonia and between ten and 25 days in Germany). For instance, Finland pays a sick-child benefit to both parents for up to 120 days if their presence is required in the hospital and/or home to adequately care for a sick child. While this provision should be afforded to both men and women to promote fairer sharing of such responsibilities, it can do much to make life easier and more sustainable for women in more challenging circumstances. For instance, sickness benefits to care for a sick child can be a godsend to single mothers who may not be able to rely on a partner or immediate family for the purpose. Expanded sickness benefits to cover certain dependants are a critical step towards enhancing the gender-responsiveness of any such scheme. Without this, women with care responsibilities may have their jobs put in jeopardy by repeated absences.
There are a number of reforms and key actions policymakers could take to enhance the gender-responsiveness of sickness cash benefits. Below are some examples of the types of recommendations that could help accomplish this.
-
Moving away from employer-liability approaches and developing proper social protection schemes financed collectively. There is a need for policymakers to move towards collectively financed sickness benefits, which provide greater potential for addressing inequalities through redistribution with positive results, especially for women. Over-reliance on employer liability worldwide is an important driver of gaps in legal and effective coverage, as evidenced during the COVID-19 pandemic. Extended periods of sickness can constitute an important risk for self-employed workers, which can threaten not only their health and income security but also their ability to maintain their economic activity (ILO 2021h; 2021g). Extending sickness benefits to self-employed workers can make a difference, especially for women.
-
Providing a guaranteed minimum level for sickness benefits. Given that sickness benefits are usually tied to earnings, ensuring a guaranteed minimum would do much to protect the income security of low-income earners, among whom women are disproportionately represented.
-
Ensuring that sickness benefits are responsive to the needs of women. Covering temporarily debilitating menstruation, menopausal episodes or more chronic conditions such as endometriosis would mark gender-responsive progress. Regulating for such conditions to be covered not only protects women’s income security but can also help normalize experience of these sicknesses in the workplace and society in general.
-
Designing sickness benefits to be more inclusive of all types of work and especially those done predominantly by women. Given women’s over-representation in part-time and temporary work, the minimum qualifying period for accessing sickness benefits should be reduced while ensuring that benefits are proportional to time employed so as to cover part-time workers.
-
To realize their gender-transformative potential, making sickness benefits help economically active persons who have to care for a sick dependant. This would help reduce the risk of women losing their jobs because of care responsibilities and diminish the care burden caused by caring for sick dependants as well as reducing the risk of forgone income, as well as allowing the employment relationship to be maintained while they are tending to their loved ones. As with other provision, policymakers must take care to ensure that caring for sick family members does not adversely affect women with respect to the unpaid care burden, and that this provision is available for men and women to facilitate equal care responsibilities. This promotes the income security of all carers and recognizes that both women and men have an employment relationship they need to manage while they fulfil those responsibilities.
4.6 Towards more gender-responsive social assistance schemes
Social assistance schemes usually provide cash income support to vulnerable populations, particularly those in poverty. They play a key role in reducing poverty, vulnerability and social exclusion, when other forms of support are unavailable. Women make up a large portion of beneficiaries of these schemes, which are the subject of significant policy action and experimentation, involving a wide range of social protection actors. Thus, the design, implementation and impact of the schemes can be significant for women. This subsection focuses on a more broad-brush analysis of social assistance programmes and schemes that deal with poverty more broadly.
Our latest data indicates that, globally, social assistance coverage has increased from 26.7 per cent of vulnerable persons in 2015 to 37.3 per cent in 2023. Disaggregating by sex, some 36 per cent of vulnerable women (not otherwise protected by contributory schemes) receive social assistance benefits, compared with 38 per cent of vulnerable men (ILO 2024g). Many women depend on social assistance despite large coverage gaps, but this reliance highlights two issues: their limited access to the more adequate forms of protection provided by contributory schemes, and the lack of gender-responsive design in social assistance. Improving these schemes with women’s active involvement is urgent for achieving gender equality, especially since their income security is less stable than men’s and they therefore have to rely more on social assistance as a means of survival of last resort.
Figure 4.5. SDG indicator 1.3.1 on effective coverage for protection of vulnerable persons: Share of vulnerable persons receiving cash benefits (social assistance), by region, subregion and income level, 2015 and 2023 (percentage)

Notes: See Annex 2 of ILO (2024g) for a methodological explanation. Global and regional aggregates are weighted by population. Estimates are not strictly comparable to the previous World Social Protection Report due to methodological enhancements, extended data availability and country revisions.
Source: ILO (2024g).
Ideally, the goal of social policy is to minimize the need for social assistance, by ensuring access to decent work and higher levels of income security. However, some level of social assistance is always likely to be necessary. For this reason, ensuring that social assistance schemes function well for women living in vulnerable circumstances is a key policy priority. Moreover, if designed badly, social assistance can reproduce gender inequality, worsening women’s quality of life and pushing them into or sinking them deeper into destitution (Watts and Fitzpatrick 2018). For instance, badly designed social assistance can increase conditions of poverty and inequality by creating poverty and precarity traps (Standing 2011; 2009). If insufficient, low benefit levels essentially convey the message that people are not valued, which can be insulting and increase feelings of shame and stigma for both men and women. This can in turn carry a high “compliance” cost and lower take-up, as was the case with the Dibao (Minimum Living Standard Guarantee) social assistance scheme in China (Yang et al. 2019).
The design of social assistance schemes can have a major impact on women’s autonomy and life opportunities – ultimately it can be freedom-constraining or enabling. For instance, there is a wealth of literature showing how social assistance can carry high opportunity, transaction, time and shame costs for women (e.g. Molyneux 2006; Fultz and Francis 2013; Walker 2014). These costs are exacerbated if eligibility criteria are complex and onerous, and entitlements are conditional (i.e. on jobseeking or other behaviours). Complex schemes can result in exclusion and non-take-up, which represent a serious violation of women’s social protection rights. For instance, in certain contexts, literacy rates tend to be lower among women, which can account for a lack of awareness of the existence of entitlements, and the absence of the rudimentary skills required for knowing how to apply for benefits. These are chief among the reasons explaining women’s low take-up of benefits to which they are entitled (UN 2022).
This subsection therefore now examines how well different social assistance instruments support gender-responsive goals, which it does first by addressing provision typically operating in higher-income contexts, and then in lower-income contexts.
Minimum income schemes
A minimum income scheme (MIS), common in Europe, provides means-tested benefits to ensure a basic living standard for those with insufficient income. These rights-based schemes support working-age adults, low earners, jobseekers and those unable to work. Some countries offer a unified benefit, while others combine MIS with additional supports like housing benefits. The level of means-testing and conditionality varies, and many MIS schemes also help individuals find employment and access public services.
The fact that MIS are means-tested means they are complex to administer and require regular recertification (periodic reassessment of eligibility), which can lead to exclusion and low take-up (Coady et al. 2021). However, well-designed such schemes ensure a basic income floor, crucial for women in vulnerable situations. They work best within broader social protection systems that cover most of the population, and support those who fall through the gaps (Laenen and Gugushvili 2021). However, if their design is overly complex, this can significantly affect women’s financial independence, well-being, and autonomy (Razavi et al. 2022).
There is considerable scope for improving the gender-responsiveness of MIS and undoing bad design (see box 4.4). For example, individualizing the calculation and payment of entitlements will maximize women’s choices in determining the nature of their cohabitation arrangements. Removing aggressive “workfare” elements that compel women – through threat of benefit withdrawal – to take up just any job misses opportunities to provide time and space for them to reskill/retrain, and find good-quality jobs. And upon work resumption, gradual reduction of an MIS benefit as earnings rise, rather than an abrupt cut, can better promote women’s economic security as they transition back to work. Immediate benefit stoppage can create considerable financial stress.
Box 4.4. A problematic and a more promising MIS example
United Kingdom: The perils of complexity and non-individualized entitlements. The Universal Credit minimum income scheme has been criticized for excessive complexity, low benefit levels and a negative impact both on claimants’ mental health and on their finances, thus obstructing their labour market participation, perpetuating in-work and out-of-work poverty, and creating precarity traps (Alston 2019; Joseph Rowntree Foundation 2023). From a gender perspective, Universal Credit calculates benefits based on the household income of two cohabiting persons rather than that of the individuals (see Torry 2015). This ignores power asymmetries and assumes equitable resource distribution within households. Single payments to households can worsen gendered dynamics, particularly in cases of financial or physical abuse, leaving women with few alternative income support mechanisms (Alston 2019).
Spain: Incorporating gender-responsivity. The introduction of an MIS (Ingreso Mínimo Vital: Minimum Living Allowance) in 2020 has been welcomed as a key reform, despite concerns about sanctions, low take-up and limited impact on poverty (Bernhofer, De Minicis, and Molina 2023). These concerns aside, the scheme shows gender-responsiveness by waiving residency and work-seeking requirements for victims of human trafficking, gender-based violence or sexual exploitation, who are almost invariably women, and providing them with modest income security while they recover from their ordeals (OECD 2023; Waidler and Gavrilovic 2020).
Conditional cash transfer schemes
Conditional cash transfer (CCT) schemes have sparked debate regarding their impact on women (Cookson 2018; Molyneux 2006), with most discussions focusing on middle- and low-income countries, though most high-income nations also implement them (Medgyesi and Temesváry 2013). CCTs have shown positive impacts, such as reducing neonatal deaths and increasing preventive healthcare use (Standing and Orton 2018). Furthermore, non-compliance with conditions does not have to trigger a punitive approach leading to the exclusion of the beneficiary. Rather, conditionality can reveal vulnerabilities through the “recursive” function of the conditional mechanism (Orton 2014), prompting administrators to address gaps in services and thus improving access to rights like health and education. The Chile Solidario programme, now replaced by Ingreso Ético Familiar (Ethical Family Income),15 incorporates such a function. Ideally, CCTs should foster service referral systems centred on beneficiaries’ needs, simplifying access to support.
However, in practice even soft conditions can lead to exclusion and delayed payments, particularly for low-income women, who pay high transaction costs for complying with conditions like child vaccinations, or face a myriad of different obstructions to take-up. In Ecuador’s CCT programme, Bono de Desarrollo Humano (Human Development Bond), for example, some indigenous women did not collect their benefits because the private security guards of the financial institution mistreated them while they were queuing (Sepúlveda and Nyst 2012). Fear of abuse is also frequently reported by women with disabilities as a reason for non-take-up of benefits (UN 2019).
Critics argue that positive outcomes attributed to conditionality most likely derive from the cash itself, with little evidence that conditions significantly impact results (Hanlon, Barrientos, and Hulme 2010; Standing and Orton 2018; Pega et al. 2017). Studies show that unconditional cash transfers (UCTs) can achieve similar health outcomes without risking women’s rights or reinforcing gender inequality, potentially meaning that the same results in terms of health service take-up could be achieved by strengthened coordination between the social protection and health sectors (Pega et al. 2022). Conditionality is fundamentally inconsistent with freedom, and especially women’s freedom and empowerment, and even well-meaning paternalism often morphs into discretionary and arbitrary coercion (Standing and Orton 2018; ILO 2004).
Poverty-targeted programmes operating in lower-income contexts
In many low- and middle-income countries, poverty-targeted benefits like cash and food, or programmes of guaranteed waged work or economic inclusion, have proliferated (see subsections 4.7 and 4.8 on public works and graduation). These “social safety net” programmes often lack a legal foundation, relying on ad hoc funding and external donors. They frequently involve means-testing, including proxy means tests. These carry a high risk of exclusion errors (Razavi et al. 2022), disproportionately affecting women, especially those with disabilities. Research shows that such programmes often produce significant exclusion errors: out of 25 such programmes or registries covering less than 25 per cent of the population, 12 had exclusion errors above 70 per cent and 5 had errors above 90 per cent (Kidd and Athias 2020). An obvious antidote is to move from strictly targeted, means-tested benefits to categorical or universal schemes, which can help address the problem of exclusion or non-take-up of benefits by those who need them most, including women.
Emergency cash transfers during crises
Crises such as violent conflict, food shortages, climate shocks and health emergencies disproportionately affect women, and can reverse progress on gender equality (UN 2023; Gavrilovic et al. 2022). Women face heightened risks like displacement, gender-based violence, limited economic opportunities, harmful coping strategies (e.g., distress migration, asset sales), reinforced discriminatory norms and increased care burdens (Pereznieto and Holmes 2023).
Recent health crises like those caused by the Ebola and Zika viruses and the COVID-19 pandemic disproportionately impacted women, affecting their economic security, health and opportunities (Gavrilovic et al. 2022). Emergency cash transfers have become a common form of social assistance during these crises, accounting for 43 per cent of assistance during the pandemic (Gentilini 2022). However, these responses were often gender-blind, failing to address women’s needs effectively (UNDP and UN Women 2021). Some exceptions, like Togo’s Novissi (“Solidarity”) programme, offered higher benefits to women, making a modest effort to address gender inequalities (ILO 2020c). Countries like Argentina, Brazil and Kenya also prioritized women, with Brazil doubling benefits for female-headed households (Gavrilovic et al. 2022). Complementary measures to address increased domestic violence, such as rental support and access to safe housing, were implemented in countries like Ireland and Uruguay (Gavrilovic et al. 2022).
To ensure emergency cash transfers and humanitarian interventions are gender-responsive, gender considerations must be integrated into analysis, design, implementation and evaluation (Pereznieto and Holmes 2023). Without this, the burden of crisis adaptation often falls disproportionately on women, who act as “human shock absorbers”. Instead, the focus should be on systemic changes that empower women to thrive, not just cope, as part of a renewed social contract (Freeland 2012; Kim Allen 2022; Razavi et al. 2020).
Building comprehensive, gender-responsive social protection systems is crucial for preventing, managing and mitigating crises, supporting swift recovery and enhancing resilience. It is essential to link short-term relief efforts with long-term social protection development to address crisis-related risks for everyone, especially women. Countries with robust, gender-sensitive systems are better equipped both to handle everyday challenges and to expand support during crises (SPIAC-B 2022). Quite simply, countries with more robust social protection systems that have gender-responsiveness built into them are primed for ordinary challenges as well as being better positioned to expand significantly when a shock strikes (ILO 2021j; UN Women and UNDP 2022).
As the world faces increasing crises, especially due to climate change, social protection will play a vital role in softening their effects. Gender-responsive policies will be crucial, such as Algeria’s unemployment insurance for income loss from extreme heat, and India’s SEWA (Self-Employed Women’s Association) pilot scheme (ILO 2019c; Desai 2023). These measures will become even more important in the coming years, as countries grapple with the climate crisis and the need to provide vital income security and access to healthcare for all.
Designing and implementing social assistance programmes in a more gender-responsive way
The design of social assistance schemes varies significantly across countries but, based on the discussion above, the following policy recommendations can make these schemes more gender-responsive:
-
Policymakers should strive to render social assistance schemes rights-based and gender-responsive. This involves anchoring benefits in national law with clear eligibility criteria, benefit levels, and indexation, in line with human rights and international social security standards. They should be based on principles of transparency, accountability and non-discrimination (or positive discrimination when required to correct for inequality). Such legal frameworks support financial stability and better planning. This ensures timely access to benefits (to avoid ending up on waiting lists), especially crucial for women (Razavi et al. 2022).
-
Eligibility determination through means tests or proxy means-testing requires careful attention when building rights-based, gender-responsive social assistance schemes, particularly for vulnerable populations at risk of poverty. Anchoring such schemes in national law ensures the transparency, accountability and clarity of eligibility rules. Designs should account for specific vulnerabilities, such as disability-related costs. Even without legal anchoring, targeting can be improved by increasing transparency and accuracy in means-testing, establishing grievance mechanisms, and protecting people’s rights and dignity (ILO forthcoming, a). These measures help address the shortcomings of community-based targeting, which can lead to gender discrimination and lack of due process.
-
Transitioning from household-based to individual benefits, with individualized enrolment, calculation and disbursement, can better address women’s income support needs. A shift such as this would enhance women’s financial security, autonomy and decision-making power. Introducing individualized categorical benefits, such as social pensions, and exploring options for individual entitlement calculation and payment within social assistance schemes, can reduce reliance on household-based benefits and improve outcomes for women.
-
Gender-based increments in social assistance entitlements can be introduced for working-age women. In contexts of acute crisis and/or high gender inequality and systemic discrimination, this may be an important corrective option for women, as was the case during the COVID-19 pandemic, to address disadvantages in contexts where gender inequality intersects with other axes of inequality, such as indigeneity or ethnicity.
-
Awareness-raising helps maximize take-up and better framing of entitlements. To ensure women can effectively access social protection, efforts must be made to raise awareness about available benefits, eligibility and access, particularly for marginalized groups. Non-take-up of entitlements is a persistent issue, and governments, administrative staff, social partners, civil society organizations and women’s groups must help women understand the full range of benefits available to them. In doing so, specific attention should be given to removing elements that can be perceived as stigmatizing and shameful for women (Walker 2014), such as portraying poor people as “lazy” or “feckless”.
-
Transparent and simple design and procedures are essential to improve the gender-responsiveness of such schemes. This involves simplifying eligibility rules, removing sanctions or benefit suspensions, and streamlining enrolment to reduce women’s time burden and compliance costs. Decentralized structures and digital services can lower transaction costs, while prioritizing access for minority groups and people with disabilities enhances inclusion. Additionally, allowing women to enrol without needing permission from a so-called head of household is key to supporting women’s agency.
-
Enrolment in schemes on demand should be prioritized, as time-bound eligibility determination and registration processes are prone to result in the exclusion of those who should have access to benefits. If recertification for social assistance benefits is done only once every several years (Grosh et al. 2022), there can be massive delays in accessing income support, with devastating impacts, especially on the most vulnerable. This fails those, including women, who need support in the here and now, and for whom obtaining support years down the line leads to unnecessary suffering. Recent positive examples of new on-demand enrolment can be seen in Fiji and Pakistan (see box 9 in Barca and Alfers 2021).
-
Social assistance schemes play a vital role for women facing acute or chronic vulnerability, including those experiencing gender-based violence (GBV), forced labour, deep-rooted prejudice, or disability. To support these women, it is essential to ensure sensitive and accessible enrolment processes, maintain confidentiality and prevent discrimination. Staff must be trained to handle sensitive situations and link women up with social workers when necessary, especially for survivors of violence or trafficking. Additionally, women in these circumstances should have access to mainstream social protection and extra financial support as well as harnessing accompaniment models to address GBV and connect them to other services through social protection (UN Women 2023a). Survivors must receive full social protection benefits, wages for time spent in legal processes, and access to healthcare and other services, as seen in countries like Uruguay,16 Albania,17 and the United Kingdom (United Kingdom, Government of, 2022).
4.7 Public works and other public employment programmes
Public works programmes (PWPs), a part of social assistance, aim to support those at risk of poverty and are seen as a blend of active labour market and social protection policies. They focus on promoting employment, income security and public investment (McCord et al. 2024). From a social protection perspective, programmes that are rights-based and include an income replacement function if no work is available or if the worker is unable to work – for example in the event of maternity or sickness – are most relevant (see subsection 4.2). Employment guarantee schemes are highlighted in the ILO Social Protection Floors Recommendation, 2012 (No. 202), as key elements of national social protection floors. While PWPs provide paid workdays to unemployed or underemployed individuals/households, offering some income security, they are often criticized for not providing sufficient income replacement when work is unavailable. Moreover – with famous exceptions like India’s MGNREGS – almost none of the PWPs currently operating provides any form of income replacement if no work is available, or other contingencies occur as stipulated in Recommendation No. 202.
Traditionally popular in higher-income countries, PWPs are increasingly common in lower-income regions. Women’s participation is substantial due to their high rates of poverty and unemployment, and gender quotas in some contexts. In South Africa, over 60 per cent of participants in the Expanded Public Works Programme are women, and the programme played a key role during the COVID-19 pandemic by providing minimum-wage work (UN Women 2015b; South Africa 2023). It also offers employment and professional development through care services, particularly in early childhood development, though concerns about low wages and limited job availability for caregivers persist (Budlender and Lund 2012).
India’s MGNREGS (see subsection 4.2) have also exhibited some positive outcomes: increased labour force participation by women and by workers with disabilities, including women with disabilities, and improved women’s autonomy within the household, by providing higher wages than other rural employment opportunities (Ehmke 2015).
Yet one recurrent issue with some PWPs is the payment of the wage (or benefit) to the household as opposed to the individual, which looms large as a gender-unresponsive feature of such programmes. For example, Ethiopia’s Productive Safety Net Programme (PSNP) has in some of its iterations provided a household payment, irrespective of who performs the work. This has had implications for women’s access to income security and control over the money they earn (UN Women 2015b). Moreover, even when the PSNP tried to introduce women-friendly design features (Lemma et al. 2023) such as offering less demanding work and providing on-site day care, this proved much harder to implement in practice (see box 3.4 in UN Women 2015b).
While some PWPs have incorporated gender-responsive elements (FCDO et al. 2021; Barca 2019), many still fall short of being decent and human-centred. Issues like physically demanding work, lack of childcare facilities, risk of child labour, and trapping women in low-paying roles remain prevalent (FCDO et al. 2021). In lower-income settings, PWPs often focus on poverty alleviation rather than offering skilled work, unlike classical historical examples such as the United States’ New Deal in the 1930s.
Some argue that these programmes come dangerously close to coerced labour (Sengupta 2019). Their self-targeting logic – where only the most destitute are willing to perform such work – is not dissimilar to that of the British publicly financed workhouses (poorhouses) of the sixteenth to nineteenth centuries (Ravallion 2016), with particular challenges for women. Therefore, enhancing PWPs’ gender-responsiveness and providing more decent work opportunities are key areas for improvement. Options include the following:
-
Public works programmes must become more women-friendly, including for women with disabilities. Key improvements include providing on-site childcare and basic services, making individualized and prompt benefit payments, offering non-manual work with equal pay, and guaranteeing a minimum level of employment (Sengupta 2019; UN Women 2015b). In the long term, these programmes should lead to better-paying, decent jobs. Gender equality also requires valuing different types of work equally, ensuring that wages for care-related jobs are not lower than those for infrastructure work (Budlender 2009).
-
Ensuring decent work in PWPs involves fair wages, good working conditions, and social protection coverage. These programmes could help transform labour markets by addressing both the exclusion of certain groups and gender-based discrimination. They can offer better terms to the lowest segments of the labour market, establish a wage floor based on national minimum wages, prevent exploitative labour, and provide access to such social protections as maternity protection, sick leave, employment injury protection, unemployment benefits and pensions (McCord et al. 2024).
-
Facilitating the transition between PWPs and regular employment can be achieved both by providing opportunities for workers to develop and apply their skills and work experience in order to increase their employability, and by addressing barriers (McCord et al. 2024).
4.8 Graduation and economic inclusion programmes and “cash-plus”
In lower-income contexts, there is growing interest in gender-responsive social protection through graduation-type approaches aimed at promoting women’s economic inclusion. These integrated programmes utilize a “laddered strategic linkage” (ILO 2010) and include elements like cash transfers, microloans, WASH (safe water, sanitation and hygiene) measures, savings programmes, asset transfers, and various health, education and psychosocial interventions (e.g. legal advice on marriage and domestic violence). Notable examples include the Targeting the Ultra Poor Programme of the non-governmental development organization BRAC in Bangladesh and different incarnations of Chile Solidario, succeeded by Ingreso Ético Familiar, in Chile (see Government of Chile 2023).
BRAC’s approach has been extensively evaluated through RCTs, showing positive impacts like increased per capita income, food security, shifts to self-employment, and improved access to sanitation and clothing, as well as anecdotal gains in self-esteem, health and women’s empowerment (Soares and Orton 2017). However, these findings face significant criticism, particularly with regard to targeting efficacy, equity, “care blindness”, post-graduation outcomes, compliance with international social security standards and alignment with human rights (Soares and Orton 2017; Kidd and Bailey-Athias 2017; Laszlo 2019).
The debate over whether these interventions can foster gender equality continues. A key insight is the importance of an integrated approach, where social workers play a crucial role in helping marginalized women navigate gender inequality. However, this “hand-holding” requires a substantial social workforce. In densely populated Bangladesh, the short distances social workers must cover enhance efficiency and economies of scale, a model that is harder to replicate in other contexts.
Moreover, narrowly targeted graduation approaches raise concerns about the absence of effective, inclusive public services for all. Governments are accountable to their entire populations and may find that investing in broader benefits and services is a more efficient way to include vulnerable groups, address inequalities and build trust in public institutions (Behrendt 2017). More broadly accessible services, with strong institutional linkages to social protection systems, will be essential for a transformative approach (Holmes and Jones 2013, 215).
