
Nursing and Artificial Intelligence in the Republic of Korea
Abstract
This paper examines the gap between what nurses need and what actually gets built, through: 1) a three-month ethnographic study at Mirae Hospital (MH) in South Korea—which combined interviews and ward observations—and 2) participatory design workshops with nurses from MH and unionized hospitals. Our findings reveal three patterns: first, AI systems succeed when addressing acknowledged problems through collaborative design; second, they fail when attempting to model volitional human behavior or assuming laboratory conditions that clinical environments lack; and third, high-impact automations requested by nurses can be overshadowed and receive less institutional priority, as technically sophisticated investments tend to garner more structural support. We further found that AI adoption differs across institutions, highlighting union representation as a meaningful asset for bringing nurses’ perspectives to the forefront of technology implementation. Together, these findings suggest how current participatory processes shape whose voices most influence AI design, with bedside nurses—those most directly affected—often having less direct input than other stakeholder groups. Addressing these shortcomings requires not only better design methods, but institutional reform in how technology priorities are set and whose needs are treated as authoritative.
Introduction1
Artificial intelligence (AI) promises to transform healthcare by enhancing diagnostic accuracy, streamlining workflows, and reducing clinician burden [1, 2]. Hospitals worldwide are investing heavily in predictive analytics, clinical decision support systems, and computer vision applications. Yet a tension emerges when we examine these deployments from the perspective of frontline healthcare workers: why do some automation efforts succeed while others fail, and why do persistent gaps remain between what nurses need to do their jobs effectively and what actually gets built?
This paper investigates the tension using two different approaches: 1) We conducted a three-month ethnographic study at Mirae Hospital (MH)1, a large academic tertiary hospital in South Korea. The ethnographic study includes semi-structured interviews with 17 participants across organizational roles, 60 hours of ward observation. 2) We also performed participatory design workshops with nurses and hospital staff from both MH and unionized hospitals. Through these two approaches, we examine how AI and automation technologies are reshaping nursing work, whose voices shape which technologies get developed, and what ideal AI systems nurses envision.
Our findings reveal a systematic pattern. Technologies that succeeded – like an automated logistics robot for ward supply management (hereafter, the logistics robot) and RTLS (real-time location system) equipment tracking – solved problems that both management and bedside nurses acknowledged, emerged through extended collaborative design processes, and eliminated work without requiring nurses or patients to change their behavior. Technologies that failed – like fall prediction algorithms and pressure ulcer imaging apps – attempted to calculate inherently volitional human behaviors or assumed laboratory conditions in messy clinical reality. Notably, however, a significant finding emerged regarding the solutions that were not developed: simple, high-impact automation like tablet-based patient education that nurses explicitly and repeatedly requested, but that lacked either the technical sophistication or institutional alignment to attract investment.
These findings point to two interrelated problems in how AI gets developed for healthcare settings. First, a technology-first orientation drives investment toward systems aligned with institutional priorities—such as cutting-edge algorithmic systems or operational efficiencies that support broader institutional goals. Second, current processes for planning and implementing technology that claim to incorporate “the field” tend to give more weight to certain voices—such as charge nurses, ward managers, innovation teams—while bedside nurses who interact with these systems daily often have fewer opportunities to provide input.
This paper makes three contributions. First, we provide nurses’ articulated visions for ideal AI systems, drawing on participatory design workshops alongside ethnographic documentation of actual technology deployments. Second, we identify the conditions that distinguish successful automation from failure, showing how the gap between “technology-first” and “need-first” approaches shapes outcomes. Third, we reveal how differential definitions of “the field” in technology development and implementation processes systematically exclude certain voices, with consequences for what gets built and what remains unaddressed. Together, these contributions offer guidance for more effective approaches to healthcare AI development.
Background
The background provides an overall description of AI systems in healthcare both within and outside South Korea. This is more about the background information of average Korean nursing situations that motivate our project rather than describing our field sites.
AI and Automation in Healthcare: Promise and Implementation Gaps
Research on AI in healthcare has expanded rapidly, with applications ranging from diagnostic imaging to clinical decision support to administrative automation [3, 4]. Systematic reviews consistently identify potential benefits: improved efficiency, enhanced patient safety, reduced cognitive burden, and more personalized care [5, 6]. Within nursing specifically, AI applications have targeted early disease detection, workflow optimization, patient monitoring, and documentation support [1, 7].
Yet a gap persists between technological promise and implementation reality. The vast majority of published research focuses on technology development and testing phases rather than actual deployment [5], leaving limited evidence about how these systems perform in clinical practice. Studies that do examine implementation reveal recurring challenges: poor fit with existing workflows, lack of trust among clinicians, inadequate training, and systems designed without meaningful input from end users [3, 8]. There is also limited evidence on how these systems actually impact the working conditions of nurses – in terms of working time, workload, occupational safety and health, skills and training, and scope of work – a gap that our study begins to address through direct ethnographic observation of deployment contexts. Notably, research on collaborative robots in nursing found that most systems were designed as patient-centered rather than nurse-centered – prioritizing visible interaction with patients or demonstrating technological sophistication to funders and administrators – with few explicitly targeting nursing workload reduction [8].
This implementation gap raises questions about whose perspectives drive AI development in healthcare. While nurses represent the largest healthcare workforce and serve as primary users of many clinical technologies, studies consistently find they are underrepresented in AI research and development processes [5, 9]. The Nursing and Artificial Intelligence Leadership Collaborative identified this as a priority concern: “Nurses must be meaningfully involved in all stages of AI: from development to implementation” [9, p.3708]. Our study contributes empirical evidence about what happens when this involvement remains superficial.
Nursing Work and the Coordination Burden
The International Council of Nurses (ICN), in its landmark 2025 revised definition, characterizes nursing as “a profession dedicated to upholding everyone’s right to enjoy the highest attainable standard of health, through a shared commitment to providing collaborative, culturally safe, people-centred care and services,” whose practice is “underpinned by a unique combination of science-based disciplinary knowledge, technical capability, ethical standards, and therapeutic relationships” [10]. Crucially, the definition recognizes that nurses “work autonomously and collaboratively across settings” and “lead, educate, research, advocate, innovate and shape policy to improve health outcomes” – a scope of practice that extends far beyond bedside task execution. This expansive, multidimensional conception of nursing work has direct implications for how AI systems should be designed: technologies that address only narrow, visible tasks risk missing the coordinative, relational, and advocacy dimensions that constitute much of what nurses actually do.
Central to this scope is the coordinative dimension of nursing work. Nurses function not simply as direct care providers but as the ‘hub’ coordinating [11, p. 727] across organizational boundaries that rarely intersect otherwise [12]. A single medication order may require coordination with pharmacy, physicians, patients’ families, and documentation systems. A patient transfer involves synchronizing operating rooms, transport services, family communication, and handoff documentation. This coordination work – what scholars have termed “articulation work”[13] or “artful coordinating”[11] – requires nurses to flexibly navigate formal procedures, local context, and situated contingencies in ways essential to hospital functioning yet often unrecognized in institutional metrics.
The coordination burden has consequences for technology development and evaluation. Technologies that eliminate coordination work may generate relief disproportionate to their objective time savings, because they reduce cognitive overhead that institutional metrics never captured. Conversely, technologies that add new coordination demands – requiring verification with multiple sources, generating alerts that must be reconciled with clinical judgment – create friction beyond their immediate task burden. Understanding these dynamics helps explain why nurses may enthusiastically embrace a logistics robot while resisting a sophisticated prediction algorithm: the former eliminates coordination, while the latter adds it.
Institutional Logics of Technology Investment
Healthcare technology adoption is shaped not only by clinical utility but by institutional priorities that may diverge from frontline needs. Hospitals operate within complex economic constraints where technology investments must be justified through multiple logics: clinical improvement, operational efficiency, regulatory compliance, and competitive positioning [14]. These institutional logics can align with or diverge from frontline worker needs in unpredictable ways. A logistics robot system might be adopted because it frees valuable floor space – previously occupied by supply storage – for revenue-generating clinical services such as imaging or procedure rooms, while simultaneously reducing nursing burden. In such cases, institutional and frontline interests converge, facilitating successful adoption. However, predictive analytics systems showcased at international conferences may attract investment based on their contribution to institutional prestige and research output, regardless of whether they address problems that frontline workers recognize as priorities – or whether they may in fact add to the workload of nurses rather than reduce it.
This dynamic suggests that understanding technology adoption requires attending to the multiple stakeholders whose interests shape investment decisions. What appears from one perspective as “technology-first” development may reflect legitimate institutional concerns; what appears from another as “need-first” design may overlook operational constraints. Our study examines how these tensions play out in practice, documenting both successful alignments and persistent mismatches.
Technology Development Processes and the Question of Whose Voice Counts
Participatory design (PD) approaches have been increasingly advocated for healthcare AI development, with the premise that involving end users produces better-fitting, more adoptable technologies [8]. In healthcare contexts, PD faces distinctive challenges: time-constrained clinicians, complex organizational hierarchies, distributed decision-making across professional groups, and tensions between institutional and individual priorities. Critical scholarship on PD has examined how participatory processes can reproduce rather than challenge existing power relations [15]. When organizations claim to involve “the field” in technology development, the question of who counts as representative of that field becomes consequential. Ward manager nurses may understand aggregate workflow problems differently than bedside nurses experiencing moment-to-moment task demands. Innovation teams positioned between clinical operations and technology development occupy yet another perspective. These differential positions shape not only what problems get identified but what solutions appear feasible or desirable.
Our study contributes empirical evidence about how these dynamics play out in healthcare AI development. We document cases where “field input” was successfully gathered yet bedside nurses experienced resulting technologies as, in one nurse’s words, appearing “one day...just there in the ward.” This tension between participatory rhetoric and exclusionary outcomes reveals how the boundaries of participation are drawn and whose experiences become authoritative in shaping technological futures.
Nursing Work in South Korea
South Korea provides a particularly salient context for examining healthcare AI adoption given the intensity of nursing workload and the severity of workforce challenges. Korean nurses manage patient loads two to three times higher than their counterparts in the United States and other OECD countries [16, 17]. In general hospital wards, a single nurse may be responsible for 40-50 patients across multiple rooms during a single shift [18, 19]. These workload conditions contribute to a nursing workforce crisis. According to the Korean Hospital Nurses Association’s annual surveys (2013-2022), nurse turnover rates have remained persistently high at 13-15% per year, with 2022 reaching 15.8% [20]. More alarming is the trajectory for new nurses: turnover within the first year rose from 38.1% in 2017 to 52.8% in 2022, meaning more than half of newly hired nurses leave their positions within twelve months. The primary reasons cited include work maladjustment, transfer to other hospitals, and career changes out of nursing entirely. National working conditions data corroborate these pressures. Korea’s 7th Working Environment Survey [21] found that workers in healthcare and social welfare had the lowest rate of any industry of being able to attend to personal matters during working hours – only 18.2%, compared to a national average of 34.9% – reflecting the relentless, uninterruptible pace of clinical work. Upper limb musculoskeletal pain and lower back pain were the most commonly reported occupational health problems nationally (32.3% and 28.5% respectively), consistent with the physically demanding nature of nursing tasks [21].
These trends intersect with broader concerns about the future pipeline of nursing recruits. A recent OECD report drawing on PISA data from over 80 countries found that interest among 15-year-olds in pursuing nursing careers declined in roughly half of OECD countries between 2018 and 2022, with difficult working conditions and relatively low pay identified as key deterrents. The report notes that nursing remains heavily feminized – over 90% of students expressing interest in nursing were girls in 2022 – and disproportionately attractive to those from lower socioeconomic backgrounds, raising equity concerns about future workforce composition. In the Korean context, where working conditions are among the most demanding in the OECD, these pipeline pressures compound existing retention challenges [22].
These statistics reflect broader structural issues. Of the approximately 481,000 licensed nurses in Korea, only 52.8% (254,227) work in clinical settings – among the lowest rates in OECD countries, where the average is 68.2% [23]. Many of the remaining nurses work outside hospital settings entirely, as health managers in corporations, school nurses, occupational health staff, or private caregiving aides – roles that draw licensed professionals away from the acute care settings where shortages are most severe. An estimated 12,000 nurses leave hospital employment annually, contributing to chronic understaffing that intensifies workload for those who remain. The Korean government has responded with various policy initiatives, including the establishment of a Nursing Policy Division within the Ministry of Health and Welfare (2021) and ongoing debates around nursing legislation. However, fundamental improvements in nurse-to-patient ratios have proven difficult to achieve.
This context shapes how nurses experience automation. Technologies that genuinely reduce workload or coordination burden address urgent, widely felt problems. Yet the same resource constraints that make workload reduction valuable also limit nurses’ capacity to participate in design processes or advocate for their priorities. The steep hierarchies between nurses and physicians – compounded by the documented culture of workplace bullying known as “Taeoom”2 – also limit nurses’ participation in the design process.
Mirae Hospital (MH)3, represents a resource-rich end of the hospital spectrum in South Korea. The institution has access to in-house software engineering capabilities, enabling rapid prototyping and deployment of novel systems. It has invested substantially in custom-developed clinical information systems and automation, including logistics robots, equipment tracking, and clinical decision support.
While our findings emerge from this specific institutional context, the dynamics we identify – technology-first investment priorities, differential inclusion in participatory processes, gaps between expressed needs and implemented solutions – reflect challenges documented across healthcare systems internationally [5, 8]. Our findings thus offer insights relevant beyond the Korean context while remaining attentive to how local conditions intensify and shape these broader patterns.
Methods: Site, Participants, and the Social Organization of Ward Work
We collected data from July to October 2025 to understand how AI and automation are reshaping nursing work and how nurses envision their ideal AI systems for the future. Our methods combined: 1) ethnographic fieldwork at MH – including interviews and observations – and 2) participatory design workshops involving union representatives from the Korean Health and Medical Workers’ Union (KHMU) as well as nurses from MH.