“Cash-plus” represents a trend towards integrating cash provision with information, knowledge and services to help families address diverse challenges. Evidence shows it positively impacts gender equality, poverty reduction, maternal health and economic inclusion, while reducing the incidence of women resorting to negative coping strategies like transactional sex (ILO and UNICEF 2023; FCDO et al. 2021). Such programmes can also foster positive attitude shifts among men and boys regarding gender norms, indicating that messaging alongside unconditional cash transfers can promote behavioural change without limiting women’s freedom. However, success relies on adequate funding for corresponding services. Often, when healthcare services without charges are included in those cash-plus packages, they are either a very limited set of services or they are fee waivers for which the facilities do not receive additional financing, leading to poor service quality, long wait times and increased mental load for women. These programmes also need to get better at recognizing and supporting care responsibilities, otherwise they risk increasing (combined paid and unpaid) work burdens on women. For all of the aforementioned reasons, the following policy considerations can help to render economic inclusion programmes more gender-responsive:
-
Ensuring continued social protection coverage after “graduating” from social assistance schemes, especially in the areas of health, maternity, unemployment and disability in line with Recommendation No. 202, and access to employment services, skills development and other support, to enhance productivity and the facilitation of transitions from the informal to the formal economy (Behrendt 2017).
-
Ensuring that support services are made available universally, not only for small groups of targeted programme participants, thereby avoiding exclusivity and community tensions. This requires investment in health, skills and public services to address inequalities, particularly for women, through a universal and inclusive approach.
-
Combining micro-level and supply-side interventions with macro-level and demand-side interventions to address the full range of barriers to employment and income security, thus helping to overcome the current limitations of economic inclusion programmes and achieve a real transformation of women’s livelihoods.
4.9 Universal basic income
With the exception of Mongolia,18 no national universal basic income (UBI) scheme has yet existed. This makes it difficult to discern its gender effects,19 and there have been many different proposals and pilots, each with different design parameters.20 UBI’s gender impacts can only be extrapolated through pilots and hypothetical supposition. While UBI could play a social assistance role and potentially help combat gender inequality, this will ultimately depend on its design, the level of the benefit provided and how it relates to other policies that attempt to tackle gender inequality and the gender structures prevailing in any national policy context (Kangas and Ylikännö 2023; Williams 2021). That said, this critique is not unique to UBI, and much existing social protection policy can and does reproduce gender inequality too, like the much-discussed CCT effects (see subsection 4.6). Nevertheless, there are different ways to think of UBI’s potential gender-responsiveness or lack thereof.
UBI has been proposed as a means to enhance women’s autonomy and economic security, thereby providing “real freedom” (Parijs 1997). Alston (2017) suggests that UBI could empower women with career choices and political voice by offering some degree of economic security and, critically, providing the financial means for them to leave abusive relationships. UBI is argued to pre-emptively address financial, life-cycle and gender-specific risks, offering continuous, preventive protection that reduces vulnerability and the risk of impoverishment before they arise (see Howard 2019; Standing 2011). UBI experiments have shown promise in producing good gender outcomes (see box 4.5).
Box 4.5. UBI pilot in India
A UNICEF and SEWA UBI pilot conducted in Madhya Pradesh in India in 2011–13 showed that women gained more than men, and girls more than boys, in terms of nutrition, health, access to healthcare and schooling, and economic inclusion, for example opening a bank account (see Standing and Orton 2018; Davala et al. 2015; Schjoedt 2016). For instance, individualized basic incomes seem to have helped assure girls of better access to nutrition, and thus improved their relative and absolute health status. Moreover, the pilots spurred the growth of new businesses or entrepreneurial ventures and own-account production, and this was particularly pronounced among women (Standing and Orton 2018).
In more advanced social protection systems, UBI might offer additional, proactive protection before the usual social insurance mechanisms kick in or a contingency arises, and potentially strengthen women’s bargaining power by increasing their reservation wage (Standing 2011; Gorz 1989; 1999). Adequate UBI benefits might also normalize time spent outside the labour market providing unpaid care and other unpaid activities, thereby promoting a fairer distribution of unpaid care work between women and men.
Conversely, critics argue that UBI might limit policy options for addressing gender inequality and reinforce traditional gender roles (see Gentilini et al. 2020; Bastagli and Hunt 2020), and has a lot of convincing to do when it comes to unpaid care work. Indeed, for some it seems far-fetched to suggest that UBI, in and of itself, would encourage recipients to allocate time to caring for others. Thus, like other social protection instruments, UBI might only induce more time devoted to care if incentivized to do so as per the “use it or lose it” paternity leave approach. With the exception of a “participatory” UBI – conditional on the performance of some socially valuable activity (i.e. voluntary work), as advocated by Atkinson (2015) – its proponents usually oppose conditionality. This might represent an obstacle for the direct incentivization of caring. Consequently, others argue that rather than UBI, governments should opt for the provision of universal basic services (Gough 2019), which might address gender inequality and unpaid care challenges better than UBI. Clearly, UBI alone cannot undo inequality in the labour market and in the provision of unpaid care. The merit of any UBI depends greatly on the specifics, including how it coheres with wider policy such as employment and care strategies to advance gender equality.
While UBI still appears to be some way off the policy agenda, it arguably has some gender-responsive insights to impart to social assistance schemes:
-
UBI’s design principles offer insights for more gender-responsive social assistance, since it potentially serves as a preferable alternative to the existing, highly flawed model, given its propensity to prevent poverty and life-cycle risk ex ante, its clear eligibility criteria, and the negligible probability that it would not be taken up or that it would create poverty or precarity traps. Indeed, many of its characteristics – being an individualized, unconditional, non-sanctionable and non-withdrawable payment – chime with the emerging consensus on what would represent gender-responsive design. But UBI’s gender-responsiveness could be increased by adding gender-based increments or supplements for families with children, adding incentives to support the sharing of care responsibilities, for instance. The main challenges for pursuing it lie in financing a meaningful and adequate UBI and implementing it in resource-limited or anti-universalist contexts.
-
Not just any UBI will do, and nor will it automatically tackle gender inequality. Implementing UBI with attention to international social security standards will ensure a rights-based approach, with at least minimum standards, adequate levels, accessibility and equitable financing. Ultimately, a UBI should be gender-responsive, support existing health and social protection, address specific needs like disability, and enhance access to the higher protections provided by social insurance (Ortiz et al. 2018; Orton, Markov, and Stern-Plaza 2024).
4.10 Making social protection systems serve the needs of working-age women
Greater efforts are needed to ensure social protection systems address the diverse needs of working-age women. Current gender-responsive discussions often limit themselves to social assistance or individual programmes (Cookson et al. 2023), missing the transformative potential of a systems-wide approach. While social assistance is vital as a last-resort benefit, and represents an important part of a social protection floor, it alone cannot ensure women’s economic empowerment. Evidence highlights the importance of combining social protection and labour market policies across the life cycle for more impactful outcomes for women.
Achieving gender equality requires shifting focus from merely reducing poverty to preventing it, and ensuring a decent standard of living for women. This involves breaking cycles of chronic poverty by providing access to decent work and higher social protection levels, such as social insurance (Diwakar and Shepherd 2021; ILO 2019a; 2021j), and addressing intersecting discrimination.
Improving non-contributory protection remains important, yet prioritizing social insurance and the transition to formal work is crucial for gender-responsive social protection and better outcomes for working-age women. Social insurance, based on collective financing, risk-sharing and legal entitlements, fosters gender equality. That it includes redistributive elements in its design is an important precondition for gender equality, which is not present in other contributory or employer-liability mechanisms. While there is still scope for improvement to make social insurance schemes more inclusive and gender-responsive (see section 2), it is important for women to be actively engaged in this process. Ultimately, a universal social protection (USP) system with a solid protection floor, sustainable financing and comprehensive benefits is essential for gender-responsive policies that address gender inequalities effectively for women of working age.
Income security and well-being in old age
Ageing has specific implications for women, as they tend to live longer than men and have lower earnings and fewer assets of their own, such as land. In view of persistent gender wage gaps and women’s typically lower lifelong earnings, linked to differences in their life courses and employment histories, the type and design of pension systems matters hugely for whether women are able to enjoy income security in old age (see section 2).
In addition to old-age pensions and access to healthcare (see section 6), to enjoy well-being and independent living many women (and men) who acquire physical and/or mental impairments also require effective access to good-quality long-term care without hardship.
5.1 Income security in old age: The gender pension gap
Figure 5.1 shows legal coverage for old-age protection by sex for the working-age population (15 years and older). One of the key points to emerge from this figure is that globally, while 60.1 per cent of working-age men have legal coverage in mandatory or voluntary contributory schemes and would therefore potentially be eligible for a contributory pension once they reach the prescribed age, this is the case for only 44.1 per cent of women. This gender gap reflects women’s lower labour market participation and their over-representation among the self-employed population and those working as contributing family workers (particularly in agriculture), as domestic workers, or in other occupations or sectors frequently excluded from the scope of existing legislation. Non-contributory pension schemes display a very small gender gap, which is in favour of women, yet often provide only modest levels of benefits (see section 2).
Figure 5.1. Legal coverage for old-age protection: Share of the working-age population aged 15 and over covered by old-age pensions, by income level, sex and type of scheme, 2023 or latest available year (percentage)
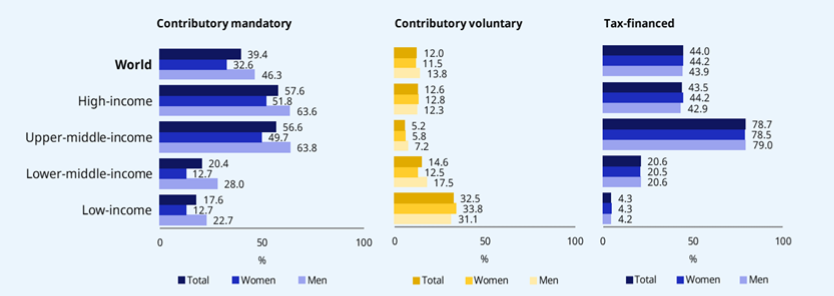
Notes: See Annex 2 of ILO (2024g) for a methodological explanation. Global and regional aggregates are weighted by working-age population aged 15 and over.
Source: ILO (2024g).
When it comes to effective coverage (see figure 5.2), the data shows that, globally, 63.2 per cent of men are receiving a contributory old-age pension as a share of persons above statutory retirement age, compared to only 49.2 per cent of women, but when it comes to tax-financed pensions, more women are receiving a benefit (34.2 per cent) than men (26.9 per cent).21 This overall picture holds when the data is disaggregated by region: in most regions and subregions, older women are less likely to receive a contributory pension than men (second panel) but, in many cases, they are more likely to receive a non-contributory (tax-financed) pension (third panel). Reflecting gender inequalities in labour markets, this gender gap is particularly pronounced in the Arab States, Africa and South Asia, where men are more than twice as likely as women to contribute, while South-Eastern Asia and the Pacific, Eastern Asia, and Latin America and the Caribbean display much smaller gender differentials (ILO 2024g, section 3.2.5).
Figure 5.2. Gender gaps in effective social protection and pension coverage: SDG indicator 1.3.1 on effective social protection coverage, beneficiaries of contributory and tax-financed pensions, contributors to pension schemes and labour force participation rates, by sex, 2023 (percentage)
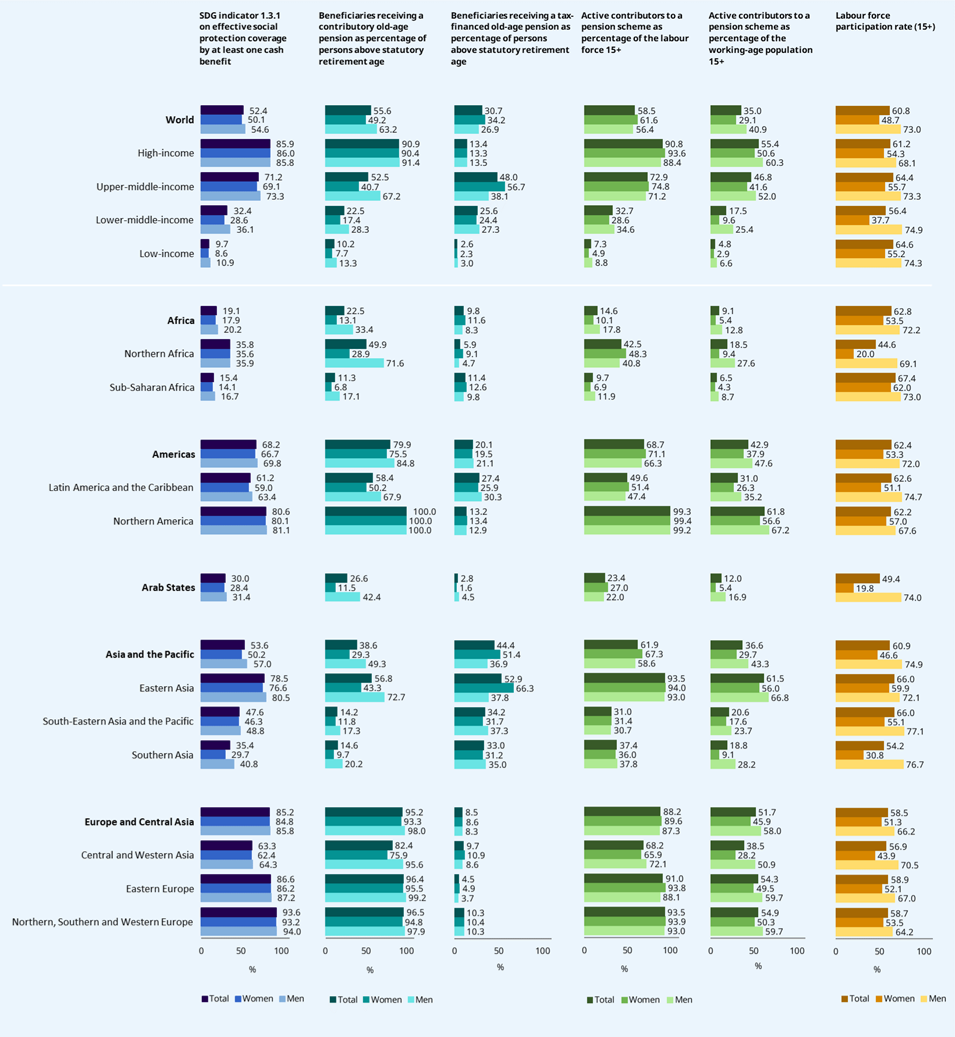
Note: Global and regional aggregates are weighted by population aged 65 and over for old-age beneficiaries; by working-age population and labour force aged 15 and over for contributors; and by working-age population for labour force participation rates.
Source: ILO (2024g).
As highlighted above, non-contributory pensions therefore play an important role for older women. Countries that have achieved universal or near-universal coverage of pensions, for both women and men, often combine contributory and non-contributory pension schemes. Countries such as the Plurinational State of Bolivia, Botswana, Lesotho, Namibia and the United Republic of Tanzania (Zanzibar) have established universal non-contributory, tax-financed schemes, and other countries, such as Cabo Verde, and Trinidad and Tobago, are close to achieving universality through a combination of contributory and non-contributory schemes (ILO 2021j). These experiences show that progress towards universal pension coverage, including of women, is feasible in low- and middle-income countries.
However, as section 2 showed, while tax-financed non-contributory pension schemes, especially when they are universal or pension-tested, can help close the gender gap in coverage, the level of benefit they provide can be low and insufficient as an income replacement mechanism, especially for those with higher levels of earnings. Based on a review of 100 schemes in 79 countries, we find that the average and minimum benefits represent merely 27.7 and 20.4 per cent of the minimum wage, respectively. In 38 countries, the minimum level of tax-financed pensions remains well below the national poverty line (ILO 2024g, figure 4.38 for selected countries). As a result, older people relying on a tax-financed pension for their income are still poor. This concerns close to 31 per cent of persons above retirement age: 34.2 per cent of older women and 26.9 per cent of older men.
It is important, therefore, that both contributory and non-contributory schemes are adapted to the realities faced by women, through their specific design features such as the reference salary used for benefit determination, the replacement rates applied, the rules for benefit indexation, and minimum benefit guarantees, as well as policies to recognize and compensate periods of care or care-related leave.
Furthermore, despite persistent gender gaps in coverage, social insurance schemes embody many features that are beneficial for women compared to other contributory mechanisms, such as individual savings schemes or private pension insurance. Such gender-responsive features include pension formulas that allow for a greater level of vertical and horizontal redistribution, care credits that recognize and reward periods spent caring for children or other family members (Fultz 2011), and minimum benefit guarantees.
For these reasons, if countries shift from social insurance schemes that are based on collective financing and have redistributive elements in their design, to privately administered individual accounts, the implications for gender equality can be adverse (Behrendt and Woodall 2015). This is both because benefit levels are directly based on past contributions and because the benefit formula usually considers the number of years during which the person is expected to collect benefits, penalizing women for earlier retirement and, in some cases, their greater average longevity through the use of gender-specific actuarial tables.
Low pension benefits are particularly challenging for women who acquire disabilities in old age, given that women tend to live longer and the risk of developing physical impairments grows exponentially at this stage of life. Most countries convert disability benefits into old-age pensions when a person reaches retirement age, without any consideration for the fact that older people with disabilities face a higher cost of living than those without impairment. Only a few countries allow the combination of a disability and old-age pension simultaneously, or provide a disability top-up to the old-age pension.
International labour standards22 provide an international reference framework for pensions and other social security benefits. They state that adequate old-age pensions should be provided at guaranteed levels, upon completion of a qualifying period, and be regularly adjusted to maintain pensioners’ purchasing power. In practice, evidence from the ILO World Social Protection Database shows that fewer than half of pension schemes reviewed (48.2 per cent) use price, wage or mixed indexation methods, while the majority resort to ad hoc adjustments, often influenced by political considerations, endangering the purchasing power of benefits, especially in inflationary contexts. Both the absence of regular indexation and the use of only ad hoc adjustments are concerning.
Based on the discussion above, the following measures can make pension systems more gender-responsive for greater income security for older women:
-
Following a comprehensive approach to ensuring income security in old age for women that guarantees both universal coverage and adequate benefits through a combination of contributory and non-contributory pensions in line with international social security standards.
-
Guaranteeing at least a basic level of income security through a nationally defined social protection floor. In the absence of other forms of pension coverage, non-contributory pensions, particularly in low- and middle-income countries, can help bridge the gender gap in pension coverage gap, though not necessarily the adequacy gap. In countries such as the Plurinational State of Bolivia, Botswana, Mauritius and Lesotho, universal coverage of pensions for both women and men is assured owing to the introduction of a universal non-contributory pension scheme.
-
Extending social insurance coverage to women workers who are not yet adequately covered, including those in part-time, temporary and self-employment, critical for securing adequate old-age pensions for women. Measures to extend social security coverage can support women in not only having access to decent employment during their working age but also accessing more adequate pensions in old age.
-
Removing elements of pension schemes that treat women and men differently, and which may have a harmful effect on women’s income security in old age, in favour of equal rules for men and women. For example, having different pensionable ages for women and men may limit women’s chances of accumulating pension entitlements, potentially resulting in lower pension benefits, whereas a higher pensionable age can enhance the adequacy of their pensions. Replacing sex-differentiated mortality tables with unisex ones can also contribute to more equity. Regulations that encourage or force women to withdraw their pension contributions upon marriage also jeopardize their prospects of enjoying income security in their own right as well as increasing their dependence (Behrendt and Woodall 2015).
-
Strengthening elements of pension schemes that recognize and reward care responsibilities, with a positive impact on gender equality, especially where they are accompanied by measures to encourage the more equal sharing of care responsibilities between women and men. This includes, in particular, care credits in pension schemes, which offset the impact that a full or partial reduction of working time has on pension entitlements, resulting in longer contributory periods and higher pension benefits.
5.2 Access to long-term care and its critical role for gender equality
Social protection systems have an important role to play in providing support to healthy ageing, taking different forms depending on the country context. Such policies can do this in at least three important ways: first, by supporting the social determinants of health throughout the life cycle,23 for example by providing income security in the event that a person loses their job or becomes sick; second, by enabling access to long-term care (LTC) without financial hardship for the older persons who need such support; and third, by being inclusive towards caregivers in all their diversity, to promote equal opportunities for women and men and be supportive of workers with family responsibilities (Tessier, De Wulf, and Momose 2022b).
Women are over-represented among the older population in all country income groupings, especially as they advance in age (UN Women 2019a). They are also more likely than men to report disabilities and difficulties with self-care, owing to their average greater longevity and the steep rise in disability after ages 70 to 75 (Vos et al. 2020). At the same time, older women are more likely to live alone (higher life expectancy plus partnering with men who are older than they are means they are more often widows), not being able to rely on support from other household members, especially partners. The range of care they need may be wide and go beyond healthcare services to include social care and support in adapting to their living environment (Perracini et al. 2022). Benefits packages under social health protection and, where they exist, LTC schemes need to be well coordinated and ensure continuity of social and healthcare, including geriatric and institutional care when needed. Failing to do so would drastically reduce the gender-transformative potential of such schemes.
There is limited data on legal and effective coverage for long-term care. Globally, only 89 of 179 countries have statutory provision for public LTC services for older persons. This is equivalent to almost half the elderly population with potential care needs living in countries with statutory LTC services (ILO 2022a).
Countries that have invested in LTC schemes have done so with a variety of institutional and financing arrangements (Tessier, De Wulf, and Momose 2022b) (see box 5.1). These include dedicated LTC schemes; top-up pension benefits and/or expansion of the scope of disability benefits; and LTC provision embedded within social health protection benefits packages. These schemes can either encompass the effective provision of LTC services or provide a cash benefit that can be used to buy services from LTC providers. The LTC services that can be provided lie on a continuum ranging from intensive institutional care (e.g. nursing homes) to less intensive institutional care (e.g. short-stay respite care) to community services (e.g. day centres or nurse and professional carer visits) to home-based services (e.g. cash benefits for carers, or home help) (Lloyd-Sherlock 2017). In most cases, the effective provision of good-quality LTC services without hardship requires strong coordination between income support and healthcare schemes, as well as high levels of integration between health- and social care. Insufficient investment in both areas leaves important adequacy gaps, even in countries where LTC is recognized as a life-cycle contingency in its own right.
LTC benefits cover the contingency of a significant decline in a person’s capacity, which requires care and support in order to live a life consistent with human rights and dignity. In practice, countries have defined different rules governing eligibility to LTC benefits, providing concrete interpretations of such contingencies. The ability to carry out activities of daily living (ADLs) – such as eating, bathing, dressing, toileting, moving about and continence – is generally used as a key metric to assess the need for both care and social services (ISSA 2022). An important aspect of assessing loss of function is to be able to effectively reflect the need for LTC. For instance, taking into account the impacts of mental illness, including dementia, and not only physical impairment, is crucial. Similarly, taking into account environmental constraints, which are often overlooked, can be central to making an adequate assessment of LTC needs, which is of particular importance to women, who are more at risk of dementia in older age (WHO, n.d.).
Of the 89 countries that have statutory provision of public long-term care services for older persons, 30 finance it either through social insurance only (seven countries) or in combination with general taxation (23 countries) (ILO 2022a). In addition, only 29 countries have established a statutory, universal and free LTC service scheme. Even when these services are legally mandated, out-of-pocket costs remain high, putting older persons and their families at risk of income poverty, hardship and adverse health conditions.
Financing arrangements for LTC are not neutral. The benefits of shifting the costs from the individual (and family) onto society can be seen as a gender-transformative investment by enhancing both equity and dignified and active ageing. While this holds true, it still requires the identification of equitable and sustainable sources of public financing that will allow for the sustainability of such an investment over time without jeopardizing existing benefits. This has been identified as a challenge by many countries that have implemented LTC schemes (Kerry Allen et al. 2011; Joshua 2017; W. M. Walker and Wyse 2021). For instance, in Singapore the long-term disability insurance scheme imposed differential contribution rates for women and men on the basis of the differential in life expectancy, regardless of the overall socio-economic and employment situation of women (ILO 2021e). Beside raising issues of equity, this penalizes women, who have a higher life expectancy but not the financial capacity to attain higher contribution rates, flying in the face of the solidarity principles that should guide social insurance.
Box 5.1. Building LTC systems: National variations in institutional and financing modalities
The Republic of Korea and Japan provide useful examples of LTC policymaking. Both countries have national long-term care insurance (LTCI) schemes that are partially funded or subsidized by the Government. In the Republic of Korea, the Government funds around 20 per cent of the annual budget for the scheme; in Japan, it is approximately 50 per cent. The remaining budget in both cases is funded by LTC social security contributions from employers and workers (Tessier, De Wulf, and Momose 2022a).
Affiliation to the LTCI scheme in the Republic of Korea is mandatory for individuals aged 65 or older, or under 65 and suffering from debilitating conditions. The LTCI package also provides a wide range of services, such as home and institutional care. Uniquely, LTCI also includes cash benefits for family members who support beneficiaries, provided they have received training. This has led notably to a reduction in unpaid care work, which is usually performed by female family members (UN Women 2019a).
The Japanese LTCI system also provides a range of care services to beneficiaries, although cash benefits for family members are not included – a demand of women’s rights advocates to avoid reinforcing women’s already heavy family duties (Abe 2010). The broad categories of benefits covered by LTCI are home care, daycare, respite care, services at LTC facilities, equipment such as wheelchairs and assistive devices, and home adaptation and community-based preventive services.