Ethnographic observation
Methods
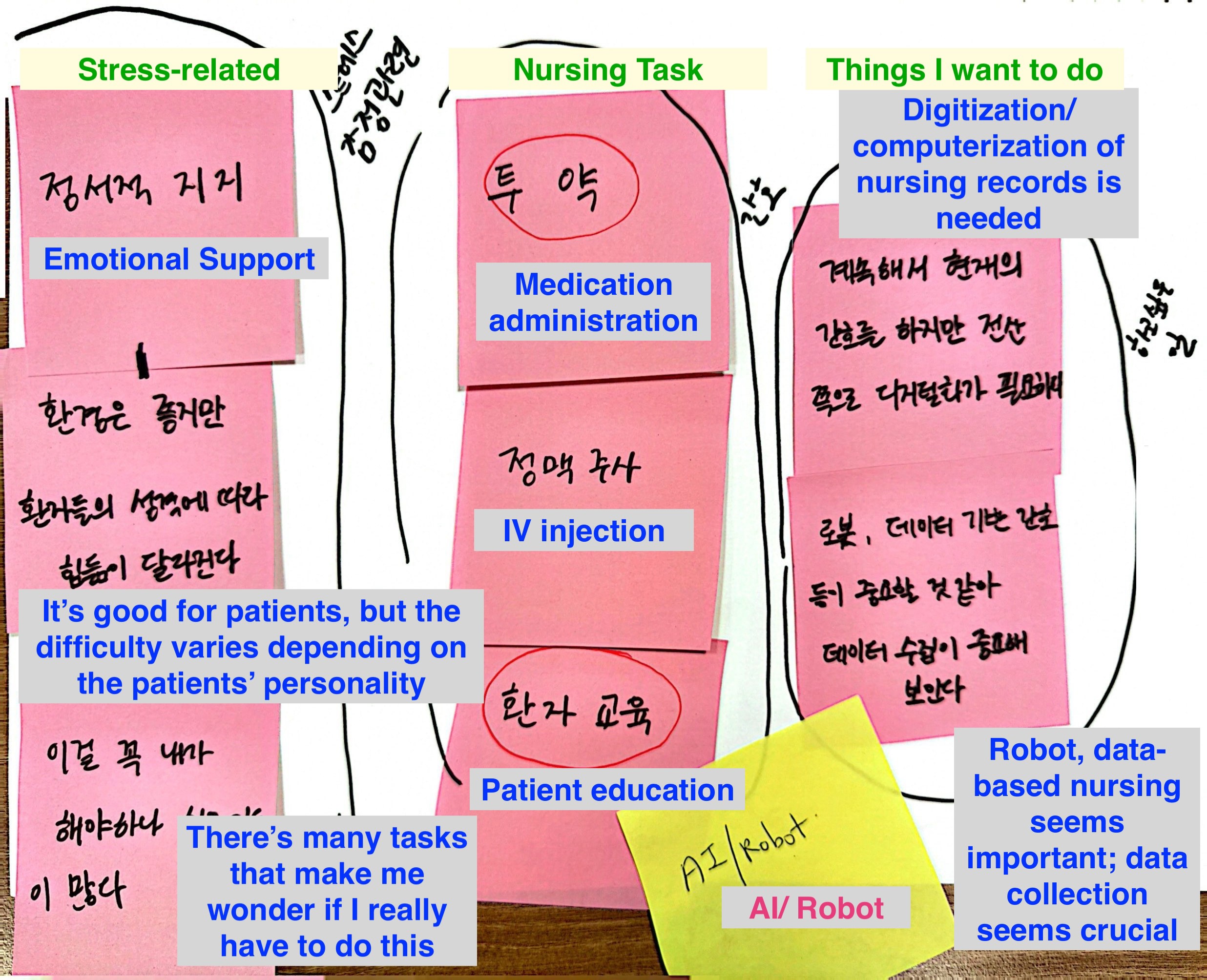
Figure 1: Results from collaborative mapping during individual interviews
Background Information
The technologies we examine were deployed at varying scales across the hospital. The automated logistics robot system – which features an Autonomous Mobile Robot (AMR) as a base platform (similar to Figure 2, left) and a conventional medical material cabinet on top (similar to Figure 2, right) – operated hospital-wide, delivering supplies to all general wards. BPOC (barcode point-of-care medication verification) had achieved near-universal adoption after several years of implementation. RTLS (real-time location system) equipment tracking covered high-turnover mobile devices like infusion pumps and vital signs monitors. Clinical decision support systems (or CDSS) for fall and pressure ulcer risk prediction were embedded in the electronic health record, generating daily alerts that nurses reviewed during morning assessments. The pressure ulcer imaging application existed as an optional mobile tool available to all nursing staff but used inconsistently.
Figure 2: The automated logistics robot system deployed at MH features an Autonomous Mobile Robot (AMR) base platform (similar to the example on the left) topped by a conventional medical supply cabinet (similar to the example in the middle). The AMR and the cabinet are integrated in a manner similar to the blue AMR and yellow shelf assembly utilized in the Amazon logistics system on the right. To protect the anonymity of the field site, sample components are shown here in place of the actual system.

Our observations of the nursing station revealed the spatial organization of this multi-actor convergence. The station sits at the center of each ward, surrounded by patient rooms extending down two parallel corridors. Rather than being enclosed, the station features a counter-height barrier that makes nurses visible to anyone approaching. Behind this counter, nurses prepare medications in the attached pharmacy room, document care in the electronic system, and coordinate with other departments by phone. The counter’s openness – designed to make nurses accessible – creates what one participant called a “glass wall” situation: nurses can be seen working, and anyone can interrupt.
During a typical two-hour observation period at a surgical ward nursing station, we counted more than twenty interruptions to the three nurses working there. Family members asked where to pay hospital bills (redirected to admissions). A patient wanted a different size hospital gown (nurse retrieved from supply room). Someone returned meal trays 30 minutes late and asked if this was acceptable (nurse confirmed it was fine). A physician asked about a patient’s morning lab results (nurse looked up in system, relayed values). These requests were individually small but cumulatively fragmenting. Nurses described this constant context-switching as preventing sustained focus on tasks requiring careful attention – medication preparation, care planning, documentation review. As one of the nurses (P5) articulated : “Every small interaction demands mental energy... like I’m giving away bits of myself with each one, scattering my attention across all these little moments.”
A medication order requires coordinating with the pharmacy (to confirm availability and preparation), the physician (to clarify ambiguous dosing), sometimes the patient’s family (to explain purpose and obtain consent), and finally documentation in the electronic record (to maintain legal continuity). A patient scheduled for surgery requires coordination with the operating room (to confirm timing), transport services (to arrange movement),the patient’s family (to inform them of timing and location), and the receiving surgical team (to hand off current status). A discharged patient’s family calls with questions about wound care, requiring the nurse to locate the discharge summary, contact the relevant physician for clarification, and call the family back with instructions – none of which is counted as direct patient care in productivity metrics.
Nurses described that, prior to the introduction of automated logistics and equipment-tracking systems, they commonly arrived 60-90 minutes before their official shift to search for mobile equipment, review patient charts, and prepare for anticipated demands. One nurse explained: “We purposely came early because, if you want uninterrupted time to assess your patients, you have no other option.” While these automation systems have significantly reduced the equipment-search burden, the underlying need for uninterrupted cognitive work continues to drive early arrival for many nurses.
This intermediary position – sandwiched between departments, between shifts, between institutional demands and patient needs – shapes how nurses experience automation. Technologies that eliminate coordination work (like the logistics robot removing the need to call other wards to borrow supplies) generate disproportionate relief relative to their objective time savings, because they reduce not just minutes but the cognitive overhead of managing multiple simultaneous requests across organizational boundaries. Conversely, technologies that add new coordination demands (like CDSS alerts requiring verification with multiple sources) create friction beyond their immediate task burden.
Participatory Design Workshops
We facilitated participatory design workshops focused on nurses’ visions of ideal AI system. At MH, 17 nursing staff participated in the workshops, including 14 of our 17 interview participants and three additional MH-affiliated nurses – a ward nurse manager, a nursing assistant, and a senior nurse from the clinical technology evaluation team – who joined the workshops without prior interviews. Workshop exercises invited participants to articulate desired automation and identify gaps between current systems and clinical needs.
Separately, we conducted two participatory design workshops with 10 union-representative nurses from the Korean Health and Medical Workers’ Union (KHMU). Participants included a senior staff member from KHMU’s central office and union branch leaders (branch managers and secretaries) representing nursing locals at six different academic medical centers and one general hospital across the Seoul metropolitan area. These workshops explored collective priorities for technology development across multiple hospital contexts. To protect participants’identities, we do not specify which institutions were represented. Across both settings, participants shared their ideas verbally or through drawings (see Fig. 3).