The LTCI systems in Japan and the Republic of Korea owe their origin to the rising cost of unnecessary hospitalization weighing on the healthcare budget, as well as growing awareness of the burden of unpaid care that was being placed on family members, particularly women. Coupled with heavy out-of-pocket payments, this made accessing long-term care increasingly difficult for older persons and their families.
While these two countries provide useful lessons, there are many which do not have statutory provision of public long-term care services for older people. In the context of rapid population ageing in many middle-income countries, LTC needs are being met through a mix of under-regulated responses from the private for-profit and not-for-profit sectors, with results that are highly uneven and not accessible to all (UN Women 2019a).
India, for example, faces a burgeoning and unregulated private care sector. There is a growing demand for care services for older people. Recent research in Tamil Nadu, Karnataka and Kerala shows that there is a large presence of the for-profit sector when it comes to providing LTC. Services, however, are only available to those who can afford them, leaving a large section of India’s older population without adequate care and vulnerable to the interlinked risks of poverty, old age and gender. Furthermore, the lack of regulation and minimal involvement of the State have led to high variability in the quality of services provided (Baru, forthcoming).
South Africa has also seen a growth in LTC facilities that are mainly run by the not-for-profit sector. Of the 400 officially registered care homes in 2019, only eight were run directly by local or national government agencies. The focus in LTC provision remains on wealthier older people who can afford to pay for these services, again leading to a lack of or inadequate care for poorer people. There are also growing concerns about the increasing numbers of informal, unregistered care homes (Lloyd-Sherlock 2019). The unregulated growth of private for-profit and not-for-profit care services has implications both for the quality of care received by older persons, and for the wages and working conditions of the care workforce.
At the same time, there is increasing evidence of the benefit that comes from integrating LTC and mainstream health services for older people (Lloyd-Sherlock et al. 2022). Since 2011, the Brazilian city of Belo Horizonte has been running an innovative scheme to support care-dependent older people in vulnerable communities: the Older Person’s Care Programme (Programa Maior Cuidado – PMC), developed and run jointly by the departments of Health and of Social Assistance. Families receive up to 20 hours a week of support from professional care workers. Research suggests the PMC is popular both among professionals in the system and families and beneficiaries themselves. It also shows it to be effective in reducing the burden on family members and enhancing the quality of life for older persons. Care workers are provided with basic training, decent wages and labour protection, with enormous benefits for their quality of life and that of their families. At the same time, the fact that the care workers are all women tends to reinforce the feminization of care work (Lloyd-Sherlock et al. 2024).
The costs of inaction
While women tend to be disproportionately represented among those needing LTC, they also constitute the majority of those providing it, both as (unpaid) caregivers and as (paid) care workers. Both factors make the gender dimension a priority issue for building LTC systems that are rights-based, inclusive and financially and socially sustainable (Tessier, De Wulf, and Momose 2022b).
The absence of LTC coverage often results in women having to care for older family members, with limited support or respite, which can have adverse impacts on their physical and mental well-being, as well as their participation in paid work and their income security (ILO 2018a). What is more, in 70 countries the law embeds legal obligations for family members to care for older relatives, intensifying women’s care responsibilities and relinquishing collective responsibility (ILO 2022a). Unpaid carers, providing many hours of care per week, are less likely to engage in employment and more likely to suffer from mental health problems, with women disproportionately affected. When unpaid carers have a job, it is more likely to be part-time, leading to lower salaries and fewer opportunities for promotion. This illustrates that LTC always has costs, even if it is provided by family members on an unpaid basis. It is therefore a priority to find ways to share these costs more equitably across society (UN Women 2017a).
Similarly, the paid care workforce is predominantly made up of women. They constitute around three quarters of people working in health and social care services in OECD countries, often working in lower-paid jobs (OECD 2020). In the European Union, almost 90 per cent of the LTC workforce are women (European Commission 2021). In the United States in 2017, of the approximately 1.5 million people employed in the LTC sector, 90 per cent were middle-aged and female and 20 per cent were foreign-born (UN Women 2017a).
At the same time, while the need for qualified staff and the shortage of professional staff are growing, working conditions have to improve to make the sector more attractive. Deficits in working conditions and low pay in LTC provision are common, which contributes to gender gaps in both pay and pensions later in life. Hence, addressing the challenges of the LTC workforce would also help tackle gender inequalities in the labour market. How LTC is financed and provided has a major impact on women’s ability both to live a dignified life and at the same time to sustain their participation in the labour force, by helping to reconcile paid employment with unpaid care responsibilities and meeting the rising demand for care.
Based on the discussion above, the following measures can make LTC systems more gender-responsive:
-
Promoting the well-being, dignity and rights of care-dependent older persons, while respecting the diversity of needs and enhancing independent living. Not all frail older people need intensive institutional care.
-
Enhancing the accessibility, affordability and quality of LTC services, recognizing the need both for financial protection against their cost and to expand their availability through better regulation and enhanced solidarity in financing, regardless of whether services are provided by public, private for-profit, or not-for-profit providers.
-
Respecting the rights of LTC workers, by addressing the low pay and deficits in working conditions and social protection that are endemic to that workforce.
-
Reducing the heavy responsibilities that are placed on unpaid family carers, by giving them respite and facilitating their participation in the labour market, including also those who need support themselves, such as carers with disabilities.
Gender-transformative social health protection
Social health protection provides a rights-based pathway towards the attainment of Universal Health Coverage (UHC) (ILO 2020f; 2024g, section 4.4). As an integral component of comprehensive social protection systems, social health protection (SHP) designates a series of public or publicly organized and mandated private measures to achieve the following (ILO 2008):
-
effective access to high-quality healthcare without hardship, which is the focus of this section; and
-
income security to compensate for lost earnings in the event of sickness (see subsection 4.5).
The lack of affordable high-quality healthcare risks creating both poor health and impoverishment, with a greater impact on the most vulnerable, among whom women tend to be disproportionately represented (ILO 2021j; 2024g). For this reason, the principle of universality of coverage has long been underlined in international social security standards (ILO 2020f).
Gender is a dimension that is particularly relevant to the design and implementation of SHP schemes and their universalization (ILO 2020f; Tessier et al. 2013). In turn, well-designed SHP schemes can make an important contribution to greater gender equality in both access to healthcare services and health outcomes (ILO 2021j; 2024g). Adopting a gender perspective requires consideration of the gender-specific healthcare needs of women and girls and the particular barriers they face in accessing services, as well as consideration of the broader social determinants of health inequities:
-
Some of the healthcare needs of women and girls are gender-specific. A case in point is the specific ones related to reproductive, maternal, newborn and child health (RMNCH). The lack of adequate medical care in the prenatal, delivery and postnatal periods can put women’s lives at risk. Sexual and reproductive rights and services, more broadly, are central to the empowerment of women and adolescent girls and their ability to make informed choices about reproduction (Temmerman, Khosla, and Say 2014). Similarly, women tend to experience greater longevity than men and are therefore more likely to need geriatric and sometimes long-term care (WHO 2021). Considering women’s lower social and economic status and more restricted opportunities in many societies, and not least discrimination and sometimes violence, they also tend to have specific mental health needs and are at higher lifetime risk of depression and other mental health disorders (GBD 2019 Mental Disorders Collaborators 2022).
-
In addition to their gender-specific healthcare needs, women and girls need access to a wide range of healthcare services that cater to everyone (WHO 2009). Still, women may experience specific barriers in some contexts, such as lack of financial resources to access healthcare services, social norms that impede access to a male healthcare professional even where this may be the only service provider, differential treatment from healthcare providers (such as breach of confidentiality, lack of respect, discrimination in service access and quality), or simply the neglect and de-prioritization of their healthcare needs within limited household budgets (WHO 2009). Women also tend to experience higher levels of time poverty than men, which therefore impacts their ability to access healthcare services that may be far away and/or involve long queues (UN Women 2019b).
-
While women across the world tend to live longer than men, they do not necessarily live healthier lives (WHO 2009). The health of women as well as men is determined by physiological factors but also largely by many that lie outside the confines of the health sector, often referred to as the social and economic determinants of health (Marmot 2001). Indeed, gender inequality more broadly and gender-based violence more specifically have been framed as social determinants of mental and physical health. Likewise, poverty, social exclusion and inequality negatively impact on health and well-being, because they affect nutrition, education, housing, health-seeking behaviours, stress levels and other social determinants of health (Commission on Social Determinants of Health 2008). For women, lack of access to maternity, sickness, disability and other cash benefits, as well as deficits in occupational safety and health (see section 4), often mean greater morbidity, unmet healthcare (and care) needs and insecurity during their working lives, and the accumulation of disadvantage as they age. Likewise, not having access to an adequate pension (see section 5) translates into poor diet and substandard living conditions that undermine women’s healthy ageing (Tessier, De Wulf, and Momose 2022a). By directly tackling these factors and facilitating access to health services, social protection plays a critical role in promoting health equity and well-being.
The Sustainable Development Goals framework integrates these dimensions under two complementary goals, on UHC (SDG 3.8) and USP systems, including floors (SDG 1.3). The two are intimately interlinked, as priority measures to enable people to lead healthy and dignified lives, and at the heart of both sustainable development and social justice (ILO 2017).
The ILO Social Protection Floors Recommendation, 2012 (No. 202), recognizes effective access to essential healthcare as the first of four basic social security guarantees constituting national social protection floors that should be made a universal reality as a matter of priority (ILO 2021d; 2019b; 2017). Acknowledging this important step in forging an international consensus around UHC, in 2012 the United Nations General Assembly adopted a Resolution on Global Health and Foreign Policy, which underlines “the importance of universal coverage in national health systems, especially through primary health care and social protection mechanisms, including nationally determined social protection floors”. The following sections will explore those two dimensions, namely population coverage and adequacy of benefits, before looking at available indicators in terms of effective access and utilization from a gender perspective.
6.1 Inclusive population coverage
Legal and effective access to adequate social health protection is critical for gender equality. Monitoring progress in such protection requires considering population coverage and adequacy of benefits, both in law and in practice. The complexity and interdependency of these dimensions, as well as the lack of systematic data collection on many of them, make social health protection coverage difficult to monitor (ILO 2021j). SHP population coverage is concerned with the proportion of the population that is entitled, in law and in practice, to a comprehensive benefits package with no (or very limited) co-payment, in facilities that meet the human rights criteria of availability, acceptability, adaptability and quality.
Based on a legal review in 164 countries, 83.7 per cent of the global population is legally entitled to access healthcare services without hardship (ILO 2024g, fig. 4.41). Therefore, one in five individuals lives in a country that does not legally recognize such entitlements. Rates of legal coverage for social health protection are high in all regions, though lower in low-income countries. SHP legal frameworks tend to convey a universalistic vision of coverage, without discrimination or exclusion based on gender. A rights-based approach to SHP has the potential to reinforce gender-transformative policies by recognizing women’s right to claim healthcare at the point of service provision. Expanding legal coverage in low-income countries should therefore be a priority as it contributes to women’s empowerment.
For individuals to effectively access health services without hardship when needed, it is important for such access to be considered a right and to be embedded in the legal framework. It is equally important for individuals to be aware of their legal entitlements and the modalities to avail themselves of such entitlements. A proxy indicator is the share of population protected by a social health protection scheme, based on a combination of administrative and survey data. In striving for universal protection, a large number of countries across all income levels have made laudable progress in extending the effective reach of social health protection mechanisms over the past decades, resulting in almost two thirds of the world’s population being protected by a scheme. However, the global coverage rate has stalled, with almost no progress since 2020 (see figure 6.1). Coverage varies greatly across country income groupings, showing stark inequalities and an uneven trend between 2020 and 2023. Coverage in low-income countries even decreased slightly. Therefore, more than four in five persons in low-income countries are left unprotected. Slight progress in high-income countries was driven by the implementation and progressive take-up of the amendments to the Affordable Care Act adopted in the United States. While coverage slightly increased in lower-middle-income countries, there was a setback in the upper-middle-income category, driven by a decrease in coverage in China, where it remains voluntary for some population groups. Southern Asia and sub-Saharan Africa remain far below global averages. Low- and lower-middle-income countries, as well as sub-Saharan Africa and Southern Asia, experience the largest gaps between legal coverage and effective protection, illustrating difficulties in enforcing legal frameworks and in giving effect to people’s rights in practice.
Figure 6.1. Share of the population protected by social health protection (protected persons), regional estimates, 2023 or latest year available (percentage)
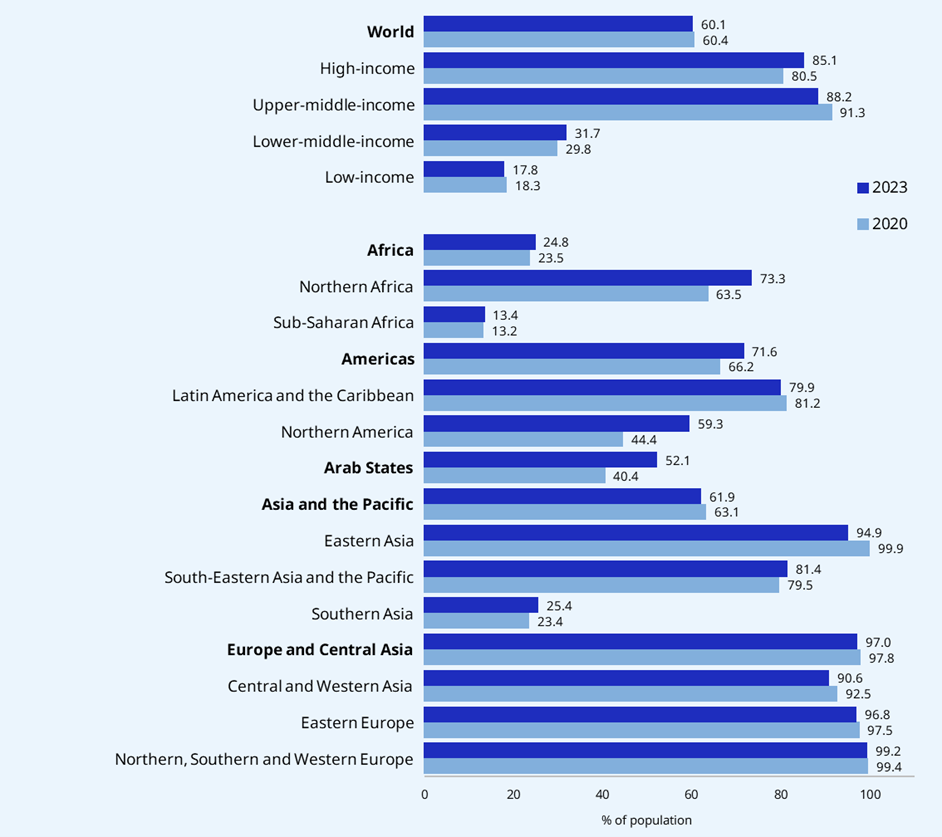
Notes: Based on data collected for 127 countries and territories, representing over 90 per cent of the world’s population. Regional estimates are weighted by total population. The figure represents the best estimate of people protected by a healthcare scheme for their primary coverage. Mechanisms include national health insurance; social health insurance mandated by the State (including subsidized coverage for the poor); national healthcare services guaranteed for free or with small co-payments; and programmes such as user fee waivers and vouchers. For primary coverage, 202 schemes were identified and included. This is substantially more than in 2020. Therefore, in order to generate trends, the 2020 estimates were recalculated, including the new countries and schemes for which data points are available in both periods. Only public or publicly mandated privately administered primary healthcare schemes were included. Supplementary public and private programmes were not.
Source: ILO (2024g).
Given the lack of sex-disaggregated data for the majority of countries in the world, it is not possible to monitor gender disparities in coverage rates at the regional level or across country groupings based on income. Analysis of available data for 58 countries shows that a lack of money to pay for health services is given as a reason for forgoing healthcare among women aged 15 to 49 across the household income spectrum. The pattern follows a clear social gradient, with over 65 per cent of women in the lowest income quintile offering the same explanation, while almost 30 per cent in the richest quintile mention it (WHO and World Bank 2023). Distance to a health facility was also adduced by almost half of the rural women surveyed, while having to take transportation was brought up by 40 per cent of them (WHO and World Bank 2023). Upholding the right to social health protection is therefore of utmost importance in countries’ endeavours to address health-related gender inequality.
It is clear that there is still a long way to go to make the right to social health protection a universal reality: 2.7 billion people are not protected by any scheme. As with other branches of social protection, more and better disaggregated data by sex and other indicators (age, location, income, migration and disability status, among others) is needed in order to identify the population groups that remain excluded, and to devise inclusive policies (Lozano et al. 2020).
While legal and regulatory SHP frameworks usually provide equal entitlements regardless of gender, labour market participation, employment patterns and other socio-demographic and socio-economic factors may lead to unequal outcomes for women and men:
-
Gender inequality in employment patterns, as we have seen (section 2), may create gaps in effective coverage when access to SHP systems is related to employment, without adequate measures to subsidize the contributions of low-income workers (ILO 2021e).
-
Similarly, some SHP schemes affiliate on an individual rather than a household basis, leaving spouses (often women) and children uncovered, as in the social security systems of Cambodia and Myanmar (ILO 2021e).
-
Where SHP systems are contributory, it is crucial that contributions be set at an adequate level and that full subsidies be in place for those with no contributory capacity. Many countries with universal health insurance schemes have shown that this is feasible, ensuring that an adequate financing mix is put in place. Social security contributions to healthcare schemes are fully or partially subsidized for workers in the informal economy and/or in self-employment in a number of countries, including Costa Rica, Indonesia, Kazakhstan, Thailand and Viet Nam. In some specific instances, this is coupled with presumptive tax regimes, as in Kazakhstan or Uruguay (ILO 2021e; 2024d; forthcoming, b).
-
Where social assistance measures to subsidize contributions are available, women may be over-represented in schemes targeting those who are poor and/or inactive, which often have lower levels of protection and may not be anchored in legislation (ILO 2021j). It is therefore crucial that entitlements be rights-based and with universal population coverage, regardless of the financing modalities of the scheme.
-
In some resource-constrained contexts, governments have put in place programmes affording free care for pregnant women and young children, or have lifted user fees for specific RMNCH services (Frota et al. 2020). Those efforts are laudable and have contributed to the progress made on maternal and child health outcomes. Still, without a comprehensive system in place, such schemes leave women and girls uncovered outside of the pregnancy and early childhood periods (ILO 2021j).
-
When fee waivers for specific services are put in place (i.e. in the framework of conditional cash transfers or of dedicated programmes to improve maternal health), it is crucial that healthcare facilities be adequately compensated financially for such services to avoid this translating into poor-quality services and inadequate treatment of beneficiaries. The Linda Mama programme in Kenya is a positive example in this respect.
6.2 Adequate and responsive benefit design
When it comes to SHP, an entitlement is actualized through a clear definition of (i) the package of benefits corresponding to the contingency, namely the range of health services that are made accessible, (ii) a dedicated network of service providers in charge of service delivery (i.e. from whom services can be obtained which meet certain quality criteria), and (iii) the level of financial protection provided to cover the costs of this benefits package. The adequacy of SHP coverage in terms of its contribution to gender equality is largely contingent on these important design parameters, explored below.
6.2.1. Ensuring availability and utilization of a comprehensive range of services
Service coverage and utilization: Where are we globally, and how does it impact women?
Effective and comprehensive monitoring of service access, allowing for direct comparisons between legal SHP entitlements and effective access meeting the criteria of availability, accessibility, acceptability and quality in a comparable manner within and across countries, is not available. Rather, most countries produce and analyse data on the availability and utilization of some specific “tracer” health interventions and services (WHO 2022b).
Many countries have progressed in terms of providing effective access to RMNCH services, largely encouraged by the Millennium Development Goals (MDGs), with the fastest increase in low-income countries (WHO 2019b). Yet important inequities in access remain, both across regions (see figure 6.2) and across wealth quintiles (see figure 6.3). More efforts are needed to ensure access to free, good-quality maternity care in line with ILO standards, to expand maternity cash benefits and to improve coordination between pre- and postnatal care and income security schemes (see section 4). Specific consideration needs to be given to certain groups of women who are at higher risk of exclusion, like women with disabilities, women from migrant or refugee communities, and women living in rural areas, among others.
Specific analysis is still needed at country level to measure gaps in effective access and potential inequities in healthcare utilization, as well as carrying out qualitative studies on gender-based discriminatory practices at the point of service. However, trend analysis of SDG target 3.8.1’s sub-indices on RMNCH (encompassing family planning, antenatal care, diphtheria–tetanus–pertussis (DTP3) immunization and acute respiratory infection care-seeking) shows very slow progress in the availability of such services over the past two decades (period 2000–21) (WHO and World Bank 2023). The average annual changes have remained below 1 per cent since 2000 and none has been observed since 2015. Also, large inequalities between countries persist, with much better access to services in high-income countries while low- and lower-middle-income countries lag behind.
Similarly, within countries, inequalities persist by economic status, education and place of residence (urban/rural). The analysis of a subset of 78–89 (depending on the disaggregation) countries for which disaggregated data is available shows that there is a striking social gradient in access to RMNCH services, with an almost 15 percentage points difference between the highest (median coverage of 73 per cent) and lowest (58 per cent) quintiles, and an overall 3–4 percentage points difference between each quintile. There are inequalities between urban (70 per cent) and rural (63 per cent) populations and also between those with no education (56 per cent) and those with secondary or higher education (71 per cent) (WHO and World Bank 2023). Patterns of inequality also prevail when considering intersectional discrimination. For example, women with disabilities are found to be regularly excluded from the provision of sexual and reproductive health services and face the additional risk of involuntary sterilization (UN 2019, 1, 7, 71).
Figure 6.2. Unequal advances in service coverage for reproductive, maternal, newborn and child health services, by region and type of service, 2023 or latest available year (percentage)
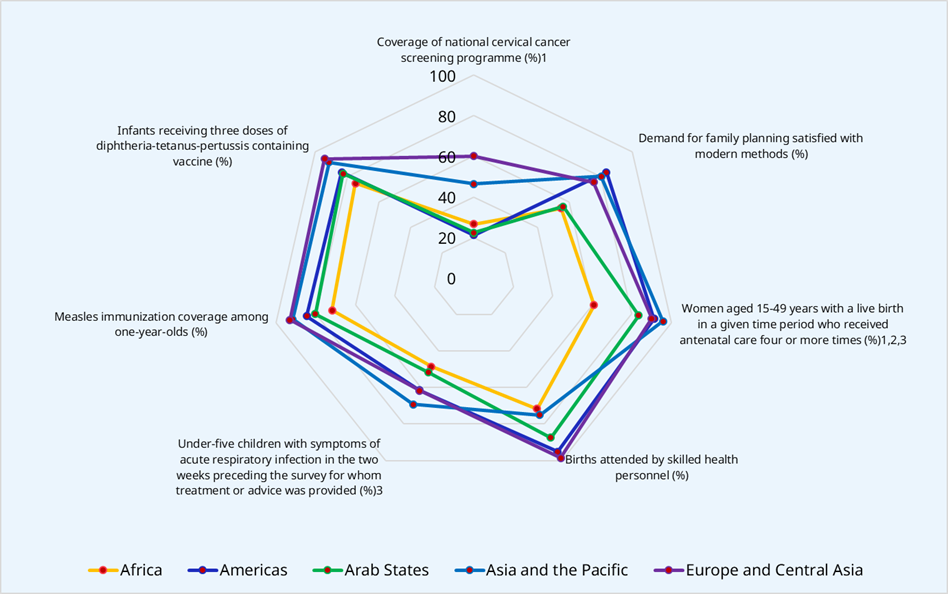
Notes: To be interpreted with caution – estimates based on reported data coverage below 40 per cent of the population: ¹ Africa and Arab States; ² Europe and Central Asia; ³ Asia and the Pacific, and Europe and Central Asia. Regional estimates are weighted by total population.
Source: ILO (2024g).
Figure 6.3. Inequities in access to maternal healthcare services: Share of live births attended by skilled health personnel by wealth quintile, selected countries by region, 2019 or latest available data (percentage)
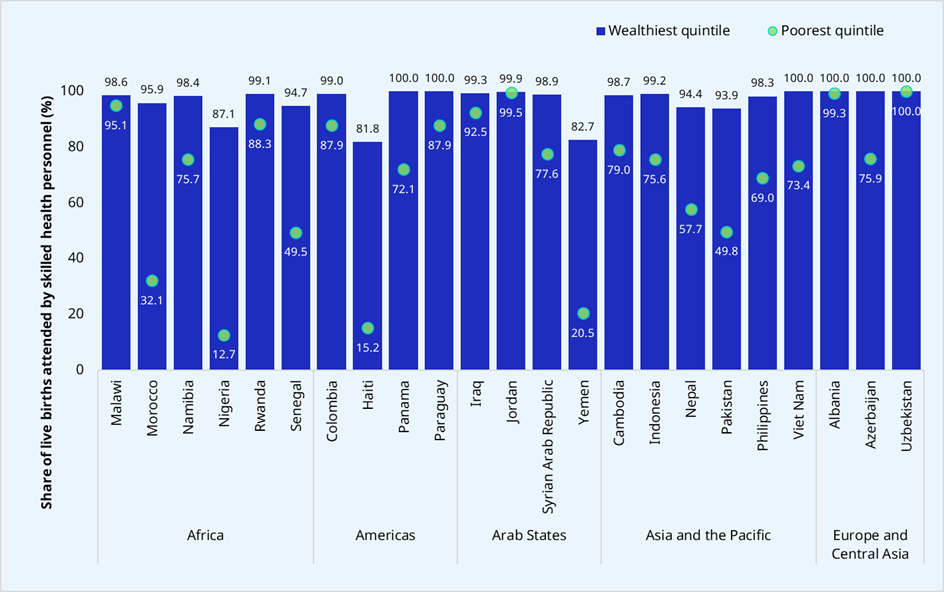
Source: ILO (2024g).
Lastly, high SHP population coverage does not necessarily translate into equitable access to services and health outcomes. This relates to the distribution and quality of facilities and services – supply-side variables. While significant efforts have been made to make health services and related infrastructure available and accessible in rural areas and remote locations, still the issue of adequate distribution of services and retention of a skilled health workforce poses a challenge, as illustrated by figure 6.4. As figure 6.5 shows, rural–urban inequities in the availability of health workers also remain significant in many countries, with rural populations often not having a commensurate share of the country’s health workers. In Nepal, for example, while around 80 per cent of the population resides in rural areas, only around 25 per cent of the health workforce is based there. The location of health services is of particular concern to women: when services are far away, both transport costs and safety risks may prevent them from seeking care, particularly in the case of women living with disabilities (Geleto et al. 2018).
Figure 6.4. Hospital bed and selected skilled health professional density by country income groups, 2022 or latest available year
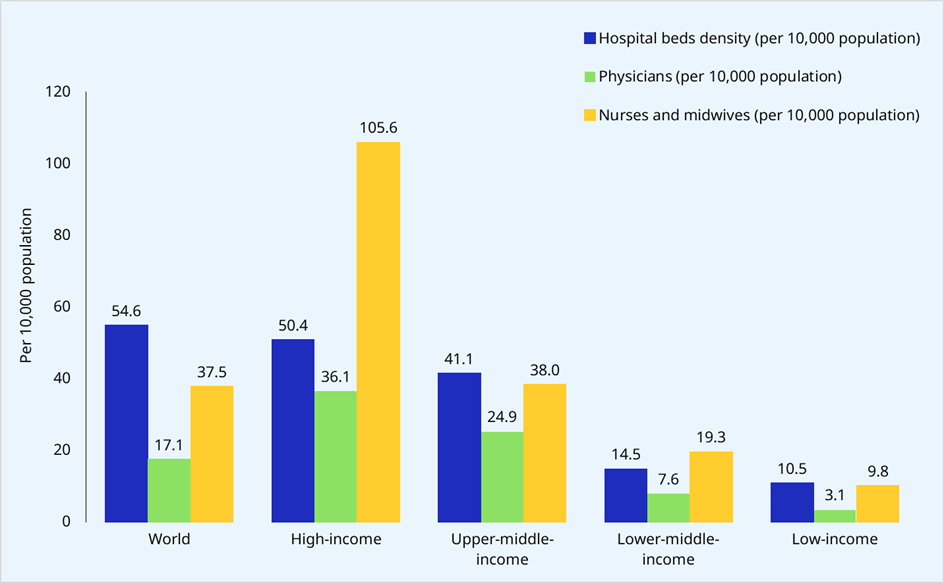
Notes: More details on the use of these reference points can be found in GHWA and WHO (2013). The European average represents 28 countries for which data was available (see Annex 2 of ILO (2024g)). See also ILO (2023c). Income-level estimates are weighted by total population.
Source: ILO (2024g).
Figure 6.5. Inequities in the availability of health workers in urban and rural areas, selected countries, 2022 or latest available year
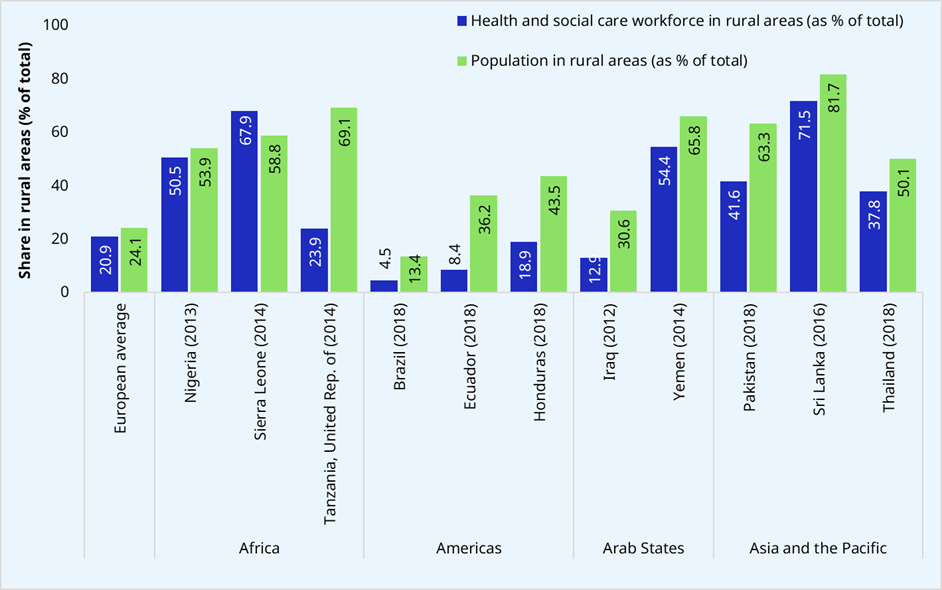
Source: ILO (2024g).
In cases where health services fall short, women’s and girls’ time spent caring for sick family members invariably increases. Even in cases where other barriers are overcome, the lack of care of adequate quality, including poor treatment and discrimination by health providers, can keep women from using health services for themselves or their dependants. Women with disabilities reportedly do not take up services for fear of abuse (UN 2019).
A large number of the jobs that are needed are in nursing and midwifery, with a projected shortfall of 5.7 million nurses by 2030 (McCarthy et al. 2020). Nurses and midwives play a central role in improving service coverage and have been key in RMNCH progress. Hiring, training and retaining them, including in rural areas, is a key building block in ensuring the availability, accessibility, acceptability and quality of care in line with ILO standards (ILO 2018b). They account for nearly half the global health workforce, and are predominantly women (WHO 2019a).
The lack of female health workers constitutes one of the access barriers that keep women away from health services. Survey data from a wide range of countries, including the Plurinational State of Bolivia, Ethiopia, Maldives, Peru, Sao Tome and Principe, and Timor-Leste, shows that half or more of the women reporting difficulties in accessing healthcare cite concerns about the availability of a female health provider (UN Women 2015b). Hence, investing in decent working conditions, in line with the ILO Medical Care Recommendation, 1944 (No. 69), and the Nursing Personnel Convention, 1977 (No. 149), and its Recommendation (No. 157), is urgent. The COVID-19 pandemic highlighted the essential role of these front-line care workers and the need to ensure decent work for them, including access to social protection and occupational safety and health (ILO 2020b) (see section 7).
At the same time, health services and the trained staff who deliver care need to become more responsive to the diverse needs of women across the life cycle and the constraints that they face in protecting their own health or in accessing and making use of available services. A case in point is the important role that healthcare staff can play in the detection of domestic violence. Yet without adequate training, screening protocols or referral mechanisms, health personnel are often unable to identify and adequately support survivors of domestic violence with the right psychosocial care. Similarly, staff should be trained to interact with people with disabilities and treat them respectfully. Equipping healthcare staff to address such situations requires the redesign of medical curricula and provision of on-the-job training. As the WHO makes explicit, “key concerns for women seeking health care include respect, trust, privacy and confidentiality – values that are often compromised in busy facilities, particularly among certain age groups and social groups” (2009, 75).
Research from countries across Africa, Asia and Latin America documents aggressive treatment of women, and disrespect shown by overworked and underpaid health staff, particularly in relation to maternity care and access to contraception, and most especially with regard to women from poorer and marginalized communities (Sen, Govender, and El-Gamal 2020; UN Women 2015b) or with disabilities (UN 2019). In Peru, for example, feminist lawyers and women’s rights organizations were able to uncover mass sterilization campaigns that systematically targeted indigenous women in poor, rural communities, as part of a broader family planning programme. Their efforts eventually led to an investigation by the national human rights commission that spurred the reform of the programme (Ewig 2006). Even in high-income countries, intersectionality manifests itself cruelly. For example in the United Kingdom, Black women are more likely to experience adverse outcomes during maternity care than their White counterparts, with maternal mortality being four times higher among Black women (Silverio et al. 2023).
Designing social health protection benefits in a responsive manner
Benefits package
ILO standards call for States to provide social protection to cover healthcare interventions needed to “maintain, restore or improve” health and people’s ability to work and to attend to their personal needs (Convention No. 102). Recommendation No. 69 further recalls that the range of services covered should be comprehensive and include preventive and curative interventions. According to Recommendation No. 202, among the guarantees that should be secured through national social protection floors, States should ensure access to a set of goods and services that constitute essential healthcare, including maternity care, and seek to provide higher levels of protection as soon as possible and to as many persons as possible, using the guidance provided by Convention No. 102 and more advanced standards, notably the Medical Care and Sickness Benefits Convention, 1969 (No. 130).
Convention No. 102 provides guidance on a minimum package of healthcare, which should include general practioners’ services, to provide basic primary healthcare (PHC) services. Moreover, it should cover reproductive, maternal, newborn and child health services, including antenatal care, childbirth, postnatal care and hospitalization if required, specialist and hospital care, and essential prescription pharmaceuticals, to be complemented by dental care and medical rehabilitation (including prosthetic and orthopaedic devices). The responsibility of national authorities is not only to regulate such entitlements but also to ensure that the services provided meet the criteria of availability, adaptability, acceptability and quality.
Against this backdrop, gaps remain in terms of SHP systems’ responsiveness to women’s specific needs. Countries have given different levels of priority to those needs in the design of social health protection benefits packages.
Primary healthcare. ILO standards stipulate that institutions responsible for SHP shall make a proactive effort to encourage protected populations to utilize population health interventions and, more generally, promotion and prevention services. This is in line with the vision promoted by the WHO on primary healthcare, identified as a central function of and a fundamental approach to service delivery. It is meant to be “the first level of contact of individuals, the family, and community with the national health system bringing health care as close as possible to where people live and work, and constitutes the first element of a continuing health care process” (WHO 1978). While this is true, in practice adopting such an approach often requires important shifts in health systems, and strong stewardship and regulatory capacity on the part of Ministries of Health. The PHC function remains incomplete in many countries (WHO 2019a).
PHC has the potential to foster greater accessibility of services for women and girls, because of its geographical proximity as well as its holistic and human-centred approach. As indicated earlier, women and girls may face barriers to their access related to geographical distance, cultural acceptability, and the financial cost of care or of accessing remote facilities, as well as constraints due to time poverty. The availability of adapted healthcare services in close proximity to one’s home can help overcome some of these contraints. Therefore, the range of services offered at primary level should include the health interventions that women need and that are of sufficient adaptability, acceptability and quality. In turn, SHP schemes should, in line with ILO standards, systematically include primary healthcare services within their benefits packages and support their role as the entry point to the health system. Similarly, specific health and social care services may be needed to tackle violence and harassment against women, as underlined by the Violence and Harassment Convention, 2019 (No. 190), for which primary care providers can play a referral role (ILO 2021e).
Reproductive, maternal, newborn and child health services. Since the promulgation of the MDGs, many countries have prioritized resource allocation to maternal healthcare and include maternal and child health in their SHP schemes. RMNCH services have often been prioritized in legal coverage, in line with ILO instruments which prioritize free maternal care. In the late 1990s, an assessment of publicly financed benefits packages in 152 countries found that delivery care and emergency obstetric care were often missing. With the focus of the MDGs on maternal healthcare, over the years this gap has been reduced. More recent analyses (Sen, Govender, and El-Gamal 2020) suggest that essential service packages often include maternal health and safe delivery. While RMNCH services are included in general primary care service packages in most countries, some have given greater priority to ensuring more comprehensive policies that guarantee coverage of mothers and children and include complicated births. The Philippines’ Safe Motherhood programme, for example, includes investments to strengthen the quality and scope of services as well as sustainable financing through PhilHealth. It covers all women about to give birth nationwide (ILO 2021e).
However, the range of services related to reproductive, maternal, newborn and child health can be defined in a more or less restrictive way and too often excludes some sexual and reproductive health services, as underlined below. Similarly, addressing men’s reproductive health needs can play a pivotal role in transforming stereotyped masculinity. Likewise, through recognizing the role of fathers in antenatal, childbirth, postnatal and child healthcare, a more equal sharing of childcare between parents can be encouraged. This can also foster non-violence at home, at work and in society more broadly (ILO 2021e).
Sexual and reproductive health and rights (SRHR). Whether or not the specific health needs of women and girls are adequately addressed is particularly important when defining SHP benefits packages, and more broadly when planning service delivery at different levels of care in the healthcare system. Recent analyses suggest that while benefits packages often include maternal health and safe delivery, they exclude the broader and equally essential range of services that women need (access to contraception, safe abortion, cervical cancer screening and treatment, adolescent healthcare and so on) (Sen, Govender, and El-Gamal 2020). Access to sexual and reproductive health and rights is a precondition for young women to exercise real choice in family planning, be able to pursue their education or training and engage in employment. This means including reproductive health services in social health protection service packages without co-payments, and minimizing the additional costs of seeking care, for example by making services easily available in remote areas and ensuring they are accessible for all women. Evidence suggests that women with disabilities face significant barriers to accessing SRHR due to misperceptions, stigma and discrimination (UN 2018).
Unsafe abortion is the fourth leading cause of maternal mortality globally and occurs mostly in low and middle-income countries (Sen, Govender, and El-Gamal 2020). Yet safe abortion is rarely included in benefits packages, even where it is legal (UN Women 2015b), and sometimes even explicitly excluded from the scope of SHP in the legal framework, as in Myanmar (ILO 2021e). Significant retrogression in access to family planning and safe abortion has occurred in recent years, with the notable prohibition of abortion being reintroduced in Poland and the United States (Amnesty International 2022b; 2022a), marking a setback for women in these countries.
Mental health. At the global level, the burden of mental disorders weighs more heavily on women than on men (GBD 2019 Mental Disorders Collaborators 2022). There are multiple socio-economic factors that contribute to this situation, as well as gender-based violence and discrimination (J. Allen et al. 2014). Different types of mental disorders affect women and men, with women particularly at risk of anxiety, depression (including post-partum), and bipolar and eating disorders (GBD 2019 Mental Disorders Collaborators 2022). The mental health and well-being of women affect their own physical health as well as the health of their children, with lasting effects (WHO 2022a).
Despite the significance of mental health disorders, often mental health services are unavailable at primary care level, or not available at all in health systems in developing countries (Patel et al. 2018). Even when they are, they are seldom included in SHP benefits packages in those settings, and may be accessed under a more restrictive set of rules (ILO 2021e). This stands in the way of improving SHP benefit responsiveness to women’s needs.
Geriatric and long-term care services (see subsection 5.2).
Rehabilitation and attention to specific needs. To achieve the objective of UHC, services need to cater also for people with specific needs. For example, persons with disabilities tend to use more health services, on average, compared to the rest of the population. In addition to requiring the same range of general health services (including immunization, screening, and sexual and reproductive health), they need additional services that are particular to their disability (such as specific medicine, assistive devices and rehabilitation). Moreover, the indirect costs of accessing care tend to be higher for those with certain types of disabilities. However, persons with disabilities overall report a poorer health status, experience greater barriers to receiving care and are more likely to face catastrophic health expenditures than persons without disabilities, since often there is little consideration for including people with disabilities and making services accessible, affordable and acceptable to them.
Network of service providers
The definition of the network of service providers and modalities to access services is part of the design features of SHP systems. The way they are designed, often in the legislation, conditions effective access to healthcare services. Ensuring the adequacy of the geographical coverage offered by healthcare providers is key to securing effective access near the home and helping to overcome the barriers to access that tend to affect women and girls disproportionately. Similarly, the way providers are paid needs to strategically align with the objective of effective protection and access to high-quality services. Attention must also be paid to avoiding any financial incentive for providers to induce unecessarily invasive procedures (Frota et al. 2020). For example, SHP schemes need to align with health sector efforts to reduce caesarian section rates in countries where they are higher than recommended (Gibbons et al. 2012; Ruth Walker, Turnbull, and Wilkinson 2002).
The services included in the benefits package need to be delivered in sufficient volume and quality. SHP policies need to foster a culture of delivery of high-quality care but also of adequate treatment of patients, regardless of their gender, disability status, or cultural, social, economic and ethnic background. The network of service providers in charge of delivering SHP benefits needs to be satisfactory in this respect. This is where close collaboration across the various pillars of health systems is needed when devising social health protection policies. If the supply side is not reinforced, with a trained workforce that enjoys decent working conditions (see section 7), adequate health products, medicine and equipment, and strong stewardship from the Ministry of Health, social health protection policies risk becoming an empty promise, with the greatest adverse impact falling on the most vulnerable, including women.
6.2.2. Securing financial protection for women and girls when accessing healthcare services
Financial protection: Where are we, and why is it important for women?
Effective and comprehensive monitoring of financial protection, allowing for direct comparisons between legal entitlements and effective financial protection24 within and across countries, is not available. Rather, most countries produce and analyse data on out-of-pocket (OOP) expenditure on health based on national surveys conducted periodically (WHO 2022b). On this basis, it is possible to know the proportion of OOP expenditures within the overall expenses on health of a country, and the share of households pushed into poverty because of such payments. The latter has been included within the SDG framework under indicator 3.8.2.
It is concerning that across the regions of the world, OOP expenditures have come to affect larger shares of the population. The proportion of the global population whose OOP health spending exceeds 10 per cent of their household budget grew from 9.4 per cent in 2000 to 13.2 per cent in 2017 (WHO 2022b). OOP expenditures remain and financial protection is insufficient, with greatest impact on the poor. Rural households in particular are more likely to incur greater OOP costs than urban households due to supply-side constraints within the rural health system (Knaul et al. 2011). The poorer the country, the higher the proportion of total health expenditure that is financed in this regressive way (WHO, forthcoming). Policy attention to UHC needs to be harnessed to address the barriers (including gender-specific barriers) that women face in accessing services (Sen, Govender, and El-Gamal 2020).
It is worth noting that these indicators are not measures of financial protection, but rather of the lack thereof. Furthermore, low catastrophic health spending could simply be due to insufficient service coverage or non-take-up, rather than improved financial protection. Indicators of financial hardship must therefore be viewed alongside the actual use of services, forgone care/unmet needs analysis, and service coverage indicators to identify whether a low incidence of catastrophic or impoverishing OOP payments reflects poor access to services rather than high levels of financial protection (see box 6.1). High OOP spending could also reflect high consumption of elective health intervention by wealthier categories of the population. Therefore, OOP expenditure must be analysed carefully to understand its source and to be able to devise adequate SHP and health system responses accordingly (ILO 2021j).
Box 6.1. Why do people forgo healthcare? Evidence from Europe
A recent study in the WHO European region estimated the prevalence and drivers of forgone care through a systematic literature review and meta-analysis (Rahman et al. 2022). It finds that among people aged 65 and over, 10.4 per cent reported forgoing healthcare, compared to 4.9 per cent among adults aged 31 to 64, and 11.5 per cent among those aged up to 30. The leading reason for forgone healthcare among older persons was affordability (31.7 per cent), followed by problems with acceptability (10.4 per cent), accessibility (6.2 per cent) and availability (4.9 per cent) of services. The study found significant variation in the pooled prevalence of forgone healthcare due to cost, by gender (male 10.9 per cent versus female 14.4 per cent) among other factors (e.g. education level, self-reported health status, insurance status and economic status).
From a gender perspective, OOP expenses pose specific challenges. For a start, the fact that existing data on them relies on household-level surveys poses a methodological constraint, given the lack of sex-disaggregated data within such surveys, whereas resources may not be shared equally within households. These constraints notwithstanding, a number of studies have found women’s OOP expenses to be systematically higher than men’s in a number of countries, including Brazil, the Dominican Republic, Ecuador, Paraguay and Peru, not only due to gender-specific health needs but also because of the greater prevalence of chronic illnesses and some mental health conditions among women (WHO 2009; WHO and PAHO 2021). It is also worth noting that when medical treatment requires co-payments, women’s access to healthcare often hinges on the readiness of male partners or fathers to provide the necessary cash (UN Women 2015b). Similarly, across a range of countries, data from household surveys shows that a significant proportion of women do not decide independently on their own healthcare – a little under half of women in Pakistan and more than two thirds of women in Senegal, for example, needed to obtain consent from family members to obtain medical care (UN Women 2015b). Power inequalities within and beyond households therefore often determine women’s and men’s differential access to health and claims on related resources at multiple levels (household, community, State).
While there is no systematic and comparable collection of data on OOP expenditure, disaggregated by gender and other stratifiers, women with disabilities face particular challenges. With a higher risk of poverty overall and greater need for healthcare, the risk of impoverishment due to OOP expenses is particularly acute for them. Some countries try to remedy this by subsidizing healthcare premiums, modifying benefits packages or waiving co-payments for people with disabilities (among them Ghana, the Maldives, the Philippines and Viet Nam).
The importance of OOP expenses in total health expenditure, especially in low- and middle-income countries, calls for greater and better allocation of public resources for the health sector, and strong SHP systems to protect people from hardship. Two points are of particular interest in terms of enhancing the gender-responsiveness of SHP and its outcomes:
-
SHP systems based on broad risk-pooling are needed to ensure the redistributive effect of such policies between women and men and ensure that women’s health needs are supported by society as a whole.
-
Much of the progress made in access to RMNCH especially in lower-income countries, has been possible thanks to the prioritization of vertical programmes and/or the use of external resources. Looking to the future, sustainable sources of domestic financing need to be made available to sustain these gains over time.
Designing social health protection to secure financial protection: Co-payments and user fees
Since the goal of SHP systems is to ensure that no one suffers financial hardship when seeking the care they need, social security standards place a strong emphasis on limiting co-payments to a minimum. Indeed, co-payments are only authorized in the case of services for which there is a need to preclude abuse on the part of users, and their level should therefore be set so as not to cause hardship (ILO 2020f). However, the provisions of national legislations and systems varies widely, impacting health services that are particularly important to women and girls.
In addition, ILO standards stipulate that maternity care should not be subject to co-payments. This is rooted in three important findings from international practice (Frota et al. 2020):
-
Timely maternity care, accessed at early stages and without delay, is an efficient and highly impactful investment in terms of health outcomes. Prenatal visits and surveillance have yielded significant results in reducing complications and associated costs (WHO 2009). Post-partum care ensures prompt recovery and early identification and management of problems and contributes to health promotion, including infant immunization and advice on breastfeeding (Lawn et al. 2016). These, in return, facilitate the full recovery of women’s capacity to work, alongside maternity benefits during maternity leave (ILO 2015).
-
The benefit–cost ratio of investment in maternal health protection is high, for the health system and beyond. The probability of using these services is generally limited to a small number of events during a woman’s lifetime, for a limited period, which limits the cost of maternal health packages per individual. Furthermore, maternal and child health interventions are shown to be particularly cost-effective (Memirie et al. 2019).
-
Ensuring the highest level of financial protection is crucial to improve effective access to maternity care for all. This is all the more important in view of the fact that women may face greater challenges than men when having to make payments up front to health facilities. Women’s greater difficulties in making such payments are in some contexts due to the fact that they may not have the power in decision-making regarding the control and allocation of household resources.
While ILO standards give high priority to financial protection for maternity care, the level of financial protection has not been prioritized equally across countries. Maternity care, in particular around delivery, remains costly in many places (see box 6.2 for examples from Asia).
Box 6.2. Different strategies to secure free maternity care in Asia
Some countries exempt maternal or child healthcare services from co-payments, including the Lao People’s Democratic Republic, Malaysia, the Republic of Korea, and Viet Nam. In Malaysia, the majority of maternal health services are exempted from user fees that apply to use of other services provided by the public healthcare system. Successful RMNCH outcomes there are attributed in part to this policy. A similar strategy has been adopted in Brunei Darussalam, with comparable success.
Likewise, in the Philippines, the Safe Motherhood initiative has been successful in ensuring the availability of services and securing PhilHealth coverage for RMNCH care. Under this programme, all women about to give birth are automatically enrolled in PhilHealth through point-of-care enrolment at the health facility. Some are eligible for government subsidies for their contributions (persons defined as indigent), but others are expected to pay contributions equal to those of informal-economy workers (if not already covered). The value of benefits exceeds the contribution amount, which facilitates enrolment and compliance with contribution payments.25
Some countries have put in place co-payment exemptions for specific groups. Often policies to exempt or further reduce co-payment amounts for RMNCH care are embedded within broader exemption policies. For example, the Lao People’s Democratic Republic’s National Health Insurance (NHI) scheme exempts village heads, pregnant women, children under 5 and Buddhist monks from co-payments.
Source: ILO (2021e).