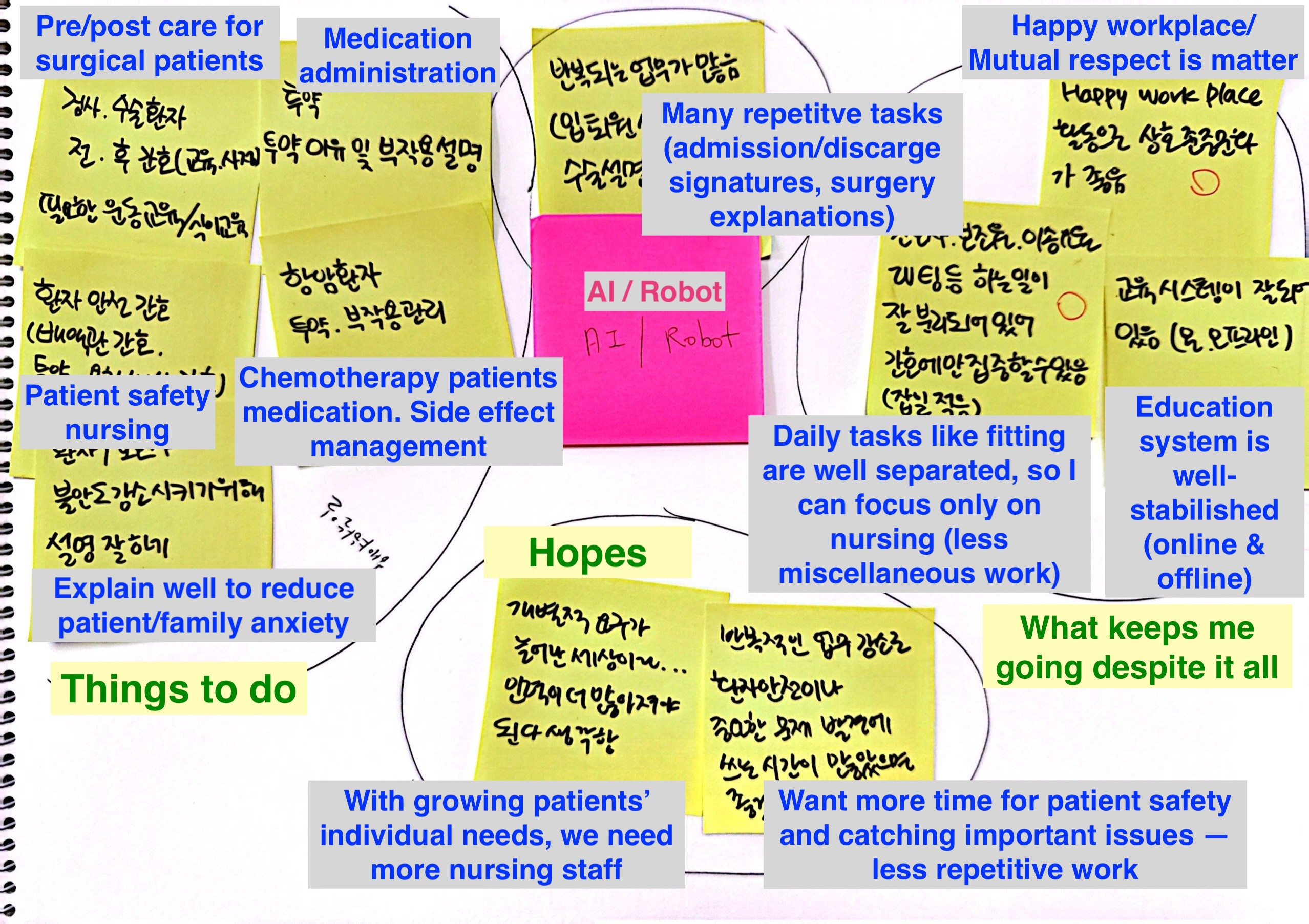
Figure 3: Example ideas created by participants during the design workshops
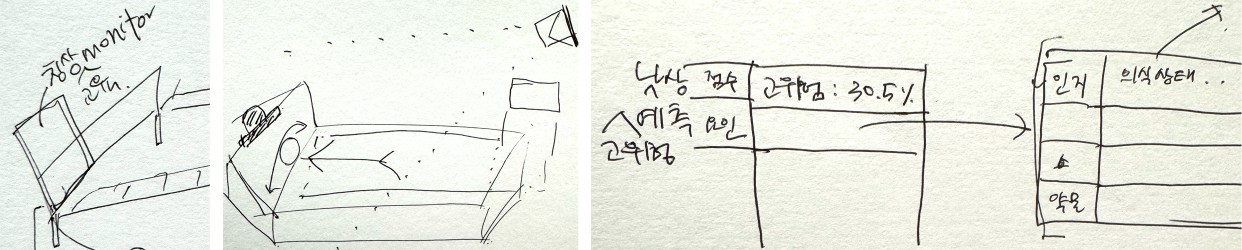
Left: a system for providing patient education (e.g., surgery-related and outpatient education).
Middle: a smart bed that adjusts patient positioning to prevent bedsores.
Right: a refined AI system offering increased transparency in its decision-making; participants also explained their ideas verbally when not using drawings.
Analysis
Our analytical approach was iterative and grounded. We began with open coding of interview transcripts and observation notes, identifying recurring themes around specific technologies, work transformations, and challenges. These initial codes coalesced into broader patterns distinguishing successful adoptions from failures and revealing systematic gaps between deployed systems and expressed needs. Through constant comparison across participants and data sources, our findings organize around two complementary analyses. Part 1 presents nurses’ collective vision of ideal AI systems, synthesized from participatory design workshops, revealing the characteristics that would make automation genuinely supportive rather than burdensome. Part 2 examines three patterns in actual implementations: technologies that succeeded by solving acknowledged problems through collaborative design, technologies that failed by attempting to predict the unpredictable or by assuming clinical realities that didn’t exist, and technologies that nurses explicitly requested but were never implemented. Together, these analyses – what nurses envision, what happened, what failed, and what was missing – provide a comprehensive picture of AI adoption from the perspectives of those who live with these systems daily.
Findings Part 1. Envisioning Ideal AI: What Nurses Want
This section outlines the five types of AI systems that nurses envision as ideal. Data were collected from nurses who are members of the Korean Health and Medical Workers’ Union (KHMU) and affiliated with multiple hospitals across South Korea, as well as from nurses and other AI system stakeholders at MH. Participants from the union are designated as U1, U2, U3, and so forth, while participants from MH are designated as P1, P2, P3, and so on. Consequently, their suggestions do not merely reflect the circumstances of a single hospital, but rather demonstrate broader design ideas identified by participants across various affiliations.
AI Reducing Workload and Saving Time
Nurses in Korea face severe overwork, managing two to three times more beds than nurses in the US [18]. Much of their labour is ‘invisible,’ with no formal measures capturing their workload. Because hospital revenue is driven mostly by doctors’ procedures and visits, nursing labour is often undervalued. Although the KHMU has pushed for regulations setting a maximum number of beds per nurse, implementing such limits has been difficult. To reduce workload, nurses envision AI systems that assist with managerial, physical, and administrative tasks. Reflecting this need, several successful AI solutions have already been deployed in South Korea.
Managerial Work : The nurses recruited from the KHMU reported that their hospitals have used AI interviewers for about five years, largely to cope with high nursing turnover. Heavy workloads contribute to frequent resignations, especially among Generation Z nurses, with some new hires abruptly leaving without notice. As turnover increased, nurse leaders had to conduct interviews much more often – previously twice a year, but now on a rolling basis to fill constant vacancies. Although hospitals attract many applicants, leaders lack the time to review them all, prompting the adoption of AI interviewers. Notably, these systems are used only in hospitals with trade unions. A policy director at KHMU (U1) outlined the reasoning behind the adoption of an AI interviewer in a hospital as follows:
“Because in large hospitals, nurse turnover is extremely high, we have to recruit about twice [as many staff], but the waiting process becomes a huge problem. They open recruitment once a year, and hundreds of people end up waiting. So when we suggested doing rolling recruitment, the senior staff in large hospitals said, ‘Interviewing is going to take forever’. ”
AI interviewers handle the first-round screening, the most time-consuming stage. However, participants expressed concerns about the transparency and quality of AI filtering. They noted instances where strong candidates – vetted during internships – were screened out, leading them to question whether the AI accurately identifies the skill sets nurses value. Furthermore, opaque AI biases could dictate which nursing characteristics are prioritized during hiring. Similar biases in AI-driven interviews have already been documented in other industries [27].