Therefore, co-payments for essential healthcare services should be restricted to a minimum when they are necessary to preclude abuse, since they constitute a barrier to access that disproportionately impacts on vulnerable populations, especially women and girls (ILO 2020f). For this protection to be effective, a designated network of healthcare providers needs to be available, adaptable, acceptable and of adequate quality, and illicit co-payments need to be sanctioned.
6.3 Coordination with social protection cash benefits and care policies
SHP benefits need to be considered together with cash benefits directed at replacing or supporting income if they are intended to meet their goal of improving well-being. Sickness, maternity and disability are all physiological conditions that require access not only to healthcare services without hardship but also to an income, as they often cause (partial or full, temporary or permanent) incapacity to work and therefore gain earnings.
CCTs, where the receipt of cash is, as we saw in sections 3 and 4, directly linked to the beneficiary meeting conditions that involve healthcare service utilization, have been the focus of policy and research. As already noted, if the supply side is not ready and/or is not compensated for the additional workload, the quality of the services can be poor, the queues can be longer, and social assistance recipients can feel stigmatized at the point of service. Even if the supply side is ready, when the burden of those conditionalities falls on women it can create an additional mental load. Careful design of such conditionalities is therefore important, together with consideration of other ways of integrating policies that do not put an undue burden on the beneficiaries themselves.
To truly contribute to gender-transformative policies, SHP systems need to be well coordinated with childcare and long-term care services. Indeed, as seen throughout this section, women experience a set of unique social, economic and cultural conditions that impact on their health and their ability to access the health and other services they and their dependants need.
6.4 Recommendations for enhancing the gender-responsiveness of social health protection
Policymakers and SHP institutions can do much more to ensure that women enjoy access to high-quality healthcare without financial hardship. In so doing they should strive to pursue some of the following recommendations that can enhance the gender-responsiveness of SHP policies and schemes.
-
Considering gender as a core dimension in the design and implementation of SHP systems, based on a thorough gender analysis. Making SHP gender-transformative requires explicit intent and effort to identify specific health needs, barriers, and other social determinants of health inequities that affect women and girls, and to purposefully address these in the design and implementation of SHP schemes. Careful design of SHP benefits packages, copayment policies and the contracting of service providers must respond to those specific needs and help overcome the barriers to access that women face, with attention to the specific vulnerabilities or support needs of women with disabilities, women from refugee or migrant communities, women living in rural areas, ethnic minority women, and so on.
-
Closing social health protection coverage gaps. While many countries have committed themselves in their legal frameworks to extending social health protection to all without gender-based discrimination, in practice many coverage gaps remain, especially in low- and middle-income countries. Gaps in effective coverage disproportionately affect people who are in informal and vulnerable employment or without employment, categories in which women tend to be disproportionately represented in these countries. Adequate design and sustainable financing of these schemes to expand their coverage are urgently needed.
-
Removing financial barriers to accessing a comprehensive range of healthcare services. While this is critical for both women and men, social health protection is particularly important for women, as they are less likely to have an income of their own or control what income they do earn, and more likely to face costly health conditions related to pregnancy, childbirth and other sexual and reproductive health needs, and to be considered primarily responsible for the health of their children.
-
Ensuring the integration of the full range of women and adolescent girls’ health needs, encompassing also sexual and reproductive rights and services, in SHP benefits packages, including for women with disabilities. Benefits packages should incorporate not only maternal health and safe delivery but also the broader and equally essential range of services that women need, including access to contraception, safe abortion, cervical cancer screening and treatment, adolescent healthcare, mental health services and so on. Similarly, women’s longer life expectancy results in an array of health issues arising in the later years of life, often the result of a lifetime of accumulated deprivations and insufficient healthcare access, which require adequate health interventions. This needs to go in tandem with corollary investment in the health sector.
-
Securing a network of service providers able to effectively deliver such services near women’s homes. Investment is needed in primary healthcare, to secure the supply of services that meet the criteria of availability, acceptability, adaptability and quality. The PHC approach is more needed than ever to address the health needs of women and girls and overcome geographical and financial barriers to access. The issues of adequate distribution of services and retention of a skilled health workforce together pose serious challenges. This requires investment in basic infrastructure and staff training, to ensure the removal of social and geographical barriers and the delivery of non-stigmatizing and woman-centred health services. Beyond maternal health services, the lack of female health workers constitutes one of the access barriers that in many settings keep women away from health services.
-
Sustaining the gains of the MDGs on maternal and child health outcomes with adequate domestic financing and political commitment. Too many free care programmes covering pregnant women and young children remain financed vertically and/or from external sources, especially in low-income countries. In an economic context of stagnation, recession and recurrent crisis, external sources of funding may not be sustainable over the long run, and risk jeopardizing the progress made thus far.
-
Adopting an integrated approach across healthcare, social care and cash benefits. In particular, more effort is needed to ensure access to free, high-quality healthcare in line with international social security standards, to expand social protection coverage, and to improve coordination between healthcare, social care and income security schemes. Indeed, access to both healthcare and income security is essential to ensure women’s rights, including both their right to work and their rights at work.
Social protection and the care economy
In line with the ILO report Decent work and the care economy (ILO 2024b), this paper has made many references to the role of social protection in ensuring decent working conditions for the care workforce and the need to adjust and reform social protection provision to ensure the continuous and adequate coverage of all unpaid caregivers. We have also touched on the role of social protection systems in some countries, or social spending in many others, in financing the provision of services (especially childcare and long-term care) to meet the needs of care recipients (be they children, working-age adults, or older persons) and the parametric adjustments to different social protection branches that can be made to ensure (paid) care workers and (unpaid) caregivers can enjoy the full range of social protection.
While there are important interconnections and complementarities between social protection policies and the care economy, the two are not coterminous. As the 2018 ILO report on the care economy recognized:
The high road to care work needs to be grounded in transformative measures in five main policy areas: care, macroeconomics, social protection, labour and migration. These policies are transformative when they contribute to the recognition of the value of unpaid care work, the reduction of the drudgery of certain forms of care work and the redistribution of care responsibilities between women and men and between households and the State. The policies need also to reward care workers adequately and promote their representation, as well as that of care recipients and unpaid carers (Addati et al. 2018, xiii).
In this section, we provide a more synthetic perspective on some of the ways in which social protection policies can recognize and value care work, both paid and unpaid, and redistribute care responsibilities between women and men, and between households and other institutions that finance and deliver care services with the overall oversight of the State.
As discussed in subsection 1.3, the activities and relationships involved in meeting the physical and emotional needs of children and adults are often structured by family and kinship relations on an unpaid basis. This is one central component of the care economy. More than three quarters of unpaid care work in the world is performed by women (ILO 2024b), even as they are increasing the time they allocate to paid work.
However, in addition to the role of families, many of the intimate tasks associated with care are also organized through non-familial institutions – the public sector, private for-profit and third-sector organizations – which, combined, constitute “regimes of care” or the “care diamond” (Jenson and Saint-Martin 2003; Razavi 2007). Over the past decades, changes in economic, social and demographic structures have spurred the growth of the care economy in many countries. Women’s entry into the labour force has squeezed the time available for unpaid care and prompted a rise in the demand for paid care services. As a result, care workers now constitute a large and growing segment of the labour force: an estimated 381 million jobs globally, or about 11.5 per cent of total employment (ILO 2024b), with significant regional variation.
7.1 Decent work deficits in the paid care sector: Recognizing, valuing and protecting care workers
Different forms of paid care now account for a large number of jobs globally. For instance, according to 2018 data, health and social work accounted for around 130 million jobs worldwide, including nurses, midwives, personal care workers, community care workers, and volunteer health workers. Education sector jobs, including early childhood education and care, constituted around 157 million jobs, and domestic work around 70 million workers worldwide (Addati et al. 2018). This raises questions about the quality of employment – i.e. conditions of work of the care workforce, including their access to social protection – and its impact on the attractiveness of (and their retention in) those jobs. The conditions of employment, including access to social protection, have implications for the quality and continuity of service that is offered to care recipients.
Historically, care occupations such as domestic service, and later the nursing and teaching professions, have often been the first entry points for women into the labour force, since they were regarded as socially appropriate professions. Today, most paid care services are still provided by a feminized workforce. This has elicited the obvious observation that shifting care work out of the family and into the public domain has not changed the fact that it is still seen as “women’s work”. A more complex question is whether such a shift can address care’s undervaluation: do care workers receive adequate wages, comparable to those that workers in non-care occupations with similar levels of education, experience and skill receive? Do they enjoy similar levels of social protection? And do they have the right to organize and engage in collective bargaining to improve their lot?
A study of 12 industrial and developing countries finds that paid care work often entails a “wage penalty”, meaning that care workers are not adequately compensated for their skills and experience in comparison to other workers (Budig and Misra 2010). In common with other “public goods”, caregiving tends to be undervalued and underpaid by the market. To take the case of domestic workers, on whose labour many households depend, to cook, clean, and take care of children or older family members, fewer than two of every ten are effectively covered by social protection (ILO 2022e). This is in addition to other decent work deficits that domestic workers face, including in the areas of wages and working time, as well as freedom from abuse and harassment. When compared to other employees, domestic workers are nearly two times less likely to be registered under social insurance schemes, which goes against the principle set out in the Domestic Workers Convention, 2011 (No. 189), of ensuring conditions that are not less favourable than those applicable to workers generally (ILO 2022e). The obstacles standing in the way of domestic workers are legion, including legal exclusion, administrative barriers and lack of information, as well as low contributory capacities, lack of enforcement of – and low compliance with – labour and social security laws, and limited unionization and voice (ILO 2022d; 2022e).
But these barriers are not insurmountable. Legislative reforms can undo the legal exclusion of domestic workers that is enshrined in labour and social security laws alike, including by recognizing the existence of an employment relationship and removing exclusionary thresholds, such as those related to working time, earnings or multiple employment relationships, to address the specificities of employment arrangements. This also means that inclusive approaches that extend existing schemes to include domestic workers should be favoured over solutions that isolate domestic workers under special schemes, which lack wider risk-pooling (ILO 2021h; 2021f). Legal reforms are an essential step that needs to be accompanied by adapted administrative procedures, for example simplified digital solutions for registration and contribution payments that address the limited contributory and administrative capacities of domestic workers and their employers, who are usually private households, and improved governance mechanisms to ensure effective access (ILO 2021h; 2021f). Governments will also need to adapt the financing modalities to ensure that despite low contributory capacities, collective financing and broad risk-pooling with subsidies from general government revenue can ensure that all domestic workers are able to access social protection when they need it. Bilateral social security agreements are also very important, given the large number of domestic workers who work outside their countries of origin, to facilitate the portability of social protection entitlements (ILO 2021i).
Aside from domestic workers, other care workers, in particular those in the health and social work sector, also face serious decent work deficits. During the COVID-19 pandemic, across the world, the public applauded health workers in recognition of their contribution to the health and well-being of societies. However, despite the applause, in most countries there is rampant underinvestment in primary healthcare, as well as a significant gap in levels of investment between low- and high-income countries. This underinvestment is associated with decent work deficits affecting the workforce (ILO 2023e).
Health professionals, such as doctors (and, to a lesser extent, nurses), who tend to enjoy somewhat better working conditions, are an important segment of the care workforce but do not represent the full spectrum of workers in the sector, located lower in the health workforce hierarchy (ILO 2022f). The latter includes personal care workers such as healthcare assistants, home-based health workers and long-term care workers, in addition to childcare workers and teaching assistants. Personal care workers constitute a smaller proportion of health workers in low-income countries (less than 8 per cent), a proportion which rises to 32.3 per cent in high-income economies, reflecting the growing demand for care work in these countries, particularly in the context of population ageing and the need for long-term care services (ILO 2023e, fig. 4.6). In addition to challenges with regard to occupational safety and health, such as the physical and mental exhaustion and physical and verbal abuse to which many personal care workers are subject, a growing concern is the increasing use of alternative contractual arrangements, temporary contracts or agency work, which deny these workers the usual array of protection that comes with decent employment. Especially for those at the most informal end of the labour market, exclusion from regulations on minimum wages, maximum working hours or mandatory employer/employee social insurance contributions leaves many workers in the care sector very vulnerable.
In fact, in the context of economic crisis and fiscal austerity, health workers in some countries have been laid off, while insufficient investment in the health sector has meant that some hitherto well-paid and protected care workers (nurses, for example) have seen their wages stagnate and face highly adverse working conditions under a deteriorating health sector infrastructure (Kentikelenis and Stubbs 2023). In some contexts, public social services have come to rely heavily on “voluntary” or “community” work – very often shorthand for unpaid, underpaid or unprotected work – patching up shortages of health personnel. Front-line care workers in public social programmes are thus kept at arm’s length by the State and denied the usual array of protections that should come with public sector employment.
A case in point is the Anganwadi (childcare centre) workers and helpers who staff the Integrated Child Development Scheme in India – probably the largest early childhood nutrition scheme globally – and the Accredited Social Health Activists (ASHAs), female community healthcare workers appointed and trained by the National Rural Health Mission of India. While employed by the State, these workers are not classified as workers but as “volunteers”, who receive stipends (or “incentives” in the case of ASHAs) instead of wages, and lack the leave entitlements and social security benefits available to permanent, full-time public employees. Likewise, in Nepal, female community health volunteers, who number around 50,000 and work under the direction of the Ministry of Health and Population, are not paid the minimum wage, and only receive about US$250 a year (compared to public sector nurses who receive about US$250 a month) plus insufficient allowances for transport. They have excessive workloads but, as they are not recognized as workers, they do not receive social protection benefits or protection of their work hours (ILO 2022f).
Furthermore, as already noted, several studies (including Addati et al. 2018; Budig and Misra 2010; England et al. 2002) show that care workers, even when considered wage workers, face significant wage disadvantages vis-à-vis workers with comparable skill levels in non-care-related occupations (widely referred to as the “care penalty”). Building on previous research on care penalties, Folbre et al. (2021) show that in the United States during the COVID19 pandemic, essential workers in care services (health, education and social services) were paid less than other essential workers with comparable personal and work characteristics (in law enforcement, support and waste services, transportation, agriculture, retail and finance), a pattern with especially costly consequences for women. Low-wage workers such as healthcare assistants are especially vulnerable.
An important finding from the pandemic is that the unionization of workers has been protective of lives (ILO 2023e). This finding emerges when one compares the excess mortality from COVID-19 of healthcare workers (despite their daily exposure to the virus) against the excess mortality of other key workers who were not unionized, the difference being attributed to the fact that the former are more likely to have health insurance and access to sickness benefits. The slow and inadequate policy response to the needs of the long-term care sector and its workforce in some countries, especially when compared to the health sector and healthcare professionals, whether in terms of monitoring and testing, staffing and working conditions, or funding, speaks to the relative neglect of the long-term care sector and its workforce, and “the deeper undervaluing of… the activity of caring and those who require care” (Daly 2020).
On a positive note, efforts at organizing certain categories of care workers, including community health workers, are translating into some tangible outcomes. In Pakistan, for example, the “lady health workers” (LHWs), who did not enjoy any working-time protection or social security coverage, were regularized in 2012 following collective action by a number of trade unions in the Sindh province. They now receive the minimum wage, though often with delayed payment. They also still face difficulties in obtaining medical leave and allowances, and retired LHWs have not yet begun to receive their pensions (ILO 2022f).
7.2 Recognizing, reducing and redistributing unpaid care work: Income transfers, paid leave and care services
Apart from addressing the decent work deficits of care workers, highlighted in the previous section, which have implications for both them and the recipients of care, social protection systems also respond directly to the needs of care recipients and unpaid caregivers in at least two other ways.
First, income security provided across the life cycle – through child and family benefits, disability benefits, sickness benefits and pensions, to name but a few – has an important role to play in ensuring the well-being of care recipients. This is often complemented by the provision of social services and other in-kind benefits. The provision of both cash benefits and services also has important implications for unpaid family caregivers.
Child benefits, for example, as we have seen, play a critical role in improving children’s development and well-being, helping them attain their full potential and supporting family livelihoods and care needs. Social protection cash benefits and effective access to care services are often mutually reinforcing, particularly with regard to healthcare, nutrition, childcare or education services, and productive inputs. Depending on their design and delivery, healthcare and childcare services can be critical in maximizing and sustaining the impacts of cash benefits, overcoming gender inequalities, and fostering social inclusion of children from marginalized families (see subsection 3.1). In theory, childcare services could pursue both child development goals – such as getting children ready for school – and work–family reconciliation goals, by offering alternatives to parental care. In practice, comprehensive Early Childhood Education and Care (ECEC) services attuned to the needs of working families remain scarce, particularly for younger children, and especially in developing countries. However, investment in childcare services can deliver significant economic and social dividends for families, individuals and societies by enhancing children’s capabilities, facilitating women’s labour market choices, and creating decent jobs in the care sector (ILO 2023b; UN Women 2015a).
Likewise, having income security in old age through a pension should be complemented by access to appropriate healthcare and long-term care services without financial hardship, as we have seen (see subsection 5.2 and section 6). With an increasing global burden of non-communicable diseases, not only should prevention be prioritized from an early age and determinants of chronic and long-term diseases addressed, but health services also need to be better coordinated with social care services that respond to the needs of older people (WHO 2015).
While every effort should be made to prevent, as much as possible, the need for LTC through the promotion of healthy and active ageing for instance, it is clear that with the absolute number of older people and longevity increasing, that need is growing, with important implications for unpaid family caregivers. This is a multifaceted issue which goes well beyond the sole scope of social protection policies. While modalities for the financing and delivery of LTC services vary greatly across countries, coherence between healthcare, social care and social protection systems is needed to ensure quality, especially in care models that are pluralistic in nature. In practice, this continuum is not always realized, and coordination is weak (see Tessier, De Wulf, and Momose 2022a). In the absence of effective coordination, models of long-term care that rely exclusively or predominantly on families are likely to be both inequitable and unsustainable. Generations of the same family are more likely to be living apart, and adult children may not always be able to care for their frail, older parents even if they want to. Moreover, rapid fertility decline in many countries means that there are fewer or no adult children to care for older parents. At the same time, women’s increasing attachment to the labour force and the concomitant reliance of families on their earnings make it difficult for them to provide full-time care for ageing spouses or parents while also holding on to their jobs. Hence, affordable and quality LTC services provide an alternative to unpaid care provided by family members, predominantly women, who form the invisible backbone of LTC systems. The key point here is that social protection systems need to assume greater responsibility so that those who need LTC can access it without hardship.
Second, social protection systems can also support persons with family responsibilities directly, through parental leave benefits and care credits, as we have seen across different sections of this paper. Having the time to care for loved ones through parental leave policies can help women and men with care responsibilities and enable women to enter and remain in the labour market when their children are young. Parental leave can be taken by parents of any gender to care for small children in the period after maternity and paternity leave expires. By reducing the economic penalties for taking time off work to provide care, paid leave policies can also be used to foster gender equality in caregiving by incentivizing men to take more parental leave. However, to truly cover the costs of child raising, all the family-friendly policies outlined in figure 3.2 ought to be in place. In most developing countries, however, where even maternity leave is often not widely available, except to employees in the formal sector (or where leave is available but not necessarily paid), the priority is to achieve universal coverage of maternity benefits, through an appropriate combination of contributory and non-contributory mechanisms. This would be the first step – chronologically speaking – in building a full, family-friendly policy portfolio.
Conclusion: A social protection agenda that works for women and for gender equality
What are some of the key requirements for building a gender-responsive social protection system?
This paper has provided an overview of the key elements that social protection policies need to include to be able to address the gender-specific risks and structural constraints that women face across the life cycle. For a start, it should be underlined that all life-cycle benefits are relevant to gender equality, and not just those relating to maternity or parenthood. However, a recent analysis of national social protection strategies in 30 African countries finds that the recognition of gender-specific risks is heavily tilted towards maternal health (28 of 30 strategies recognize maternity-related health risks), while other life-cycle risks, such as widowhood and poverty in old age, were far less frequently cited (respectively 15 and one out of 30 strategies) (UN Women 2021b). Furthermore, all life-cycle benefits can be enhanced to be more gender-responsive by taking into account the structural specificities of women’s labour market trajectories, as well as gender power dynamics within and beyond households. Evidence shows that when well-designed, social protection measures can narrow gender-based income gaps, enhance women’s access to an income of their own and be a lifeline, especially for single mothers.
This paper has identified the key design considerations that can ensure responsiveness to gender-specific risks across the life cycle discussed in some detail in preceding sections. For example, family and child benefits can redress the disadvantages faced by girls with regard to secondary school attendance, by providing higher benefit levels for them than for boys at the onset of secondary school, which is when the risk of girls dropping out of school is highest. Remaining in school longer can also help reduce the incidence of early marriage for girls. When it comes to OSH policy and employment injury benefits, policies need to respond better to the occupational risks that women workers are more likely to face, such as the mental health issues that are rife among health, education and care sector staff, violence and harassment, and the general wear and tear associated with repetitive movements on electronic assembly lines, for example. Social protection systems should also provide income security through cash transfers for survivors of domestic violence, coordinated with violence-against-women services, to give them the time they need to seek support (administrative, medical, psychological) and recover from the trauma. To guard against inadequate pension income during old age, allocating pension care credits and establishing minimum benefit levels can partly offset the effects of the gender pay gap and the motherhood penalty incurred by women as a result of care-related disruptions in their labour market trajectories.
We are not alone in calling for a systems and life-cycle approach. There is growing recognition among a wide range of development actors “that no single social protection programme can guarantee that women are protected through various shocks that may occur throughout their lives”. These calls, as Cookson et al. (2023) note, represent a pivot from the earlier emphasis on singular social protection instruments targeting women, towards a much broader systemic focus.
The present paper has also underlined the important interconnections between gender and other forms of social exclusion and vulnerabilities, such as disability status, the related inequalities in labour markets and women’s access to social protection, and the level of benefits they can expect to receive. This is particularly relevant for social insurance schemes, where entitlements often depend on past working and earnings trajectories and contributions. In this context, specific design features to extend social insurance coverage to hitherto unprotected groups of workers, and in particular to women, are critical for providing access to adequate levels of social protection for women and recognizing their contributions to society through both paid and unpaid work. In fact, social protection systems that are designed to compensate for interrupted periods of paid work and low earnings benefit not only women and carers but also other categories of workers, and can benefit employers with a healthier, more productive workforce, with dividends for the whole of society. Where social insurance schemes cover only a small share of the population, as is the case in many low- and middle-income countries, non-contributory social protection schemes have an important role to play in ensuring that women enjoy at least a basic level of social protection.
However, there is also evidence of a shift taking place in some countries, from social insurance to individual capital accounts. As elaborated in section 4, this will likely have an adverse effect on women’s income security, most notably by making benefits more directly based on lifetime contributions, through benefit formulas that often consider the number of years during which the person is expected to receive benefits (discriminating against women who have a higher life expectancy), thus penalizing women for earlier retirement while not having other redistributive design features such as guaranteeing minimum benefit levels.
The paper has also underscored the complementarities and synergies between social protection policies and investments in accessible, affordable and good-quality social services – including health services as well as childcare and long-term care services. Evidence shows that the effect of social services on poverty and inequality is significant, and the complementarities between transfers and services are particularly important for women. Because of their reproductive and other gender-specific health needs, and their lower earnings, access to health services without financial hardship is even more important for women than men. Women also tend to perform the bulk of unpaid care work, caring for sick family members and accompanying them on medical visits, but are less likely than men to receive care from a spouse when they are old and frail. Hence, finding alternatives to family care that are affordable, accessible and of good quality is an urgent policy issue, as is the challenge of finding sources of financing that are both equitable and sustainable. The fact that care services – be they healthcare, childcare or long-term care – are delivered by a predominantly female workforce, often characterized by decent work deficits, draws attention to their working conditions, including access to social protection, and the need for adequate recognition and valuation of the work, along with the potential for creating decent employment as a dynamic sector that is understaffed in many countries.
Given the significant potential that social protection policies hold in reducing gender inequality, women’s participation in the design, implementation and monitoring of these policies is crucial. Removing the barriers to women’s right to social protection requires legal and policy reforms, decisive action by States, attitudinal and normative change, and progressive action by employers’ and workers’ organizations (UN Women 2023b). The role of social movements and civil society organizations (CSOs) in changing attitudes in everyday life and ensuring that policy action does not lag behind normative shifts is also pivotal. Yet the role of political context and political actors in enabling or constraining the gender-responsiveness of social protection policies and system-building has not been the subject of extensive studies, with a few exceptions (Cookson et al. 2023).
To ensure women’s participation in social protection policymaking, it is key for them to play a strong role in an inclusive social dialogue. The participation of social partners and consultation with women’s rights organizations in the process of putting a social protection strategy together are key, as is the inclusion of gender-specific indicators in the monitoring and evaluation framework, and adequate grievance and redress mechanisms. However, as a recent review of social protection strategies concluded, “The limited recognition of structural gender inequalities and the gap between recognition and action to address them, suggest a need for greater monitoring, participation and accountability at all stages of the policy cycle” (UN Women 2021b).