Even so, nurses generally appreciate the time and labour savings. They explained that human-led screening also results in roughly a 10% error rate, and the AI’ s performance appears comparable. Additionally, AI interviewers automatically generate interview archives, allowing leaders to revisit candidate responses whenever needed.
Physical Work : Nurses from both MH and KHMU emphasized that reducing workload is also crucial for physical tasks, such as managing supplies and physically assisting patients. MH has successfully adopted logistics robots – robotic cabinets that store small medical supplies like syringes. Before their introduction, nurses manually tracked daily supply usage, reordered items, and rearranged materials according to the ’first in, first out’ rule by checking individual expiration dates. With logistics robots, this work is largely automated. The carts travel on their own to a parking area, where a third-party logistics company retrieves the cabinet, restocks it off-site, and returns it. From the nurses’ perspective, the supplies come back fully stocked and correctly organized. P5 from the urology unit at MH described how satisfied she is with the logistics robot as follows:
“Before [the logistics robot], we (nurses) had to check everything: the number and quantity of items arriving in the evening, whether they matched the sheet we sent, whether the items arrived properly, and whether we had all the items we needed. But now, the whole process has been fully systematized and delegated to the logistics company. The required quantities are automatically filled in as requested, moving down the line, and we no longer have to perform those checks ourselves. This has significantly reduced our workload.”
Despite the benefits, some nurses expressed concerns about off-site restocking. They questioned whether supplies are managed in hygienic conditions equivalent to hospital standards and noted occasional cases of expired materials being returned. Because automation has reduced their habit of checking expiration dates, they also worried they might accidentally use expired items. They mentioned risks of robots colliding with patients – though robots typically operate at night – and occasional inconvenience when supplies are unavailable while a cart is being transported. Even so, most nurses at MH overwhelmingly appreciated the reduction in tedious manual labour and were generally satisfied with the system.
Nurses recruited through KHMU whose hospitals do not have logistics robots stated a desire for similar automated material-management systems, while those with experience using the carts at MH hoped to expand them to handle additional items, including medications and blood products that are still managed manually. Management also noted that nurses’ positive feedback has motivated expansion of the system.
For other physical tasks, nurses (P11, P12, P16) suggested robotic assistance to help move patients, such as transferring them between beds. These tasks often require more than one person, but busy schedules make it difficult to find help, leading to frequent back and wrist injuries among nurses.
Nurses also hoped to reduce time spent tracking patients’ intake and output (P5, P14, U4, U9). For example, pediatric nurses currently must weigh every diaper before and after use, because even small weight differences matter for premature infants. An automated system that weighs and records diapers would save significant time. Similarly, nurses imagined AI tools that could more reliably track intake and output for adult patients. Although patients and family caregivers sometimes help with this task, nurses remain responsible for monitoring accuracy, making it a persistent workload burden. Despite the participants’ desire for an automated intake–output tracking system, MH leadership noted that a previous attempt to deploy smart food trays was unsuccessful due to high error rates. Because this was a past initiative, the nursing staff – excluding leadership – remained unaware of the trial’s failure.
Office Work : All participants hoped to reduce workload related to administrative tasks, such as managing documents. MH has been pilot-testing an AI dictation system that generates text based on nurses’ conversations with patients, helping them spend less time entering information into the Electronic Medical Record (EMR) system. According to leadership (P20), nurses are generally positive about the tool. Although it does not produce complete documents, it provides a solid draft that nurses can copy, paste, and edit.
Nurses also imagined AI tools that could draft patient consent forms (P5, P8), analyze medical records from other hospitals (U6, U7), or assist with preparing handover documents during shift changes (P8, P16). Shift-change hours are not always treated as official work time, so nurses sometimes skip meals to complete handover documentation. They envisioned AI acting as a mediator that retrieves key information from the outgoing nurse and delivers it to the incoming nurse, easing the burden of this critical but time-pressured task.
AI Addressing Interpersonal Issues
All nurse participants reported that they sit at the center of more than ten stakeholder groups – including doctors, pharmacists, patients, family caregivers, logistics teams, operations teams, administrative departments, pathology teams, insurance teams, and surgical teams. This central position creates additional workload beyond their core responsibility of providing patient care. They explained that the most challenging part of their job is performing tasks outside their clinical expertise, such as administrative duties, service work, or supporting doctors with non-nursing tasks. Frequent communication with so many groups also leads to misunderstandings and inefficiencies. Nurses (U2, U3, P5, P17) expressed interest in AI systems that could mediate between them and other stakeholders or handle certain tasks on their behalf to reduce these communication burdens.
AI as a Mediator between Nurses and Doctors : In addition to the strong hierarchy in hospitals, nurses – who are mostly women – often have limited authority over doctors. In many cases, doctors are also professors, a role that carries additional prestige and authority in South Korea. Doctors sometimes treat nurses like secretaries, assigning them tasks considered less important. Communication with doctors is particularly challenging because, in cases of medical errors (e.g., administering the wrong medication), nurses – who execute the orders – are more likely to be held responsible than the doctors who gave them. Organizationally, nurses have less authority but greater responsibility.
This strict hierarchy makes it difficult for nurses to speak up or ask questions, even when doctors make mistakes. New nurses, in particular, find it challenging to question orders in person. As a result, nurses envisioned an AI system that could provide potential rationale behind doctors’ orders and highlight possible issues, minimizing the need for in-person interactions. A union branch manager at a large-sized, university-based hospital (U6) shared a potential AI that could mediate communication with doctors as follows:
“When doctors prescribe a drug, it’s fine if it’s a medication I’m familiar with. But if it’s prescribed for a different effect, like we mentioned earlier, and I don’t know it, I would normally look it up in a drug reference or pharmacopeia – but sometimes it’s not listed, or I don’t have time to check. In those cases, if it’s a doctor I know well, I can ask, ‘Doctor, why did you prescribe this?’ However, the current hospital culture doesn’t really allow for that kind of questioning. As a result, if you don’t know in the beginning, you might not understand why a patient is taking a certain medication later on. That’s why it would be helpful to have an AI that could easily resolve this.”
Nurses also noted that doctors have different preferences for communication (P5, P8, P15). Some prefer lab results via messages through the EMR system, others prefer phone calls, and some prefer notifications sent to their secretaries. Following these individual preferences adds complexity for nurses who are already overloaded with tasks. Therefore, nurses want an AI system that can track each doctor’ s preferred communication method and deliver information accordingly, allowing them to simply enter the necessary information and focus on patient care while the AI handles the complex communication.
AI as a Mediator between Nurses, Patients, and Family Caregivers : In addition to the strong hierarchy in hospitals, nurses, as frontline workers, spend a significant amount of time with patients and their family caregivers. While most patients appreciate nurses’ efforts, some are ignorant or even abusive. Nurses expressed interest in AI systems that could support their communication with patients and caregivers.
One type of AI envisioned is for patient education (P8, P10, P13, U1, U3). Nurses are responsible for explaining medical procedures – why they are needed, how they will be performed, and any follow-up tasks after discharge. Despite repeated explanations, patients or caregivers often fail to understand the information, requiring nurses to repeat themselves multiple times. In some cases, patients claim they were not properly informed, leading to repeated calls for clarification. To address this, nurses (P10, P13) imagined either a mobile AI agent or an embodied AI, like a robot, that can answer the same questions repeatedly (see Fig 3, Left). While nurses recognized that such systems cannot fully solve these challenges – especially for older patients with diverse questions – even a small reduction in repetitive interactions would be highly beneficial.
Nurses also noted that some patients distrust the information they provide (P5, P10, P14, U8, U9). For example, patients may question whether a procedure is correct or request to speak directly with a doctor, potentially reflecting microaggressions toward generally younger, female nurses. In such cases, nurses envisioned a robot displaying a doctor’ s image to provide basic procedural explanations, allowing nurses to address follow-up questions.