As this paper has suggested throughout, it is critical to have timely and robust gender data and analysis not only to inform the design and implementation of social protection strategies, policies and schemes but also to monitor and evaluate their performance and outcomes. Effective policymaking requires effective monitoring. This means closing data and knowledge gaps in the provision of social protection. Policymakers can only ensure effective coverage for girls and women if they have access to high-quality data that is disaggregated by sex, age, disability and migration status, among other things, to track progress – or the lack thereof – in reducing gender inequalities and intersectional discrimination regarding key indicators such as legal and effective coverage, adequacy and comprehensiveness, and expenditure with respect to all benefits and services.
Closing data gaps on the coverage, adequacy and comprehensiveness of social protection systems is urgent, and demands collaboration among data producers at the national level (social security institutions and others producing administrative data, and national statistical offices), as well as between national and international bodies that have a mandate for the harmonization of national data sources and a role to play in national capacities to produce social protection data.
We also need better analysis of the extent to which gender equality is addressed in national social protection policies and strategies providing the broad contours of the social protection system that countries want to chart, as well as the specific policy and legal efforts that are made to achieve the vision. We still know too little about many of these facets and their outcomes.
What is clear is that we need further efforts to close gender gaps in access to social protection and to design and implement social protection policies and programmes that can more effectively and systematically address the gender-specific risks and constraints that women face across the life cycle. “Simply calling a social protection system gender-responsive or gender-transformative does not make it so” (Cookson et al. 2023). Fiscal constraints may explain some of the gaps between recognition of gender-specific risks and constraints and putting effective policies to address them in place. Yet the many examples cited in this paper attest to the fact that despite such constraints, policy efforts are under way, while costing studies have also shown that a gender-responsive social protection floor is affordable for most countries.
For example, in low- and middle-income countries, the financing gap to achieve universal social protection coverage for mothers of newborns represents 0.05 per cent of GDP. This is the required investment needed for ensuring a floor-level maternity cash benefit for all mothers of newborns who are currently not receiving any benefit for this contingency (Cattaneo et al. 2024). Likewise, to ensure that all women and men have access to an old-age pension would require an additional investment of 0.3 per cent of the GDP of low- and middle-income countries, or US$115.0 billion, with 67.0 per cent of these resources needed to pay old-age pensions for women.26 These figures give a broad, bird’s eye view of the additional investment needed for two specific areas of social protection, underlining the point that such investment is within the realm of possibility for most countries.
References
Abe, Aya. 2010. “The Changing Shape of the Care Diamond: The Case of Child and Elderly Care in Japan”. Report No.9. UNRISD Gender and Development Programme Paper. UNRISD.
Addati, Laura. 2015. “Extending Maternity Protection to All Women: Trends, Challenges and Opportunities”. International Social Security Review 68 (1): 69–93. https://doi.org/10.1111/issr.12060.
Addati, Laura, Umberto Cattaneo, Valeria Esquivel, and Isabel Valarino. 2018. Care Work and Care Jobs for the Future of Decent Work. ILO. https://www.ilo.org/sites/default/files/wcmsp5/groups/public/%40dgreports/%40dcomm/%40publ/documents/publication/wcms_633135.pdf
Addati, Laura, Umberto Cattaneo, and Emanuela Pozzan. 2022. Care at Work: Investing in Care Leave and Services for a More Gender Equal World of Work. ILO.
Alfers, Laura. 2016. Our Children Do Not Get the Attention They Deserve: A Synthesis of Research Findings on Women Informal Workers and Child Care from Six Membership-Based Organizations. Research Report. Women in Informal Employment: Globalizing and Organizing (WIEGO). https://www.wiego.org/sites/default/files/publications/files/Alfers-Child-Care-Initiative-Full-Report.pdf.
Allen, Jessica, Reuben Balfour, Ruth Bell, and Michael Marmot. 2014. “Social Determinants of Mental Health”. International Review of Psychiatry 26 (4): 392–407.
Allen, Kerry, Rastislav Bednárik, Lorna Campbell, Anja Dieterich, E. Durrett, T. Emilsson, Jon Glasby, P. Gobet, G. Kagialaris, and J. Klavus. 2011. Governance and Finance of Long-Term Care across Europe-Overview Report. https://interlinks.euro.centre.org/sites/default/files/1%20WP6_GOV_FIN_final.pdf
Allen, Kim. 2022. “Re-claiming Resilience and Re-imagining Welfare: A Response to Angela McRobbie”. European Journal of Cultural Studies 25 (1): 310–15. https://doi.org/10.1177/13675494211036922.
Alston, Philip. 2017. Report of the Special Rapporteur on Extreme Poverty and Human Rights (A/HRC/35/26). Geneva: Human Rights Council. https://digitallibrary.un.org/record/842173/files/A_HRC_35_26-EN.pdf?ln=en.
———. 2019. Visit to the United Kingdom of Great Britain and Northern Ireland: Report of the Special Rapporteur on Extreme Poverty and Human Rights (A/HRC/41/39/Add.1). https://documents-dds-ny.un.org/doc/UNDOC/GEN/G19/112/13/PDF/G1911213.pdf?OpenElement.
Amnesty International. 2022a. “Amnesty Statement on Supreme Court Decision to Overturn Roe v. Wade”. https://www.amnesty.org/en/latest/news/2022/06/supreme-court-decision-overturn-roe-wade/.
———. 2022b. “Poland: Regression on Abortion Access Harms Women”. Oxford: Amnesty International. https://www.amnesty.org/en/latest/news/2022/01/poland-regression-on-abortion-access-harms-women/.
Aransiola, Temidayo James, and José Alejandro Ordoñez, Daniella Medeiros Cavalcanti, Gabriel Alves de Sampaio Morais, Dandara de Oliveira Ramos, and Davide Rasella. 2023. “The combined effect of social pensions and cash transfers on child mortality: Evaluating the last two decades in Brazil and projecting their mitigating effect during the global economic crisis”. The Lancet Regional Health – Americas, November. https://doi.org/10.1016/j.lana.2023.100618
Arenas de Mesa, Alberto, and Veronica Montecinos. 1999. “The Privatization of Social Security and Women’s Welfare: Gender Effects of the Chilean Reform”. Latin American Research Review 34 (3): 7–37.
Arenas de Mesa, Alberto, and Claudia Robles, eds. 2024. Non-Contributory Pension Systems in Latin America and the Caribbean: Towards Solidarity with Sustainability. Santiago de Chile: Economic Commission for Latin America and the Caribbean (ECLAC). https://www.cepal.org/en/publications/80540-non-contributory-pension-systems-latin-america-and-caribbean-towards-solidarity
Arza, Camila. 2012. “Pension Reforms and Gender Equality in Latin America”. UNRISD. http://www.unrisd.org/80256B3C005BCCF9/%28httpAuxPages%29/3513162DF26920D5C12579CF0053534B/$file/Arza%20paper.pdf
———. 2015. “The Gender Dimensions of Pension Systems: Policies and Constraints for the Protection of Older Women”, Discussion Paper 1. UN Women. https://socialprotection-humanrights.org/wp-content/uploads/2015/08/ARZA-Fin.pdf
———. 2017. “The Expansion of Economic Protection for Older Adults in Latin America: Key Design Features of Non-Contributory Pensions”. WIDER Working Paper 2017/29. UNU-WIDER.https://www.wider.unu.edu/sites/default/files/wp2017-29.pdf
Atkinson, Anthony. 2015. Inequality: What Can Be Done? Cambridge, MA: Harvard University Press.
Avila, Zulum. 2021. “Public Employment Services That Work for Young People”. In Is the Future Ready for Youth? Youth Employment Policies for Evolving Labour Markets, edited by Sukti Dasgupta and Juan Chacaltana. http://www.ilo.org/employment/Whatwedo/Publications/WCMS_776024/lang--en/index.htm
Barca, Valentina. 2019. Gender-Sensitive Public Works: Literature Review. Oxford: HEART. https://archive.ids.ac.uk/heart/wp-content/uploads/2020/02/Gender-sensitive-public-works-Lit-Review_HEART-format-final.pdf
Barca, Valentina, and Laura Alfers. 2021.“Including Informal Workers within Social Protection Systems: A Summary of Options”. Social Protection Approaches to COVID-19 Expert Advice Service (SPACE), DAI Global UK. https://socialprotection.org/sites/default/files/publications_files/SPACE_Including%20informal%20workers%20within%20social%20protection%20systems_A%20summary%20of%20options_0.pdf
Baru, Rama. Forthcoming. “Public–Private Mix for Continuity of Care for Older Persons: Study of Select Countries in the Asia Pacific Region”. Asia Pacific Observatory, WHO, 11 (2).
Bastagli, Francesca, Jessica Hagen-Zanker, Luke Harman, Valentina Barca, Georgina Sturge, Tanja Schmidt, and Luca Pellerano. 2016. Cash Transfers: What Does the Evidence Say? A Rigorous Review of Programme Impact and of the Role of Design and Implementation Features. ODI (Overseas Development Institute). https://odi.org/en/publications/cash-transfers-what-does-the-evidence-say-a-rigorous-review-of-impacts-and-the-role-of-design-and-implementation-features/
Bastagli, and Abigail Hunt. 2020. “Social Protection and the Future of Work: A Gender Analysis”. Working Paper 590. ODI. https://cdn.odi.org/media/documents/Social_protection_and_the_future_of_work_a_gender_analysis.pdf
Behrendt, Christina. 2000. “Private Pensions - a Viable Alternative? Their Distributive Effects in a Comparative Perspective”. International Social Security Review 53 (3): 3–26.
———. 2017. “Can Graduation Approaches Contribute to Building Social Protection Floors?” Policy in Focus 14 (2): 33–35.
Behrendt, Christina, and Valeria Nesterenko. 2022. “Employment and Social Protection”. In Handbook on Forms of Employment, edited by UNECE, 85–98. https://unece.org/sites/default/files/2022-08/2210309E_ECE_CES_STAT_2022_4_WEB.pdf
Behrendt, Christina, and John Woodall. 2015. “Pensions and Other Social Security Income Transfer Systems”. In Labour Markets, Institutions and Inequality: Building Just Societies in the 21st Century, edited by Janine Berg, 242–62. Cheltenham, UK: Edward Elgar Publishing. https://www.e-elgar.com/shop/gbp/labour-markets-institutions-and-inequality-9781784712099.html
Berkman, Lisa F., and Yenee Soh. 2017. “Social Determinants of Health at Older Ages: The Long Arm of Early and Middle Adulthood”. Perspectives in Biology and Medicine 60 (4): 595–606.
Bernhofer, Juliana, Massimo De Minicis, and Oscar Molina. 2023. “Conditionality in France and Spain: Assessing Workers’ Social Protection System”. Working Paper 111, November. https://oa.inapp.org/xmlui/handle/20.500.12916/4077
Budig, Michelle J. 2014.“The Fatherhood Bonus and The Motherhood Penalty: Parenthood and the Gender Gap in Pay – Third Way”. Third Way (blog). 02 September 2014. https://www.thirdway.org/report/the-fatherhood-bonus-and-the-motherhood-penalty-parenthood-and-the-gender-gap-in-pay.
Budig, Michelle J., and Paula England. 2001.“The Wage Penalty for Motherhood”. American Sociological Review 66 (2): 204–25. https://doi.org/10.2307/2657415
Budig, Michelle J., and Joya Misra. 2010.“How Care-Work Employment Shapes Earnings in Cross-National Perspective”. International Labour Review 149 (4): 441–60. https://doi.org/10.1111/j.1564-913X.2010.00097.x
Budlender, Debbie. 2009. Towards Minimum Wages and Employment Conditions for the Expanded Public Works Programme Phase II. Report Prepared by Community Agency for Social Enquiry (CASE).
Budlender, Debbie, and Francie Lund. 2012. “Care in South Africa: A Legacy of Family Disruption”. In Global Variations in the Political and Social Economy of Care: Worlds Apart. https://www.routledge.com/Global-Variations-in-the-Political-and-Social-Economy-of-Care-Worlds-Apart/Razavi-Staab/p/book/9780415754552
Cattaneo, Umberto, Helmut Schwarzer, Shahra Razavi, and Andrea Visentin. 2024. “Financing Gap for Universal Social Protection: Global, Regional and National Estimates and Strategies for Creating Fiscal Space”. ILO Working Paper 113. https://www.social-protection.org/gimi/Media.action?id=19617
Cichon, Michael, Wolfgang Scholz, Arthur van de Meerendonk, Krzysztof Hagemejer, Fabio Bertranou, and Pierre Plamondon. 2004. Financing Social Protection. Geneva: ILO and ISSA. http://www.ilo.org/wcmsp5/groups/public/---ed_protect/---soc_sec/documents/publication/wcms_secsoc_8030.pdf
Coady, David, Samir Jahan, Riki Matsumoto, and Baoping Shang. 2021. “Guaranteed Minimum Income Schemes in Europe: Landscape and Design”. IMF Working Paper 21/179. https://www.imf.org/en/Publications/WP/Issues/2021/07/02/Guaranteed-Minimum-Income-Schemes-in-Europe-Landscape-and-Design-461341
Commission on Social Determinants of Health, WHO. 2008. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health – Commission on Social Determinants of Health Final Report. https://apps.who.int/iris/bitstream/handle/10665/43943/9789241563703_eng.pdf?sequence=1
Cook, Rose, and Damian Grimshaw. 2020. “A Gendered Lens on COVID-19 Employment and Social Policies in Europe”. European Societies, October: 1–13. https://doi.org/10.1080/14616696.2020.1822538
Cookson, Tara Patricia. 2018. Unjust Conditions. Women’s Work and the Hidden Cost of Cash Transfer Programs. Oakland, CA: University of California Press.
Cookson, Tara Patricia, Nina Ebner, Yardain Amron, and Kritika Kukreja. 2023. “Social Protection Systems and Gender: A Review of the Evidence”. Global Social Policy, 24 (1): 25–45. https://doi.org/10.1177/14680181231180507
Cuesta, Laura. 2022. “Public Guarantee of Child Support: A Key Policy for Improving the Economic Well-Being of Lone-Mother Families”. Policy Brief No. 25. UN Women. https://www.unwomen.org/en/digital-library/publications/2022/08/policy-brief-public-guarantee-of-child-support
Daly, Mary. 2020. “COVID-19 and Care Homes in England: What Happened and Why?” Social Policy & Administration 54 (7): 985–98. https://doi.org/10.1111/spol.12645
Davala, Sarath, Renana Jhabvala, Guy Standing, and Soumya Kapoor Mehta. 2015. Basic Income: A Transformative Policy for India. 1st ed. Bloomsbury Academic. http://dx.doi.org/10.5040/9781472593061
Davis, Benjamin, Sudhanshu Handa, Nicola Hypher, Natalia Winder Rossi, Paul Winters, and Jennifer Yablonski. 2016. From Evidence to Action: The Story of Cash Transfers and Impact Evaluation in Sub-Saharan Africa. Oxford: Oxford University Press. https://global.oup.com/academic/product/from-evidence-to-action-9780198769446
Desai, Aditi. 2023. “Heat-Linked Parametric Insurance System Offers Climate Change Lifeline for Indian Women in the Informal Sector”. Journal of Public and International Affairs (blog). 06 October 2023. https://jpia.princeton.edu/news/heat-linked-parametric-insurance-system-offers-climate-change-lifeline-indian-women-informal
Diwakar, Vidya, and Andrew Shepherd. 2021. “Sustaining Escapes from Poverty”. World Development, 151. https://doi.org/10.1016/j.worlddev.2021.105611
Dorn, Franziska, Nancy Folbre, Leila Gautham, and Martha Macdonald. 2023. “Cheap Praise: Supplemental Pay for Essential Workers in the 2020 COVID-19 Pandemic”. In From Crisis to Catastrophe: Care, COVID, and Pathways to Change, edited by Mignon Duffy, Amy Armenia, and Kim Price-Glynn, 115–33. Ithaca, NY: Rutgers University Press. https://doi.org/10.36019/9781978828599-016
Drago, Robert. 2010. “Sick at Work: Infected Employees in the Workplace During the H1N1 Pandemic”. Institute for Women’s Policy Research. https://iwpr.org/wp-content/uploads/2020/11/B284.pdf
Duvvury, Nata, Aoife Callan, Patrick Carney, and Srinivas Raghavendra. 2013. Intimate Partner Violence: Economic Costs and Implications for Growth and Development. Women’s Voice, Agency, & Participation Research Series 3. Washington DC: World Bank. https://openknowledge.worldbank.org/handle/10986/16697
Ehmke, Ellen. 2015. National Experiences in Building Social Protection Floors: India’s Mahatma Gandhi National Rural Employment Guarantee Scheme. ESS Paper No. 49. ILO. http://www.social-protection.org/gimi/gess/RessourcePDF.action?ressource.ressourceId=53326
Elson, Diane. 2005. “Unpaid Work, the Millennium Development Goals, and Capital Accumulation”. Conference on Unpaid Work and the Economy: Gender, Poverty, and the Millennium Development Goals. New York: Levy Economics Institute. https://www.levyinstitute.org/undp-levy-conference/papers/paper_Elson.pdf
England, Paula, Michelle Budig, and Nancy Folbre. 2002. “Wages of Virtue: The Relative Pay of Care Work”. Social Problems 49 (4): 455–73. https://doi.org/10.1525/sp.2002.49.4.455
European Commission, Directorate-General for Employment, Social Affairs and Inclusion. 2021. Long-Term Care Report: Trends, Challenges and Opportunities in an Ageing Society. Volume I. Luxembourg: Publications Office of the European Union. https://data.europa.eu/doi/10.2767/677726
———. 2023. “Your rights country by country: Slovakia”. https://ec.europa.eu/social/main.jsp?catId=1127&langId=en
Ewig, Christina. 2006. “Global Processes, Local Consequences: Gender Equity and Health Sector Reform in Peru”. Social Politics: International Studies in Gender, State & Society 13 (3): 427–55. https://doi.org/10.1093/sp/jxl002
FCDO, UNICEF, HEART, and ODI. 2021. Social Protection and Gender Equality Outcomes Across the Life-Course: A Synthesis of Recent Findings. https://www.unicef.org/media/112591/file/Social-Protection-Gender-Equality-Outcomes-Across-the-Lifecycle-Full-Report.pdf
Folbre, Nancy. 1994. “Children as Public Goods”. The American Economic Review 84 (2): 86–90.
Folbre, Nancy, Leila Gautham, and Kristin Smith. 2021. “Essential Workers and Care Penalties in the United States”. Feminist Economics 27 (1–2): 173–87. https://doi.org/10.1080/13545701.2020.1828602
Fortin, Pierre. 2017. “What Have Been the Effects of Quebec’s Universal Childcare System on Women’s Economic Security?”. Brief Submitted to the Standing Committee on the Status of Women (FEWO) of the House of Commons, Ottawa. https://www.ourcommons.ca/content/Committee/421/FEWO/Brief/BR8806290/br-external/FortinPierre-e.pdf
Fortin, Pierre, Luc Godbout, and Suzie St-Cerny. 2013. “L’impact des services de garde à contribution réduite du Québec sur le taux d’activité féminin, le revenu intérieur et les budgets gouvernementaux”. Revue Interventions économiques. Papers in Political Economy, 47. https://doi.org/10.4000/interventionseconomiques.1858.
Freeland, Nicholas. 2012. “Re: Silly-Ence – or the Reinvention of Vulnerability Nicholas Freeland”. Pathways’ Perspectives on Social Policy in International Development, 8. Development Pathways. https://www.developmentpathways.co.uk/wp-content/uploads/2012/12/8-PathwaysPerspective-Re-silly-ence-%E2%80%93-or-the-Reinvention-of-Vulnerability-PP8.pdf.
Frota, Luis, Lou Tessier, Christian Pfleiderer, and Zhao Ying. 2020. “International Review of Financial Protection in Maternal Health Care”. Technical Note 2. ILO Regional Office for Asia and the Pacific. https://www.ilo.org/wcmsp5/groups/public/---asia/---ro-bangkok/---ilo-beijing/documents/briefingnote/wcms_765077.pdf.
Fukuda-Parr, Sakiko, James Heintz, and Stephanie Seguino. 2015. Critical and Feminist Perspectives on Financial and Economic Crises. Routledge. https://www.routledge.com/Critical-and-Feminist-Perspectives-on-Financial-and-Economic-Crises/Fukuda-Parr-Heintz-Seguino/p/book/9781138886377.
Fultz, Elaine. 2011. Pension Crediting for Caregivers: Policies in Finland, France, Germany, Sweden, the United Kingdom, Canada and Japan. Washington, DC: Institute for Women’s Policy Research. https://iwpr.org/wp-content/uploads/2020/12/D497_Fultz.pdf.
Fultz, Elaine, and John Francis. 2013. “Cash Transfer Programmes, Poverty Reduction and Empowerment of Women: A Comparative Analysis – Experiences from Brazil, Chile, India, Mexico and South Africa”. GED Working Paper 4. ILO. http://www.ilo.org/wcmsp5/groups/public/---dgreports/---gender/documents/publication/wcms_233599.pdf.
Gavrilovic, Maja, Monica Rubio, Francesca Bastagli, Roopa Hinton, Silke Staab, Ruth Graham Goulder, Charlotte Bilo, et al. 2022. “Gender-Responsive Social Protection Post–COVID-19”. Science 375 (6585): 1111–13. https://doi.org/10.1126/science.abm5922.
GBD 2019 Mental Disorders Collaborators. 2022. “Global, Regional, and National Burden of 12 Mental Disorders in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019”. The Lancet Psychiatry 9 (2): 137–150. https://doi.org/10.1016/S2215-0366(21)00395-3.
Geleto, Ayele, Catherine Chojenta, Abdulbasit Musa, and Deborah Loxton. 2018. “Barriers to Access and Utilization of Emergency Obstetric Care at Health Facilities in Sub-Saharan Africa: A Systematic Review of Literature”. Systematic Reviews 7 (1): 183. https://doi.org/10.1186/s13643-018-0842-2.
Gentilini, Ugo. 2022. Cash Transfers in Pandemic Times: Evidence, Practices, and Implications from the Largest Scale Up in History. World Bank Group. https://documents1.worldbank.org/curated/en/099800007112236655/pdf/P17658505ca3820930a254018e229a30bf8.pdf.
Gentilini, Ugo, Margaret Grosh, Jamele Rigolini, and Ruslan Yemtsov. 2020. Exploring Universal Basic Income: A Guide to Navigating Concepts, Evidence, and Practices. Washington, DC: World Bank. https://openknowledge.worldbank.org/handle/10986/32677.
GHWA (Global Health Workforce Alliance) and WHO (World Health Organization). 2013. A Universal Truth: No Health Without A Workforce. GHWA (Global Health Workforce Alliance) and WHO (World Health Organization). https://www.who.int/publications/m/item/hrh_universal_truth.
Gibbons, Luz, José M. Belizan, Jeremy A. Lauer, Ana P. Betran, Mario Merialdi, and Fernando Althabe. 2012. “Inequities in the Use of Cesarean Section Deliveries in the World”. American Journal of Obstetrics and Gynecology 206 (4): 331.e1-331.e19. https://doi.org/10.1016/j.ajog.2012.02.026.
Gorz, André. 1989. Critique of Economic Reason. New York: Verso Press.
———. 1999. Reclaiming Work: Beyond the Wage-Based Society. Cambridge: Polity Press.
Gough, Ian. 2019. “Universal Basic Services: A Theoretical and Moral Framework”. The Political Quarterly 90 (3): 534–42. https://doi.org/10.1111/1467-923X.12706.
Government of Chile. 2023. “Chileatiende: Ingreso Ético Familiar (IEF)”. Santiago de Chile: Ministerio de Desarrollo Social y Familia. https://www.chileatiende.gob.cl/fichas/20055-ingreso-etico-familiar-ief.
Government of India. 2023. “Participation of Women Worker in Mahatma Gandhi National Rural Employment Guarantee Scheme”. Ministry of Rural Development. https://rural.gov.in/en/press-release/participation-women-worker-mahatma-gandhi-national-rural-employment-guarantee-scheme
Gromada, Anna, and Dominic Richardson. 2021. “Where Do Rich Countries Stand on Childcare? Assessing the Parental Leave and Childcare Policies in 41 High-Income Countries Using the Most Recent Comparable Data”. UNICEF Office of Research– Innocenti. https://www.unicef.org/innocenti/media/5431/file/UNICEF-Where-Do-Rich-Countries-Stand-on-Childcare-2021.pdf.
Grosh, Margaret, Philippe Leite, Matthew Wai-Poi, and Emil Tesliuc. 2022. Revisiting Targeting in Social Assistance: A New Look at Old Dilemmas. Washington, DC: World Bank. https://openknowledge.worldbank.org/handle/10986/37228.
Hanlon, Joseph, Armando Barrientos, and David Hulme. 2010. Just Give Money to the Poor: The Development Revolution from the Global South. Boulder, CO; London: Kumarian Press.
Heintz, James. 2019. The Economy’s Other Half: How Taking Gender Seriously Transforms Macroeconomics. Newcastle-upon-Tyne: Agenda Publishing.
Holmes, Rebecca, and Nicola Jones. 2013. Gender and Social Protection in the Developing World: Beyond Mothers and Safety Nets. London and New York: Zed Books.