Additionally, technology-based communication could serve as proof that nurses provided appropriate information. In some instances, doctors penalize nurses based solely on patient complaints. If AI systems maintain records of information sharing, these data could provide valuable evidence of nurses’ efforts. A union branch manager at a large-sized, university-based hospital (U8) explained how AI could facilitate communication with patients while mitigating distrust toward doctors:
“Professors (doctors) sometimes criticize nurses for not explaining things properly to patients, or even claim that an explanation wasn’t given at all. An AI that provides necessary information, allows me to review it with patients, and tracks what has been shared could help reduce this distrust between nurses and doctors.”
Finally, nurses wanted AI to help identify abusive patients. They reported experiencing verbal or even physical abuse and suggested an AI system that tracks patient interactions and alerts them when patients with a history of abuse are nearby.
AI as a Mediator between Nurses and Administrator Teams : Nurses also hoped to reduce their administrative workload. One of the most demanding tasks is checking health insurance–related data (P5, U7, U9, U10). They must verify that each procedure is correctly listed across various forms, many of which are created by doctors who often enter incorrect codes. Nurses reported that this insurance-related work occurs once or twice a month and requires them to skip meals or stay overnight without proper rest, as they must handle it on top of their regular duties.
They envisioned an AI system that could automatically detect errors in procedural codes based on each patient’ s health condition and diagnosis (U9, U10). Nurses also noted that such a system could benefit patients, as incorrect codes sometimes result in procedures not being covered by insurance – errors patients may not even notice. They expected that this AI system would save time, allowing them to focus on patient care, which is their area of expertise.
AI for Fair Work Distribution
Because of the demanding workload, labour distribution has been a crucial issue among nurses. The work itself is stressful because it is time-critical and high-stakes, and without other ways to manage it, nurses often experience high levels of stress, which can contribute to bullying. This bullying is a well-known part of nursing culture in Korea, locally called “Taeoom” [24–26]. In extreme cases, this issue has contributed to severe stress or even suicide among junior nurses.
KHMU recognizes this as a serious problem. One of their efforts to manage Taeoom is to establish a scheduling committee that includes both senior nurses in managerial roles and junior nurses. Before the committee existed, head nurses sometimes penalized specific junior nurses by assigning them more demanding schedules, such as additional night shifts. Korean nurses currently work three shifts. While the total hours are the same, night shifts are generally more demanding.
AI for Scheduling and Bed Assignment : To further improve fairness, some union locals (U2, U3) began using AI scheduling systems that automatically create schedules based on factors selected by the committee. While minor adjustments are still made to the AI-generated schedules, nurses report better reactions to these schedules, feeling they reflect a more objective distribution of labour. Nurses also envision a similar AI system to assign nurses to patient rooms, taking into account patient severity and the distance from nurse stations (P5, P15). Not only the shift schedule but also patient assignments significantly influence workload.
AI for Patient Assignment : Furthermore, nurses both from MH and KHMU see potential for AI in patient assignment management. Hospitals often increase bed occupancy to increase profit, which can result in patients being assigned to units that are less relevant to their condition. When multiple unexpected patients are assigned to a unit, nurses face challenges due to unfamiliar procedures and doctors, leading to increased stress. Nurses with less authority may be asked to handle more work and criticized for inefficiencies. To prevent this, some strategic head nurses coordinate with administrative staff to assign patients requiring lighter care to their units. However, if a head nurse has limited connections with administrative staff, the unit may end up with patients needing more intensive care. To make this process fairer, nurses hope an AI system could objectively assign patients based on their condition, potential workload, and past assignment history. A union secretary at a large-sized, university-based hospital (U10) described how the AI system supports patient assignment as follows:
“And when assigning patients to rooms, sometimes a single ward ends up with a high concentration of patients. When that happens, conflicts can arise, like, ‘Why do we have this many patients while they don’t?’ If we could analyze the severity of the patients assigned to each ward, we could identify cases where a patient might be too difficult for a certain ward. This seems related to the earlier discussion about patient assignment. It would be helpful to have a feature that can automatically adjust or optimize these assignments.”
AI for Improving Productivity and Efficiency
Similar to findings in existing literature on AI systems for workers, nurses from both MH and KHMU expected AI to enhance the productivity and efficiency of their work. They desired AI that could support decision-making in medical procedures, improve their approaches to error management, and provide complex information not commonly encountered in their daily practice.
AI Supporting Medical Procedures : KHMU nurses expressed a desire for AI systems capable of identifying and notifying them of emerging issues, such as delirium or pressure ulcers (U1, U2, U5). Their goal was to proactively monitor high-risk patients.
However, similar systems previously implemented at MH – which used EMR data to predict falls and bedsores – met with limited success. While some nurses found these features helpful, trust remained low due to limited perceived accuracy and difficulties in understanding the rationale behind the AI’s decisions. Consequently, MH staff found it challenging to communicate risks to patients without a clear rationale for the AI’ s findings. This highlights the practical challenges of integrating predictive systems into clinical workflows.
AI Handling Errors : The KHMU and MH nurses expected an AI system that could alert them to potential errors in the EMR. Occasionally, either they or doctors enter incorrect information into the EMR, which can lead to serious issues, such as inaccurate medication records (P16, U6, U10).
While nurses saw AI as a tool to help manage errors more effectively, they expressed concern that increasing reliance on technology could lead to deskilling (P8, U1, U2, U3, U8). At the same time, they noted that the increasing availability of medical equipment (e.g., life scope monitors versus manual vital sign checks) is helpful and beneficial. Nonetheless, participants universally agreed that education in critical thinking remains essential, even in highly automated environments, to manage scenarios involving equipment unavailability or technological failure.
AI Handling Complex Information : Both MH and KHMU Nurses envisioned an AI system capable of providing information about medications or medical procedures with which they are less familiar. Although nurses are trained across multiple areas, they occasionally encounter rare cases. For example, doctors may prescribe medication not for its primary effect but for secondary or tertiary effects (U7). Existing search systems often fail to provide the precise information nurses need in these situations. An AI system specifically trained to address such rare cases could therefore be extremely helpful.
The same applies to procedures that nurses rarely perform. For instance, nurses in certain units may infrequently manage bedsores (P14). As a result, assessing the severity of a bedsore or determining the appropriate materials, such as pads, can be confusing.
This is why the bedsore AI system at MH, which analyzes pictures taken and uploaded by nurses to diagnose bedsore severity and recommend optimal medical procedures, was particularly helpful for gastroenterology nurses. However, for nurses caring for more bed-ridden patients, the system was often inaccurate – its diagnostic performance is sensitive to room brightness – resulting in extra work (P10). In these cases, nurses could more efficiently assess the bedsore visually without taking a picture, uploading it to the AI system, and checking the suggestions. Consequently, the AI system proved most useful for nurses performing specific procedures they do not encounter frequently. This does not necessarily mean that newer nurses find all AI systems more helpful; in fact, the nurses who valued the system most had over seven years of experience. This suggests that AI can more effectively support tasks that are performed only occasionally, regardless of a nurse’s overall seniority.
AI in Managing Economic Disparities among Hospitals
Although this discussion was not about a specific AI system, the KHMU nurses emphasized that an ideal AI system should not exacerbate existing resource gaps among hospitals in South Korea. All participants in this study were nurses from large hospitals in Seoul, which generally have more resources than smaller hospitals outside the capital. Even among these large hospitals, resource disparities were evident.
For example, MH has abundant resources, including easy access to software engineers from an affiliated IT services subsidiary, who provide IT services ranging from software development to maintenance. Its EMR system is also developed by this subsidiary. In contrast, one nurse participant from a national institution (U7) affiliated with the Ministry of Health and Welfare highlighted that EMR systems vary across hospitals. Even when hospitals use EMR systems from the same company, features vary depending on each hospital’s budget.
Since many prediction models are developed using historical patient data from EMRs, hospitals start from very different baselines due to variations in EMR quality. Beyond these existing disparities, nurses were concerned that implementing additional AI systems, which require financial investment, could further widen the gap. Ideally, they hope that such AI systems would be equally accessible across hospitals, either through government support or public health policy initiatives. U7 explained her concerns about the relationship between resource gaps and AI adoption as follows:
“When I think about AI, I realize that, since my hospital is a public institution, it always operates at a deficit. The resource gap among hospitals is significant because, unlike in other countries, hospitals in Korea are not fully public. This means that AI would likely be adopted first by hospitals that generate more revenue. I wondered whether, when introducing AI technology, it should be left to individual hospitals or implemented nationally by the government. Considering that AI is closely linked to patient safety, I believe that, if necessary, it should be implemented at the national level – for both hospitals in rural areas and those in Seoul. Because advancements in nursing technology and related areas are directly connected to patient safety, I believe patients in Seoul and in rural areas should receive the same level of service.”
Findings Part 2. Automating Care: Success, Failure, and the Gap Between Technology and Need
This section provides three patterns that distinguish the success and failure of various technologies, including AI systems, in a hospital setting. This analysis is primarily based on the ethnographic study conducted at MH, where the research team was able to obtain a more holistic view of various technology adoption cases.
Pattern One: When Automation Works
Eliminating Drudgery and Unpaid Preparation Time
From nurses’ perspective, successful automation involves 1) reducing drudgery and 2) increasing the time they can focus on care work.
Reducing Drudgery : Every morning before the logistics robot system was implemented, nurses arrived at the hospital between 6:00 and 6:30 AM for shifts that officially began at 8:00 AM. P5, a nurse with extensive clinical experience, described this ritual: “I came 1.5 to 2 hours early – one hour for patient assessment and 30 minutes to find supplies.” This time fell outside their officially scheduled hours. When we asked why nurses didn’t simply arrive at 8:00 AM, P15 explained the logic that naturalized this practice: “It’s attributed to your personal capability.” This framing suggested that the duration of pre-shift preparation depended on individual capability rather than systemic design.
What nurses were doing during these pre-shift hours becomes clear in P14’s account of the pre-automation morning routine: “Before, the first thing nurses did when arriving was equipment check… [we] must find 10 items... going around several times checking and checking.” She described searching for SpO2 monitors, infusion pumps, and other mobile equipment scattered across multiple patient rooms, borrowed by the night shift, or taken to other wards. This was followed by inventory verification: printing daily usage reports, manually counting supplies in each drawer, comparing against standard quantities, and calling other wards to borrow items that had run short. P16 added another layer: “Expiration date management for items in the carts was also a problem. We had to maintain first-in-first-out for all the cart supplies.”
The logistics robot system eliminated this entire routine overnight. Automated supply replenishment based on pre-calculated standard quantities meant that nurses no longer needed to count, order, or verify inventory. RTLS tags on equipment meant that P14 could now “just open the screen and it shows where all 10 items are”. The transformation was immediate and universal. Across all 17 participants – from 4-year nurses to senior managers, from ICU to rehabilitation units – we heard consistent praise. P17 summarized the consensus: “[the logistics robot] is convenient for nurses... no inconvenient points at all.”
Increasing Time for Care Work : The significance of this automation extends beyond time savings. P16 described an unexpected benefit: “As that time becomes free, my mind stabilizes, and my sharp nerves calm down a bit”. The elimination of morning logistical stress created emotional capacity for patient care. P6, a nurse administrator involved in the rollout of the logistics robot system, showed us satisfaction survey results: 4.5 out of 5 across all metrics. She explained why: “Time spent on supply management greatly decreased... that much more time to see patients.”
The RTLS equipment tracking system had similarly eliminated the 1-2 hours of early arrival before officially scheduled hours for equipment search – what multiple nurses described as the most “dramatic improvement.” P17 explained the change: “Before, we came an hour early... but by utilizing this technology we could drastically reduce that work... so now we can arrive on time.” This represented not just efficiency gains but a structural recognition that preparation work is a necessary part of the job – not a reflection of individual inadequacy.
The Conditions of Success
While a bottom-up approach – designing technology based on issues identified in the field together with frontline workers – contributes to the successful design and adoption of technology (e.g., crash carts for cardiac emergencies, which require rapid access to resuscitation equipment and were re-designed through nurse input at many institutions), a top-down approach – implementing technology through management directives – can also support successful adoption. In this section, we present how these two approaches worked.
Bottom-up Approach : Several conditions distinguished these successes from the failures we examine later. P7, a manager in infrastructure operations involved in robot deployment, described the logistics robot’s development process: year-long weekly meetings involving five departments – nursing, facilities, purchasing, IT, and logistics. P3, a a staff member in digital transformation, emphasized the iterative design cycles: “Pre-meetings, requirement gathering, 1st, 2nd, 3rd, 4th design iterations... exchanging feedback... that period took longest.” The robot manufacturing took 2-3 months; the collaborative design process took 3-4 months.
Yet this “co-design” process contained a crucial ambiguity about whose voice counted as “the field.” P7 claimed that “Robots are requested by field workers (nurses working in the clinical field)”, while P5’s experience of the same system was that it “one day was just there in the ward.” The resolution to this apparent contradiction lies in recognizing that “field” meant different things to different actors. For administrators, “field” included nurse managers and ward leaders who understood inventory burden as an aggregate problem affecting ward operations. For bedside nurses, “field” meant themselves – the individuals doing the daily work. The Magic Cart succeeded because it solved a problem that both groups acknowledged, even if they experienced it differently.
P6 (a former bedside nurse currently working in clinical innovation), who oversees daily operations of the logistics robot, highlighted the overlooked downside of its success, particularly regarding stakeholders who are excluded due to the limited definition of the field. While nurses universally praised the system, she described the warehouse workers who now manually counted items for each cart: “One person packs for 4 departments, about 30 carts, doing that all day long... standing and I felt like gagging from watching.” While the automation reduced nursing workload, it shifted some operational burden onto third-party warehouse staff. From the institutional perspective, this represented an overall improvement in care time allocation.
Top-down Approach : The BPOC (Barcode Point of Care medication verification)4 followed a different trajectory to success. Unlike the logistics robot, which was welcomed from the start, BPOC faced initial resistance that eventually transformed into acceptance. P10 described the early adoption phase: “The hospital publicly displayed BPOC usage rates... ‘Your usage is under 80%, so we send you notes.’ ”This metric-driven enforcement created what she saw as contrarian reactions among nurses, captured in complaints like ‘Why do they evaluate everything I do?’ But over time, as nurses habituated to carrying the device, perception shifted. P13 now described it as a “last safety device”: “because I’m human... sometimes it’s hectic. But if I make a mistake or prepare the wrong medication... the device says “not this person.”’ P10 summarized the evolution: “It became so familiar... I guess you’d say it became routine.”
Pattern Two: When AI Fails
Gap between Contextual and Model-based Predictions
The fall risk prediction CDSS (Clinical Decision Support System) represented the hospital’s investment in what administrators saw as cutting-edge AI-based clinical decision support. The system calculated fall probability based on patient age, medications, mobility scores, cognitive status, and recent vital signs. Every morning, nurses reviewed color-coded alerts identifying high-risk patients who required enhanced monitoring, bedside safety equipment, and frequent checking. But at the rehabilitation unit, these predictions had become what she called “noise” – signals that nurses learned to ignore.
She explained why during an evening shift interview, surrounded by wheelchairs and parallel bars: “From our experience, when we give patients medication that might cause dizziness, we tell patients and caregivers ‘This might make you dizzy, so please use the urinal in bed only,’ but ultimately many fall incidents happen because of patient or caregiver non-compliance with these instructions.” She described a patient who had been marked low-risk by the system – appropriate age, no high-risk medications, good mobility scores – who fell because he decided to walk to the bathroom despite being told not to. Another patient, marked high-risk, never fell because his daughter was vigilant. The system calculated risk from medical variables; the reality was behavioral and, as she put it with resignation, ultimately ungovernable: “People who are going to fall will fall anyway.”