Howard, Neil. 2019. “Universal Basic Income: A Way through the Storm?” OpenDemocracy. https://www.opendemocracy.net/en/beyond-trafficking-and-slavery/universal-basic-income-way-through-storm/.
Hunter, Wendy, Leila Patel, and Natasha Borges Sugiyama. 2021. “How Family and Child Cash Transfers Can Empower Women: Comparative Lessons from Brazil and South Africa”. Global Social Policy 21 (2): 258–77. https://doi.org/10.1177/1468018120981421.
ILO. 2004. Economic Security for a Better World.
———. 2008. Social Health Protection: An ILO Strategy towards Universal Access to Health Care. https://www.social-protection.org/gimi/gess/Media.action;jsessionid=fVdt6lyHlZfssluTmIn09XLuRgbMe2AWKZNwMTNq3ZhvkyG67dsQ!-458942951?id=9473
———. 2010. Extending Social Security to All. A Guide through Challenges and Options. https://www.ilo.org/sites/default/files/wcmsp5/groups/public/%40dgreports/%40dcomm/%40publ/documents/publication/wcms_146616.pdf.
———. 2015. Social Protection for Maternity: Key Policy Trends and Statistics. https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---soc_sec/documents/publication/wcms_366590.pdf.
———. 2016a. Maternity Cash Benefits for Workers in the Informal Economy. http://www.social-protection.org/gimi/gess/RessourcePDF.action?ressource.ressourceId=54094.
———. 2016b. Non-Standard Employment around the World: Understanding Challenges, Shaping Prospects. https://www.ilo.org/global/publications/books/WCMS_534326/lang--en/index.htm.
———. 2016c. Women at Work: Trends 2016. http://www.ilo.org/wcmsp5/groups/public/---dgreports/---dcomm/---publ/documents/publication/wcms_457317.pdf.
———. 2017. World Social Protection Report 2017–19: Universal Social Protection to Achieve the Sustainable Development Goals. https://www.ilo.org/publications/world-social-protection-report-2017-19-universal-social-protection-achieve
———. 2018a. Care Work and Care Jobs for the Future of Decent Work. https://www.ilo.org/wcmsp5/groups/public/---dgreports/---dcomm/---publ/documents/publication/wcms_633135.pdf.
———. 2018b. Decent Working Time for Nursing Personnel: Critical for Worker Well-Being and Quality Care. https://www.ilo.org/wcmsp5/groups/public/---ed_dialogue/---sector/documents/publication/wcms_655277.pdf.
———. 2018c. Global Wage Report 2018/19: What Lies behind Gender Wage Gaps. https://www.ilo.org/wcmsp5/groups/public/---dgreports/---dcomm/---publ/documents/publication/wcms_650553.pdf.
———. 2019a. A Quantum Leap for Gender Equality: For a Better Future of Work for All. https://www.ilo.org/wcmsp5/groups/public/---dgreports/---dcomm/---publ/documents/publication/wcms_674831.pdf.
———. 2019b. Universal Social Protection for Human Dignity, Social Justice and Sustainable Development: General Survey Concerning the Social Protection Floors Recommendation, 2012 (No. 202). ILC.108/III/B. https://www.ilo.org/wcmsp5/groups/public/---ed_norm/---relconf/documents/meetingdocument/wcms_673680.pdf.
———. 2019c. Working on a Warmer Planet: The Impact of Heat Stress on Labour Productivity and Decent Work. https://www.ilo.org/wcmsp5/groups/public/---dgreports/---dcomm/---publ/documents/publication/wcms_711919.pdf.
———. 2020a. A Gender-Responsive Employment Recovery: Building Back Fairer. https://www.ilo.org/wcmsp5/groups/public/---ed_emp/documents/publication/wcms_751785.pdf.
———. 2020b. COVID-19 and the Health Sector. https://www.ilo.org/wcmsp5/groups/public/---ed_dialogue/---sector/documents/briefingnote/wcms_741655.pdf.
———. 2020c. Extending Social Protection to Informal Workers in the COVID-19 Crisis: Country Responses and Policy Considerations. https://www.social-protection.org/gimi/RessourcePDF.action?id=56833.
———. 2020d. Sickness Benefits: An Introduction. https://www.ilo.org/secsoc/information-resources/publications-and-tools/Brochures/WCMS_744506/lang--en/index.htm.
———. 2020e. Sickness Benefits during Sick Leave and Quarantine: Country Responses and Policy Considerations in the Context of COVID-19. https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---soc_sec/documents/publication/wcms_744510.pdf.
———. 2020f. Towards Universal Health Coverage: Social Health Protection Principles. https://www.social-protection.org/gimi/RessourcePDF.action?id=56009.
———. 2020g. Unemployment Protection in the COVID-19 Crisis: Country Responses and Policy Considerations. https://www.social-protection.org/gimi/RessourcePDF.action?id=56834.
———. 2021a. Adapting Social Insurance to Women’s Life Courses: A Gender Impact Assessment of Viet Nam. https://www.ilo.org/wcmsp5/groups/public/---asia/---ro-bangkok/---ilo-hanoi/documents/publication/wcms_819801.pdf.
———. 2021b. Assessment of the Maternity Insurance in Jordan. http://www.ilo.org/beirut/publications/WCMS_776223/lang--en/index.htm.
———. 2021c. Building Forward Fairer: Women’s Rights to Work and at Work at the Core of the COVID-19 Recovery. https://www.ilo.org/publications/building-forward-fairer-womens-rights-work-and-work-core-covid-19-recovery
———. 2021d. Building Social Protection Systems: International Standards and Human Rights Instruments. https://www.ilo.org/publications/building-social-protection-systems-international-standards-and-human-rights.
———. 2021e. Extending Social Health Protection: Accelerating Progress towards Universal Health Coverage in Asia and the Pacific. https://www.social-protection.org/gimi/ShowRessource.action?id=38425.
———. 2021f. Extending Social Security to Domestic Workers: Lessons from International Experience. https://www.social-protection.org/gimi/gess/RessourcePDF.action?id=55723.
———. 2021g. Extending Social Security to Self-Employed Workers: Lessons from International Experience. https://www.social-protection.org/gimi/gess/RessourcePDF.action?id=55726.
———. 2021h. Extending Social Security to Workers in the Informal Economy: Lessons from International Experience. https://www.social-protection.org/gimi/Media.action?id=16990.
———. 2021i. Intervention Model: For Extending Social Protection to Migrant Domestic Workers. http://www.ilo.org/global/topics/labour-migration/publications/WCMS_826718/lang--en/index.htm.
———. 2021j. World Social Protection Report 2020–22: Social Protection at the Crossroads – in Pursuit of a Better Future. https://www.ilo.org/publications/flagship-reports/world-social-protection-report-2020-22-social-protection-crossroads-pursuit
———. 2022a. Care at Work: Investing in Care Leave and Services for a More Gender Equal World of Work. https://www.ilo.org/publications/major-publications/care-work-investing-care-leave-and-services-more-gender-equal-world-work.
———. 2022b. Global Employment Trends for Youth 2022: Investing in Transforming Futures for Young People. http://www.ilo.org/global/publications/books/WCMS_853321/lang--en/index.htm.
———. 2022c. Global Wage Report 2022-2023: The Impact of Inflation and COVID-19 on Wages and Purchasing Power. https://www.ilo.org/digitalguides/en-gb/story/globalwagereport2022-23.
———. 2022d. Making Decent Work a Reality for Domestic Workers: Progress and Prospects Ten Years after the Adoption of the Domestic Workers Convention, 2011 (No. 189). http://www.ilo.org/global/topics/domestic-workers/publications/WCMS_802551/lang--en/index.htm.
———. 2022e. Making the Right to Social Security a Reality for Domestic Workers: A Global Review of Policy Trends, Statistics and Extension Strategies. https://www.ilo.org/global/publications/books/WCMS_848280/lang--en/index.htm.
———. 2022f. Securing Decent Work for Nursing Personnel and Domestic Workers, Key Actors in the Care Economy. ILC110/III/(B). https://www.ilo.org/sites/default/files/wcmsp5/groups/public/%40ed_norm/%40relconf/documents/meetingdocument/wcms_839652.pdf.
———. 2023a. Aligning Skills Development and National Social Protection Systems. https://www.ilo.org/sites/default/files/wcmsp5/groups/public/%40ed_protect/%40soc_sec/documents/publication/wcms_900970.pdf.
———. 2023b. The Benefits of Investing in Transformative Childcare Policy Packages towards Gender Equality and Social Justice. https://labordoc.ilo.org/discovery/delivery/41ILO_INST:41ILO_V2/12119347050002676.
———. 2023c. What Labour Force Survey Data Can Tell Us about the Workforce in the Health and Social Care Sector: A Review of Data from 56 Countries. https://www.ilo.org/media/361016/download.
———. 2023d. Women and Men in the Informal Economy: A Statistical Update. https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---travail/documents/publication/wcms_869188.pdf.
———. 2023e. World Employment and Social Outlook 2023: The Value of Essential Work. http://www.ilo.org/global/research/global-reports/weso/WCMS_871016/lang--en/index.htm.
———. 2023f. World Employment and Social Outlook: Trends 2023. https://doi.org/10.54394/SNCP1637.
———. 2024a. Report of the Committee of Experts on the Application of Conventions and Recommendations (Articles 19, 22 and 35 of the Constitution) – General Report and Observations concerning Particular Countries). ILC.112/III(A). https://www.ilo.org/wcmsp5/groups/public/---ed_norm/---relconf/documents/meetingdocument/wcms_911183.pdf.
———. 2024b. Decent Work and the Care Economy. ILC.112/Report VI. https://www.ilo.org/wcmsp5/groups/public/---ed_norm/---relconf/documents/meetingdocument/wcms_921863.pdf.
———. 2024c. Disability Schemes and Programmes around the World: Design and Compliance with International Social Security Standards. https://www.social-protection.org/gimi/Media.action?id=19403.
———. 2024d. Extending Social Health Protection: Accelerating Progress towards Universal Health Coverage in Central and Western Asia. https://www.social-protection.org/gimi/ShowRessource.action?id=58650.
———. 2024e. General Discussion Committee on Decent Work and the Care Economy. ILC.112/CDG/D.1. https://www.ilo.org/international-labour-conference/112th-session-international-labour-conference/general-discussion-committee-decent-work-and-care-economy-112th-session
———. 2024f. The Impact of Care Responsibilities on Women’s Labour Force Participation. https://www.ilo.org/sites/default/files/2024-10/GEDI-STAT%20brief_formatted_28.10.24_final.pdf.
———. 2024g. World Social Protection Report 2024-2026: Universal Social Protection for Climate Action and a Just Transition. https://www.ilo.org/publications/flagship-reports/world-social-protection-report-2024-26-universal-social-protection-climate
———. Forthcoming a. Developing a Rights-Based Framework to Assess Poverty-Targeted Social Assistance in MENA.
———. Forthcoming b. Extending Social Health Protection: Accelerating Progress towards Universal Health Coverage in Latin America.
ILO and ISSA (International Social Security Association). 2023. Universal Access to Social Protection and Ensuring Basic Income Security. https://www.ilo.org/wcmsp5/groups/public/---dgreports/---dcomm/documents/genericdocument/wcms_882455.pdf.
ILO and NHIF (National Health Insurance Fund of Kenya). 2023. The Introduction of a Maternity Cash Benefit in Kenya. https://www.social-protection.org/gimi/Media.action?id=19372.
ILO and OECD (Organisation for Economic Co-operation and Development). 2020. Women at Work in G20 Countries: Policy Action since 2020. https://www.oecd-ilibrary.org/docserver/db32ba54-en.pdf?expires=1732038902&id=id&accname=guest&checksum=82228E47B8D4433256A2272D3410AFC5.
ILO and UNICEF (United Nations Children’s Fund). 2019. Towards Universal Social Protection for Children: Achieving SDG 1.3. https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---soc_sec/documents/publication/wcms_669336.pdf.
———. 2023. More than a Billion Reasons: The Urgent Need to Build Universal Social Protection for Children. https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---soc_sec/documents/publication/wcms_869602.pdf.
ILO, UNICEF and Learning for Well-Being Institute. 2024. The Promise of Universal Child Benefits: The Foundational Policy for Economic and Social Development. https://www.social-protection.org/gimi/Media.action?id=19447.
ILO and WIEGO. 2020a. Extending Childcare Services to Workers in the Informal Economy: Policy Lessons from Country Experiences. https://www.ilo.org/wcmsp5/groups/public/---dgreports/---gender/documents/genericdocument/wcms_737555.pdf.
———. 2020b. Labour and Human Rights Frameworks Promoting Childcare for All Workers. https://www.ilo.org/wcmsp5/groups/public/---dgreports/---gender/documents/genericdocument/wcms_737553.pdf.
———. 2020c. Quality Childcare Services for Workers in the Informal Economy. https://www.ilo.org/wcmsp5/groups/public/---dgreports/---gender/documents/genericdocument/wcms_737551.pdf.
Institute for Fiscal Studies. 2023. Early Years Spending Update: Budget Reforms and Beyond IFS Report R274. September 2023. https://ifs.org.uk/publications/early-years-spending-update-budget-reforms-and-beyond.
IOE (International Organisation of Employers). 2023. “Spain: New Law on Menstrual Sick Leave”. Industrial Relations and Labour Law Newsletter, March 2023. https://industrialrelationsnews.ioe-emp.org/industrial-relations-and-labour-law-march-2023/news/article/spain-new-law-on-menstrual-sick-leave.
ISSA (International Social Security Association). 2017. Megatrends and Social Security: Family and Gender. https://www.issa.int/sites/default/files/documents/publications/2-Megatrends%20Gender%20Family-Final-217637.pdf
———. 2020. Responses to the COVID-19 crisis: Can COVID-19 Be Considered an Occupational Disease? https://www.issa.int/analysis/can-covid-19-be-considered-occupational-disease.
———. 2022. Asia and the Pacific: Priorities for Social Security – Trends, Challenges and Solutions. https://www.issa.int/sites/default/files/documents/2022-02/2-Priorities-report-asia.pdf
James, Phil. 2019. “Sick Pay, Compensation and the Future of Work”. In Safety and Health at the Future of Work. A Compilation of Think Pieces, 30–33. Geneva: ILO. https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---safework/documents/genericdocument/wcms_681841.pdf.
Jenson, Jane, and Denis Saint-Martin. 2003. “New Routes to Social Cohesion? Citizenship and the Social Investment State”. The Canadian Journal of Sociology/Cahiers Canadiens de Sociologie 28 (1): 77–99. https://doi.org/10.2307/3341876.
Joseph Rowntree Foundation. 2023. “Guarantee Our Essentials: Reforming Universal Credit to Ensure We Can All Afford the Essentials in Hard Times”. JRF Blog. 27 February 2024 https://www.jrf.org.uk/report/guarantee-our-essentials.
Joshua, Laurie. 2017. “Aging and Long Term Care Systems: A Review of Finance and Governance Arrangements in Europe, North America and Asia-Pacific”. Social Protection and Labor Discussion Paper 1705. World Bank Group. https://documents.worldbank.org/en/publication/documents-reports/documentdetail/761221511952743424/aging-and-long-term-care-systems-a-review-of-finance-and-governance-arrangements-in-europe-north-america-and-asia-pacific
Kabeer, Naila, Shahra Razavi, and Yana van der Meulen Rodgers. 2021. “Feminist Economic Perspectives on the COVID-19 Pandemic”. Feminist Economics 27 (1–2): 1–29. https://doi.org/10.1080/13545701.2021.1876906.
Kangas, Olli, and Minna Ylikännö. 2023. “Basic Income and the Status of Women in an Established Gender-Equal Welfare State: Results from the Finnish Basic Income Experiment”. International Journal of Environmental Research and Public Health 20 (3): 1733. https://doi.org/10.3390/ijerph20031733.
Karamessini, Maria, and Jill Rubery. 2013. Women and Austerity: The Economic Crisis and the Future for Gender Equality. Routledge.
Kaushik, Urvashi, Preksha Golchha, Madhumitha Hebbar, and Misaki Akasaka Ueda. 2023. “Integrate but How? Lessons from an Integrated Universal Child Grant in Bihar, India”. In Social Protection in East Asia and Pacific: From Evidence to Action for Children – Lessons from Strengthening Social Protection Systems. UNICEF Regional Office for East Asia and Pacific. https://www.unicef.org/eap/media/13666/file/UNICEF%20From%20Evidence%20to%20Action%20for%20Children.pdf.
Kentikelenis, Alexandros, and Thomas Stubbs. 2023. A Thousand Cuts: Social Protection in the Age of Austerity. Oxford; New York: Oxford University Press. https://global.oup.com/academic/product/a-thousand-cuts-9780190637736?cc=ch&lang=en&.
Kidd, Stephen. 2009. “Equal Pensions, Equal Rights: Achieving Universal Pension for Older Women and Men in Developing Countries”. Gender and Development 17 (3): 377–88.
Kidd, Stephen, and Diloá Athias. 2020. “Hit and Miss: An Assessment of Targeting Effectiveness in Social Protection with Additional Analysis”. Working Paper. Development Pathways. https://www.developmentpathways.co.uk/wp-content/uploads/2019/03/Hit-and-miss-long-report-.pdf.
Kidd, Stephen, and Diloá Bailey-Athias. 2017. “The Effectiveness of the Graduation Approach: What Does the Evidence Tell Us?” Policy in Focus 14 (2): 22–28.
Kishani Farahani, Najme, Zulfikur Ali Khan, and Ian Orton. 2019. “Universal Child Benefit Case Studies: The Experience of Iran”. UNICEF. https://www.unicef.org/media/70456/file/IRN-case-study-2020.pdf.
Knaul, Felicia, Rebeca Wong, Héctor Arreola-Ornelas, Oscar Méndez, Ricardo Bitran, Antonio Campino, Carmen-Elisa Florez, Ursula Giedion, Daniel Maceira, and Magdalena Rathe. 2011. “Household Catastrophic Health Expenditures: A Comparative Analysis of Twelve Latin American and Caribbean Countries”. Salud Pública de México 53 (January): 85–95.
Laenen, Tijs, and Dimitri Gugushvili. 2021. “Are Universal Welfare Policies Really More Popular than Selective Ones? A Critical Discussion of Empirical Research”. International Journal of Sociology and Social Policy 41 (9/10): 1134–47. https://doi.org/10.1108/IJSSP-01-2021-0010.
Laszlo, Sonia. 2019. “The Gender Transformative Potential of Graduation Programs”. GrOW Research Working Paper Series, 25. Institute for the Study of International Development, McGill University. https://grow.research.mcgill.ca/publications/working-papers/gwp-2019-25.pdf.
Lawn, Joy E., Hannah Blencowe, Mary V. Kinney, Fiorella Bianchi, and Wendy J. Graham. 2016. “Evidence to Inform the Future for Maternal and Newborn Health”. Best Practice & Research. Clinical Obstetrics & Gynaecology 36:169–83. https://doi.org/10.1016/j.bpobgyn.2016.07.004.
Lemma, Melisew Dejene, Tesfaye Semela Kukem, Siera Vercillo, and Logan Cochrane. 2023. “Norms, Equity and Social Protection: A Gender Analysis of the Productive Safety Net Programme in Ethiopia”. Forum for Development Studies 50 (1): 159–81. https://doi.org/10.1080/08039410.2022.2096482.
Liu, Hongyan, Dian Yu, and Hui Wang. 2020. “A Review of the Development of Maternity Leave Policy in China over the Past 70 Years”. China Population and Development Studies 3 (2): 172–87. https://doi.org/10.1007/s42379-019-00038-1.
Lloyd-Sherlock, Peter. 2017. “Pathways to Accessible, Affordable and Gender-Responsive Care Services for Older Persons.” Background Paper prepared for Progress of the World’s Women 2019–2020. UN Women.
———. 2019. “Long-Term Care for Older People in South Africa: The Enduring Legacies of Apartheid and HIV/AIDS”. Journal of Social Policy 48 (1): 147–67. https://doi.org/10.1017/S0047279418000326.
Lloyd-Sherlock, Peter, Karla Giacomin, Poliana Fialho de Carvalho, and Quesia Nayrane Ferreira de Sousa. 2022. “Integrated Long-Term Care Partnerships between Government Social Care and Health Agencies in Brazil: The Belo Horizonte Model”. International Social Security Review 75 (3–4): 103–20. https://doi.org/10.1111/issr.12309.
Lloyd-Sherlock, Peter, Karla Cristina Giacomin, Poliana Fialho de Carvalho, and Lucas Sempé. 2024. Programa Maior Cuidado: An Integrated Community-Based Intervention on Care for Older People. Technical Note. IADB. https://doi.org/10.18235/0005535.
Lönnroth, Knut, Lou Tessier, Gunnel Hensing, and Christina Behrendt. 2020. “Income Security in Times of Ill Health: The Next Frontier for the SDGs”. BMJ Global Health 5 (6). https://doi.org/10.1136/bmjgh-2020-002493.
Lozano, Rafael, Nancy Fullman, John Everett Mumford, Megan Knight, Celine M. Barthelemy, Cristiana Abbafati, Hedayat Abbastabar, Foad Abd-Allah, Mohammad Abdollahi, and Aidin Abedi. 2020. “Measuring Universal Health Coverage Based on an Index of Effective Coverage of Health Services in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019”. The Lancet 396 (10258): 1250–84.
Marmot, Michael. 2001. “Economic and Social Determinants of Disease”. Bulletin of the World Health Organization 79: 988–89.
McCarthy, Carey, Mathieu Boniol, Ka Daniels, G. Cometto, K. Diallo, A. D. Lawani, and J. Campbell. 2020. State of the World’s Nursing 2020: Investing in Education, Jobs, and Leadership. WHO. https://www.who.int/publications/i/item/9789240003279
McClanahan, Shea, and Björn Gelders. 2019. Assessing the Potential for Multi-Tiered Child Benefits in Viet Nam. Geneva: ILO. https://www.developmentpathways.co.uk/wp-content/uploads/2019/11/ILO-Multi-tiered.pdf.
McCord, Anna, Maikel Lieuw-Kie-Song, Christina Behrendt, and Mito Tsukamoto. 2024. Public Employment Programmes at the Intersection of Employment and Social Protection Policies. ILO. https://www.ilo.org/publications/public-employment-programmes-intersection-employment-and-social-protection.
Medgyesi, Márton, and Zsolt Temesváry. 2013. “Conditional Cash Transfers in High-Income Countries and Their Impact on Human Capital Accumulation”. AIAS, GINI Discussion Paper 84. https://www1feb-uva.nl/aias/84-6-1-4.pdf.
Memirie, Solomon Tessema, Mieraf Taddesse Tolla, Dawit Desalegn, Mengistu Hailemariam, Ole Frithjof Norheim, Stéphane Verguet, and Kjell Arne Johansson. 2019. “A Cost-Effectiveness Analysis of Maternal and Neonatal Health Interventions in Ethiopia”. Health Policy and Planning 34 (4): 289–97. https://doi.org/10.1093/heapol/czz034.
Molyneux, Maxine. 2006. “Mothers at the Service of the New Poverty Agenda: Progresa/Oportunidades, Mexico’s Conditional Transfer Programme”. Social Policy and Administration 40 (4): 385–424.
———. 2007. Change and Continuity in Social Protection in Latin America: Mothers at the Service of the State? UNRISD.
Moussié, Rachel. 2016. “Women Informal Workers Mobilizing for Child Care”. Research Paper. Durban: WIEGO. https://www.wiego.org/sites/default/files/publications/files/Moussie%CC%81-Mobilizing-for-Child-Care.pdf.
Muñoz Boudet, Ana María, Antra Bhatt, Ginette Azcona, Jayne Yoo, and Kathleen Beegle. 2021. “A Global View of Poverty, Gender, and Household Composition”. Policy Research Working Paper 9553. World Bank.
Nguyen, Long H., David A. Drew, Mark S. Graham, Amit D. Joshi, Chuan-Guo Guo, Wenjie Ma, Raaj S. Mehta, et al. 2020. “Risk of COVID-19 among Front-Line Health-Care Workers and the General Community: A Prospective Cohort Study”. The Lancet Public Health 5 (9): e475–83. https://www.thelancet.com/journals/lanpub/article/PIIS2468-26672030164-X/fulltext.
Nys, Evelien, Sara Pauwels, Balázs Ádám, João Amaro, Athanasios Athanasiou, Osnat Bashkin, Tatjana Kofol Bric, et al. 2023. “Recognition of COVID-19 with Occupational Origin: A Comparison between European Countries”. Occupational and Environmental Medicine 80 (12): 694–701. https://doi.org/10.1136/oemed-2022-108726.
OECD. 2016. “Parental Leave: Where Are the Fathers?” Policy Brief.
———. 2020. Who Cares? Attracting and Retaining Care Workers for the Elderly. https://doi.org/10.1787/92c0ef68-en.
———. 2021. Pensions at a Glance 2021: OECD and G20 Indicators. Paris: OECD. https://www.oecd-ilibrary.org/docserver/ca401ebd-en.pdf?expires=1645674160&id=id&accname=guest&checksum=890070854FF299DDEBDF39D21B191803.
———. 2023. Boosting Social Inclusion in Spain: Improving Pathways and Co-Ordination of Services. Paris: Organisation for Economic Co-operation and Development. https://doi.org/10.1787/56b604a0-en.
Ortiz, Isabel, Christina Behrendt, Andrés Acuña Ulate, and Quynh Anh Nguyen. 2018. “Universal Basic Income Proposals in Light of ILO Standards: Key Issues and Global Costing”. Extension of Social Security (ESS) Paper Series, 62. ILO. http://www.social-protection.org/gimi/gess/RessourcePDF.action?ressource.ressourceId=55171.
Orton, Ian. 2014. “Conditional Cash Transfers and the Human Right to Social Security”. Social Protection and Human Rights (blog), 27 May 2014. https://socialprotection-humanrights.org/expertcom/conditional-cash-transfers-and-the-human-right-to-social-security/.
Orton, Ian, Kroum Markov, and Maya Stern-Plaza. 2024. “What Role for Emergency Basic Income in Building and Strengthening Rights-Based Universal Social Protection Systems? ” International Social Security Review 77 (1–2): 17–34. https://doi.org/10.1111/issr.12358.
Parijs, Philippe Van. 1997. Real Freedom for All: What (If Anything) Can Justify Capitalism? Oxford: Oxford University Press. https://doi.org/10.1093/0198293577.001.0001.
Patel, Vikram, Shekhar Saxena, Crick Lund, Graham Thornicroft, Florence Baingana, Paul Bolton, Dan Chisholm, et al. 2018. “The Lancet Commission on Global Mental Health and Sustainable Development”. The Lancet 392 (10157): 1553–98. https://doi.org/10.1016/S0140-6736(18)31612-X.
Pega, Frank, Sze Yan Liu, Stefan Walter, Roman Pabayo, Ruhi Saith, and Stefan K Lhachimi. 2017. “Unconditional Cash Transfers for Reducing Poverty and Vulnerabilities: Effect on Use of Health Services and Health Outcomes in Low‐ and Middle‐income Countries”. Cochrane Database of Systematic Reviews, 2017 (11): CD011135. https://doi.org/10.1002/14651858.CD011135.pub2.
Pega, Frank, Roman Pabayo, Claire Benny, Eun-Young Lee, Stefan K. Lhachimi, and Sze Yan Liu. 2022. “Unconditional Cash Transfers for Reducing Poverty and Vulnerabilities: Effect on Use of Health Services and Health Outcomes in Low‐ and Middle‐income Countries”. Cochrane Database of Systematic Reviews, 2022 (3). https://doi.org/10.1002/14651858.CD011135.pub3.
Perera, Camila, Shivit Bakrania, Alessandra Ipince, Zahrah Nesbitt-Ahmed, Oluwaseun Obasola, Dominic Richardson, Jorinde Van de Scheur, and Ruichuan Yu. 2022. “Impact of Social Protection on Gender Equality in Low- and Middle-Income Countries: A Systematic Review of Reviews”. Campbell Systematic Reviews 18 (2): e1240. https://doi.org/10.1002/cl2.1240.
Pereznieto, Paola, and Rebecca Holmes. 2023. Gender-Transformative Social Protection in Crisis Contexts: Guidance Note. Social Protection Technical Assistance, Advice and Resource Facility (STAAR), DAI Global UK. https://socialprotection.org/sites/default/files/publications_files/Gender%20transformative%20SP%20guidance%20note_03.10.23.pdf.
Perracini, Monica R., Natalia Arias-Casais, Jotheeswaran A. Thiyagarajan, Colin Rapson, Vivian Isaac, Shahid Ullah, Jang Hyobum, Ritu Sadana, and Zee A. Han. 2022. “A Recommended Package of Long-Term Care Services to Promote Healthy Ageing Based on a WHO Global Expert Consensus Study”. Journal of the American Medical Directors Association 23 (2): 297–303.e14.
Peyron Bista, Céline, and John Carter. 2017. Unemployment Protection: A Good Practices Guide and Training Package – Experiences from ASEAN. ILO. http://www.ilo.org/wcmsp5/groups/public/---asia/---ro-bangkok/documents/publication/wcms_571465.pdf.
Rahman Khandker, Shahidur, Hussain Akhterus Samad, Nobuhiko Fuwa, and Ryotaro Hayashi. 2021. “The Female Secondary Stipend and Assistance Program in Bangladesh: What Did It Accomplish? ” ADB South Asia Working Paper Series, 81. Asian Development Bank. https://www.adb.org/sites/default/files/publication/678776/sawp-081-female-secondary-stipend-assistance-program-bangladesh.pdf.
Rahman, Md Mizanur, Megumi Rosenberg, Gabriela Flores, Nadia Parsell, Shamima Akter, Md Ashraful Alam, Md Mahfuzur Rahman, and Tessa Edejer. 2022. “A Systematic Review and Meta-Analysis of Unmet Needs for Healthcare and Long-Term Care among Older People”. Health Economics Review 12 (1): 60. https://doi.org/10.1186/s13561-022-00398-4.
Ravallion, Martin. 2016. The Economics of Poverty: History, Measurement, and Policy. Oxford: Oxford University Press.
Rawls, John. 1999. A Theory of Justice. Cambridge, MA: Belknap Press.
Razavi, Shahra. 2007. “The Political and Social Economy of Care in a Development Context: Conceptual Issues, Research Questions and Policy Options”. Gender and Development Programme Paper Number 3. UNRISD. https://cdn.unrisd.org/assets/library/papers/pdf-files/razavi-paper.pdf.
———. 2013. “Households, Families, and Social Reproduction”. In The Oxford Handbook of Gender and Politics, edited by Georgina Waylen, Karen Celis, Johanna Kantola, and Laurel Weldon. Oxford: Oxford University Press.
———. 2020. “What Does the UN Have to Say About Family Policy? Reflections on the ILO, UNICEF, and UN Women”. In The Palgrave Handbook of Family Policy, edited by Rense Nieuwenhuis and Wim Van Lancker, 87–115. Cham: Springer International Publishing. https://doi.org/10.1007/978-3-030-54618-2_5.
Razavi, Shahra, Christina Behrendt, Mira Bierbaum, Ian Orton, and Lou Tessier. 2020. “Reinvigorating the Social Contract and Strengthening Social Cohesion: Social Protection Responses to COVID-19”. International Social Security Review 73 (3): 55–80. https://doi.org/10.1111/issr.12245.
Razavi, Shahra, Christina Behrendt, Valeria Nesterenko, Ian Orton, Celine Peyron Bista, Alvaro Ramos Chaves, Helmut Schwarzer, Maya Stern-Plaza, and Veronika Wodsak. 2022. “Building Universal Social Protection Systems for All: What Role for Targeting?” Global Social Policy 22(3): 449–463. https://doi.org/10.1177/14680181221121449.
Razavi, Shahra, and Silke Staab. 2018. “Rethinking Social Policy: A Gender Perspective from the Developing World”. In Handbook on Gender and Social Policy, edited by Sheila Shaver, 74–89. Cheltenham: Edward Elgar.
Richardson, Dominic, David Harris, Sophie Mackinder, and John Hudson. 2023. Too Little, Too Late: An Assessment of Public Spending on Children by Age in 84 Countries. UNICEF Innocenti – Global Office of Research and Foresight. https://www.unicef.org/innocenti/media/2851/file/UNICEF-Too-Little-Too-Late-Report-2023.pdf.
Richterman, Aaron, Christophe Millien, Elizabeth F. Bair, Gregory Jerome, Jean Christophe Dimitri Suffrin, Jere R. Behrman, and Harsha Thirumurthy. 2023. “The Effects of Cash Transfers on Adult and Child Mortality in Low- and Middle-Income Countries”. Nature 618: 575–82. https://doi.org/10.1038/s41586-023-06116-2.
Rodriguez, Zachary. 2022. “The Power of Employment: Effects of India’s Employment Guarantee on Women Empowerment”. World Development 152. https://doi.org/10.1016/j.worlddev.2021.105803.
Salmeron-Gomez, Daylan, Solrun Engilbertsdottir, Jose Antonio Cuesta Leiva, and David Stewart. 2023. “Global Trends in Child Monetary Poverty According to International Poverty Lines”. Policy Research Working Paper 10525. World Bank Group. https://documents1.worldbank.org/curated/en/099835007242399476/pdf/IDU0965118d1098b8048870ac0e0cb5aeb049f98.pdf.
Schjoedt, Rasmus. 2016. “India’s Basic Income Experiment”. Pathways’ Perspectives on Social Policy in International Development, 21.Development Pathways. https://www.developmentpathways.co.uk/publications/india-basic-income-experiment/
Sen, Gita, Veloshnee Govender, and Salma El-Gamal. 2020. “Universal Health Coverage, Gender Equality and Social Protection: A Health Systems Approach”. Discussion Paper 38. UN Women. https://www.unwomen.org/en/digital-library/publications/2020/12/discussion-paper-universal-health-coverage-gender-equality-and-social-protection.
Sengupta, Anasuya. 2019. “All Work and No Pay: The Invisibilisation of Women’s Labour in Public Works Programmes”. Development Pathways (blog). 8 March 2019. https://www.developmentpathways.co.uk/blog/all-work-and-no-pay-the-invisibilisation-of-womens-labour-in-public-works-programmes/.
Sepúlveda, Magdalena, and Carly Nyst. 2012. The Human Rights Approach to Social Protection.Helsinki: Ministry for Foreign Affairs of Finland. https://www.ohchr.org/sites/default/files/Documents/Issues/EPoverty/HumanRightsApproachToSocialProtection.pdf.
Silverio, Sergio A., Nila Varman, Zenab Barry, Nina Khazaezadeh, Daghni Rajasingam, Laura A. Magee, and Jacqueline Matthew. 2023. “Inside the ‘Imperfect Mosaic ’: Minority Ethnic Women’s Qualitative Experiences of Race and Ethnicity during Pregnancy, Childbirth, and Maternity Care in the United Kingdom”. BMC Public Health 23 (1). https://doi.org/10.1186/s12889-023-17505-7.
Soares, Fabio, and Ian Orton. 2017. “Debating Graduation”. Policy in Focus 14 (2). International Policy Centre for Inclusive Growth. https://ipcig.org/pub/eng/PIF39_Debating_Graduation.pdf.
South Africa, The Presidency. 2023. Building a Society That Works: A Million Jobs, Opportunities and More. Presidential Employment Stimulus Update, February 2023. https://pres-employment.openup.org.za/img/Presidential%20Employment%20Stimulus%20Update%20February%202023.pdf.
Spasova, Slavina, Dalila Ghailani, Sebastiano Sabato, Stéphanie Coster, Boris Fronteddu, and Bart Vanhercke. 2021. Non-Standard Workers and the Self-Employed in the EU: Social Protection during the COVID-19 Pandemic. Report 2021.02. Brussels: European Social Observatory and European Trade Union Institute. https://etui.org/publications/non-standard-workers-and-self-employed-eu.
SPIAC-B. 2022. Strengthen Linkages Between Humanitarian Assistance and National Social Protection Systems for Effective Responses to Forced Displacements. https://www.social-protection.org/gimi/Media.action;jsessionid=ZRiLkWKIzD9L2CNERcXol03IQyrsMWaY3YphZPBZ3TGSIXJpwAbs!1945465934?id=18878.
Staab, Silke. 2019. “Early Childhood Education and Care from a Gender Perspective”. In Early Childhood and Development Work, edited by Anne Trine Kjørholt and Helen Penn, 69–89. London: Palgrave Macmillan. https://www.palgrave.com/gp/book/9783319913186.
Staab, Silke, and Constanza Tabbush. 2022. “Following a Moving Target on a Global Scale: Gender Data Collection during COVID-19”. Global Social Policy 22 (1): 184–89. https://doi.org/10.1177/14680181221079088.
Standing, Guy. 2009. Work after Globalization: Building Occupational Citizenship. Northampton: Edward Elgar. https://www.e-elgar.com/shop/gbp/work-after-globalization-9781848441644.html.
———. 2011. The Precariat: The New Dangerous Class. London: Bloomsbury Academic.
Standing, Guy, and Ian Orton. 2018. “Development and Basic Income: An Emerging Economic Model”. In The Ins and Outs of Inclusive Finance: Some Lessons from Microfinance and Basic Income, edited by Diana Barrowclough, 59–103. UNCTAD (United Nations Conference on Trade and Development). https://unctad.org/en/PublicationsLibrary/gdsmdp2017d3_en.pdf.
Temmerman, Marleen, Rajat Khosla, and Lale Say. 2014. “Sexual and Reproductive Health and Rights: A Global Development, Health, and Human Rights Priority”. The Lancet 384 (9941): e30–31.
Tessier, Lou, Nathalie De Wulf, and Yuta Momose. 2022a. “Long-Term Care in the Context of Population Ageing: A Rights-Based Approach to Universal Coverage”. ILO Working Paper 82. https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---soc_sec/documents/publication/wcms_858784.pdf.
———. 2022b. “Long-Term Care in the Context of Population Ageing: What Role for Social Protection Policies?” International Social Security Review 75 (3–4): 19–45. https://doi.org/10.1111/issr.12306.
Tessier, Lou, Maya Stern Plaza, Christina Behrendt, Florence Bonnet, and Emmanuelle St-Pierre Guilbault. 2013. “Social Protection Floors and Gender Equality: A Brief Overview”. ESS Working Paper 37. http://www.social-protection.org/gimi/gess/RessourceDownload.action?ressource.ressourceId=39137.
Torry, Malcolm. 2015. 101 Reasons for a Citizen’s Income: Arguments for Giving Everyone Some Money. Bristol: Policy Press. https://policy.bristoluniversitypress.co.uk/101-reasons-for-a-citizens-income.
UN (United Nations). 2018. Realization of the Sustainable Development Goals by, for and with Persons with Disabilities: UN Flagship Report on Disability and Development 2018 (advance unedited version). https://reliefweb.int/attachments/fcb51103-4646-304f-a7a4-ac0da2fcfe76/UN-Flagship-Report-Disability.pdf.
———. 2019. Disability and Development Report 2018: Realizing the Sustainable Development Goals by, for and with Persons with Disabilities. https://social.un.org/publications/UN-Flagship-Report-Disability-Final.pdf.
———. 2022.Visit to Lebanon: Report of the Special Rapporteur on Extreme Poverty and Human Rights, Olivier De Schutter. A/HRC/50/38/Add.1. https://documents-dds-ny.un.org/doc/UNDOC/GEN/G22/306/19/PDF/G2230619.pdf?OpenElement.
———. 2023. Women and Peace and Security: Report of the Secretary-General. S/2023/725. https://documents-dds-ny.un.org/doc/UNDOC/GEN/N23/279/08/PDF/N2327908.pdf?OpenElement.
UN Women. 2015a. Gender Equality, Child Development and Job Creation: How to Reap the ‘Triple Dividend’ from Early Childhood Education and Care Services. https://www.unwomen.org/sites/default/files/Headquarters/Attachments/Sections/Library/Publications/2015/UNwomen-PolicyBrief02-GenderEqualityChildDevelopmentAndJobCreation-en.pdf.
———. 2015b. Progress of the World’s Women 2015-2016: Transforming Economies, Realizing Rights. https://www.unwomen.org/en/digital-library/publications/2015/4/progress-of-the-worlds-women-2015.
———. 2017a. Long-Term Care for Older People: A New Global Gender Priority. https://www.unwomen.org/en/digital-library/publications/2017/12/long-term-care-for-older-people.
———. 2017b. Progress of Women in Latin America and the Caribbean 2017: Transforming Economies, Realizing Rights. https://lac.unwomen.org/sites/default/files/Field%20Office%20Americas/Documentos/Publicaciones/2017/07/UNW16017_Executive_Summary_Web_ENG.pdf.
———. 2018. Turning Promises into Action: Gender Equality in the 2030 Agenda for Sustainable Development.
———. 2019a. Progress of the World’s Women 2019–2020: Families in a Changing World. https://www.unwomen.org/sites/default/files/Headquarters/Attachments/Sections/Library/Publications/2019/Progress-of-the-worlds-women-2019-2020-en.pdf.
———. 2019b. World Survey on the Role of Women in Development: Report of the Secretary-General (2019): Why Addressing Women’s Income and Time Poverty Matters for Sustainable Development. https://www.unwomen.org/en/digital-library/publications/2019/06/world-survey-on-the-role-of-women-in-development-2019.
———. 2020a. Leaving No One behind: Access to Social Protection for All Migrant Women. https://migrationnetwork.un.org/resources/leaving-no-one-behind-access-social-protection-all-migrant-women.
———. 2020b. Whose Time to Care? Unpaid Care and Domestic Work during COVID-19. https://data.unwomen.org/sites/default/files/inline-files/Whose-time-to-care-brief_0.pdf
———. 2021a. Beyond COVID-19: A Feminist Plan for Sustainability and Social Justice. https://www.unwomen.org/en/digital-library/publications/2021/09/beyond-covid-19-a-feminist-plan-for-sustainability-and-social-justice.
———. 2021b. Putting Gender Equality at the Centre of Social Protection Strategies in Sub-Saharan Africa: How Far Have We Come? https://www.unwomen.org/sites/default/files/2021-12/Policy-brief-Putting-gender-equality-at-the-centre-of-social-protection-strategies-in-sub-Saharan-Africa-en.pdf.
———. 2023a. Addressing Violence against Women through Social Protection: A Review of the Evidence. https://www.unwomen.org/en/digital-library/publications/2023/03/policy-brief-addressing-violence-against-women-through-social-protection.
———. 2023b. Social Norms, Gender and Development: A Review of Research and Practice. https://www.unwomen.org/en/digital-library/publications/2023/10/discussion-paper-social-norms-gender-and-development-a-review-of-research-and-practice.
UN Women and UN DESA. 2021. Progress on the Sustainable Development Goals: The Gender Snapshot 2021. https://www.unwomen.org/sites/default/files/Headquarters/Attachments/Sections/Library/Publications/2021/Progress-on-the-Sustainable-Development-Goals-The-gender-snapshot-2021-en.pdf.
UN Women and UNDP (United Nations Development Programme). 2022. Government Responses to COVID-19: Lessons on Gender Equality for a World in Turmoil. https://www.unwomen.org/sites/default/files/2022-06/Government-responses-to-COVID-19-Lessons-on-gender-equality-for-a-world-in-turmoil-en.pdf.
UN Women and World Bank. 2018. Gender Differences in Poverty and Household Composition Through the Life Cycle. https://www.unwomen.org/sites/default/files/Headquarters/Attachments/Sections/Library/Publications/2018/SDG-report-Spotlight-01-Gender-differences-in-poverty-and-household-composition-en.pdf.
UNDP (United Nations Development Programme). 2021. Informality and Social Protection in African Countries: A Forward-Looking Assessment of Contributory Schemes. https://www.undp.org/africa/publications/informality-and-social-protection-african-countries-forward-looking-assessment-contributory-schemes.
———. 2022. Human Development Report 2021-22: Uncertain Times, Unsettled Lives – Shaping our Future in a Transforming World. https://hdr.undp.org/content/human-development-report-2021-22
UNDP and UN Women. 2020. “COVID-19 Global Gender Response Tracker Fact Sheets” (various titles). Global Factsheet. https://www.undp.org/content/undp/en/home/librarypage/womens-empowerment/COVID-19-Global-Gender-Response-Tracker.html.
———. 2021. “COVID-19 Global Gender Response Tracker”. UNDP COVID-19 Data Futures Platform (blog), March 2021. https://data.undp.org/gendertracker/.
UNICEF. 2020. Social Protection and Its Effects on Gender Equality: A Literature Review. Florence: UNICEF Office of Research – Innocenti. https://www.un-ilibrary.org/content/papers/10.18356/25206796-2020-16/read.
———. 2021. Preventing a Lost Decade: Urgent Action to Reverse the Devastating Impact of COVID-19 on Children and Young People. https://www.unicef.org/media/112891/file/UNICEF%2075%20report.pdf.
UNICEF and Learning for Well-Being Institute. 2024. Proven Solutions for Children: Accelerating Progress towards the Sustainable Development Goals and Beyond. https://www.unicef.org/media/162436/file/UNICEF%20Proven%20solutions%20SDGs%2022092024.pdf.pdf.
United Kingdom, Government of. n.d “Statutory Guidance: Early Education and Childcare”. https://www.gov.uk/government/publications/early-education-and-childcare--2/early-education-and-childcare-applies-from-1-april-2024.
United Kingdom, Government of. 2022. Modern Slavery: Statutory Guidance for England and Wales (under S49 of the Modern Slavery Act 2015) and Non-Statutory Guidance for Scotland and Northern Ireland. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1087550/Modern_Slavery_Statutory_Guidance__EW__Non-Statutory_Guidance__SNI__v2.10__FINAL_.pdf.
Vos, Theo, Stephen S. Lim, Cristiana Abbafati, Kaja M. Abbas, Mohammad Abbasi, Mitra Abbasifard, Mohsen Abbasi-Kangevari, Hedayat Abbastabar, Foad Abd-Allah, and Ahmed Abdelalim. 2020. “Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019”. The Lancet 396 (10258): 1204–22.
Waidler, Jennifer, and Maja Gavrilovic. 2020. “From Crisis Comes Opportunity: Spain’s Basic Income Response to COVID-19”. Evidence for Action, 1 July.Florence: UNICEF Office of Research -– Innocenti.
Walker, Robert. 2014. The Shame of Poverty: Global Perspectives. Oxford: Oxford University Press.
Walker, Ruth, Deborah Turnbull, and Chris Wilkinson. 2002. “Strategies to Address Global Cesarean Section Rates: A Review of the Evidence”. Birth 29 (1): 28–39. https://doi.org/10.1046/j.1523-536X.2002.00153.x.
Walker, Wendy M., and Meredith Wyse. 2021. “Leadership and Governance of Long-Term Care Systems in Asia and the Pacific”. ADB briefs No. 198. https://www.adb.org/sites/default/files/publication/751896/adb-brief-198-long-term-care-systems-lessons-asia-pacific.pdf
Watts, Beth, and Suzanne Fitzpatrick. 2018. Welfare Conditionality. New York; London: Routledge. https://www.routledge.com/Welfare-Conditionality/Watts-Fitzpatrick/p/book/9781138119918.
WHO (World Health Organization). 1978. Declaration of Alma-Ata. Copenhagen: World Health Organization. Regional Office for Europe.
———. 2009. Women and Health: Today’s Evidence: Tomorrow’s Agenda. https://screening.iarc.fr/doc/Womenandhealthreport.pdf.
———. 2015. World Report on Ageing and Health.
———. 2019a. Delivered by Women, Led by Men: A Gender and Equity Analysis of the Global Health and Social Workforce. Geneva: https://apps.who.int/iris/bitstream/handle/10665/311322/9789241515467-eng.pdf.
———. 2019b. Primary Health Care on the Road to Universal Health Coverage: 2019 Global Monitoring Report. https://www.who.int/docs/default-source/documents/2019-uhc-report-executive-summary.
———. 2021. Decade of Healthy Ageing: Baseline Report. https://www.who.int/publications-detail-redirect/9789240017900.
———. 2022a. Guide for Integration of Perinatal Mental Health in Maternal and Child Health Services. https://www.who.int/publications/i/item/9789240057142.
———. 2022b. World Health Statistics 2022: Monitoring Health for the SDGs. https://www.who.int/publications/i/item/9789240051157.
———. n.d. “International Classification of Functioning, Disability and Health (ICF)”. https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health
———. Forthcoming. Reducing the Socio-Economic Burden of Public Health and Social Measures on Households during the COVID-19 Pandemic: Landscape of the Evidence on the Role of Social Protection Policies and Programmes.
WHO and PAHO (Pan American Health Organization). 2021. Out-of-Pocket Expenditure in Health: The Need for a Gender Analysis’. https://iris.paho.org/bitstream/handle/10665.2/54670/9789275123546_eng.pdf?sequence=1&isAllowed=y.
WHO, and World Bank. 2023. Tracking Universal Health Coverage: 2023 Global Monitoring Report. https://www.who.int/publications/i/item/9789240080379.
Williams, Loui. 2021. “Universal Basic Income: Potential and Limitations from a Gender Perspective”. Policy Brief 22. UN Women. https://www.unwomen.org/sites/default/files/Headquarters/Attachments/Sections/Library/Publications/2021/Policy-brief-Universal-basic-income-en.pdf.
Yang, Lichao, Robert Walker, Jiexuan Chen, and Rui Zhang. 2019. Universal Child Benefits and Dignity and Shame. UNICEF.
Acknowledgements
Data analysis and preparation of figures was done by Valeria Nesterenko and Isabella Kopp.
Contributions and comments were also received from the following (in alphabetical order): Laura Addati (ILO), Salma Awad Elgamal (ILO), Mira Bierbaum (formerly ILO, now UNICEF), Umberto Cattaneo (ILO), Valeria Esquivel (ILO), Chidi King (ILO), Kroum Markov (ILO), Valeria Nesterenko (ILO), Silke Staab (UN Women), Maya Stern Plaza (ILO), Loui Williams (UN Women) and Zhiming Yu (ILO).