P17’s assessment was blunt: “Computer calculations are based on clear evidence-based factors. But here many accidents happen from human non-compliance, so often doesn’t match.” When we asked if nurses consulted the CDSS predictions, she shook her head: “We don’t judge based on the [fall risk] percentage. More than the percentage, we rely on what we’ve accumulated through direct experience with this caregiver or patient – ‘this person really doesn’t comply with instructions, right? This patient seems like they won’t follow this again’ – these experiences. For these to be reflected, we’d have to input them into the system, but we can’t automatically put this into the computer... What computers calculate is based on clear evidence-based factors.”
P10, working in the surgical ICU, described how the initial engagement with CDSS predictions gradually shifted toward more passive use, as nurses found it difficult to influence the system’s outputs based on their clinical judgment : “At first, if I felt this patient didn’t seem high-risk for falls, I would inquire with the system team about it, but later it became ‘Oh whatever, I don’t know anymore, let’s just do what it tells us.’ ” This was not trust but resignation – a shift from active questioning to passive compliance driven by the impossibility of changing the system’s outputs. P2, in the professional development team managing these systems, had spent six months trying to address what she described as an intractable problem: “When it’s clinically not high-risk but the AI flags it as high-risk... I don’t know how we can bridge that gap... it seems really difficult.”
The problem was not simply inaccuracy but a fundamental mismatch between what algorithmic prediction requires – stable, calculable risk factors – and what clinical reality presents – volitional human behaviors that refuse calculation. P17 captured this when she said the system worked better in medical wards where patients were more compliant with restrictions: rehabilitation patients, determined to prove their recovery, were the least governable by algorithmic prediction.
Gap between Lab and Real-world Settings
While the fall prediction CDSS encountered fundamental limits in modeling volitional behavior, the pressure ulcer staging mobile application failed for different reasons. The app used computer vision to classify pressure ulcer stages from smartphone photographs, providing real-time assessment support at the bedside. P1, who helped implement it, initially framed it as a solution for junior nurses uncertain about staging: “When it’s hard to judge alone, when the pressure ulcer stage is ambiguous – stage 2 or stage 3... the app suggests the stage and treatment products according to the ulcer condition... so I think they can manage the patient’s pressure ulcer independently.”
But P16, an experienced surgical-specialty nurse, explained why she and her colleagues didn’t use it:
“There’s a slight difference between natural light and camera... whether it photographs as purple or reddish or pink affects stage assessment.” P10 was more direct about the lighting problem: “Depending on brightness it’s fine but in darkness suddenly says DTI [deep tissue injury]).” Pressure ulcers, by their nature, occur in areas difficult to photograph: buttocks, sacrum, heels – locations requiring patient repositioning in already dim lighting. Using flash “worsened recognition accuracy further” (P10).
When uncertain about staging, they consulted senior nurses, not the app. P17 explained the app’s low credibility: “Say someone classifies an ulcer as stage 3. But if it doesn’t look like stage 3 and you ask ”Who said stage 3?” and they answer “The pressure ulcer app said so” – that’s not actually trustworthy.’” The app existed outside the professional consultation hierarchy: junior nurse —> senior nurse —>PWN (wound-certified nurse) —> ward nurse leader. Technology that did not align with this existing chain of clinical consultation faced challenges in becoming part of routine practice, regardless of its laboratory validation accuracy.
A separate but related failure emerged from the RTLS (real-time location system) equipment tracking implementation, which is distinct from the pressure ulcer imaging app discussed above. P8 added another dimension to the failure: the RTLS tags attached to equipment. Designed to eliminate the counting burden, the tags instead doubled it. “[we nurses are] ended up counting double... count equipment and also count the location tracker... ultimately counting twice.” The tags frequently detached during equipment transport. P17 explained: “The size is bigger than expected... this blocky rectangle has to be additionally attached to equipment... and we often take equipment to the rehabilitation area, so during transport it bumps into things and falls off.” Nurses now had to count equipment, verify tags were attached, match tag numbers to equipment IDs, and search for detached tags. Although the tags created additional workflow challenges for nurses, the initial investment in the system limited options for change.
Pattern Three: The Persistent Gap
What Nurses Asked For
When P13 described her daily work in a surgical specialty ward, she lingered on one task: patient education. “When patients come for specific surgical procedure, about 8 are admitted per day. The explanation is identical – I give the same explanation to all 8 people.” She walked us through what she explained: pre-operative preparation, the surgery itself, post-operative care, catheter management, pain medication, infection signs, incontinence exercises, follow-up schedule, sexual function recovery. The content was completely standardized – in fact, it was already written in detailed brochures.
Her role was what she called “helping them absorb it visually and aurally” – reinforcing written information through verbal repetition.
This took 20-30 minutes per patient. Eight times per day. She found it draining: “I wish just that part – repeatedly saying the same thing – could be reduced.” When we asked if she thought elderly patients could handle video education, she rejected the common objection: “People say ‘Because they’re elderly, won’t they have trouble viewing?’... but actually these days elderly people also watch YouTube so much... [so in my view] I think everyone can do it.” Her conclusion was direct: “Couldn’t an AI robot do at least that much?” P13 was not alone. P10 in the ICU described education as taking “20-30 minutes just pass – at least twice as long as medication administration. P8 called it “takes the longest” and explicitly said she would be willing to let AI handle it: “I think education doesn’t absolutely require people – as long as continuous information delivery [to patients] happens, I think AI or robots doing it would be fine.” P16, despite being more cautious about automation generally, agreed that because “Current patient education work is, from a nursing perspective, extremely repetitive work, so it is an appropriate” automation target.
Yet this automation had not been attempted. The hospital had invested in fall prediction CDSS, pressure ulcer imaging AI, and various other “advanced” systems, but not in the straightforward video/tablet education system that multiple nurses explicitly requested. P15 had a different priority: drug interaction checking. As nurses had absorbed pharmacist responsibilities for medication preparation, they now needed to know “some antibiotics must mix only with saline, some only with dextrose”, plus concentration requirements, pump usage rules, and potential crystal formation from incompatible drugs. She wanted an AI system that would alert her during preparation: “I wish it could detect things like ‘This drug interaction shouldn’t happen – crystals might form.’ Currently there’s nothing that filters this, so nurses have to verify everything, but we can’t remember all those medications.”
P17 wanted ARS (Automatic Response System)-style call bell filtering. Her rehabilitation ward received constant calls – transport requests, toileting assistance, minor questions – that interrupted nurses continuously. “Like ARS, if you press 1 it would automatically route to transport” – a simple triage mechanism that could route routine requests to appropriate staff, leaving only urgent or ambiguous calls for nurses. P8 and P10, both working in ICU, wanted assistance with patient repositioning – the task that caused chronic wrist and back injuries: “Every two hours... two people (a nurse and transport staff) must lift a patient weighing about 90kg... so back discs develop or wrists get injured frequently.” While this request falls more squarely in the domain of physical assistance technology than AI per se, it reflects a broader pattern of nurses identifying high-burden, injury-prone tasks that remain unaddressed by current technology investment.
Why Patient Education Automation Didn’t Happen
The case of patient education automation is particularly revealing because it represents nearly an ideal candidate by conventional design criteria. The task is highly repetitive (8-15 times daily for identical content). It’s completely standardized (detailed brochures already exist). It’s temporally extensive (20-30 minutes per patient, consuming 4-6 hours daily). The technology is straightforward and cheap (video on tablets with QR code access). The target population can handle the technology (YouTube usage is widespread among elderly). And nurses explicitly requested it.
Yet when we asked P4, who works in digital transformation, why this hadn’t been pursued, he hesitated: “Fantastical things mainly come up as needs among nurses... they feel like they could be realized soon, but we can’t do it with our current resources.” This response was puzzling – education videos require less sophisticated technology than the computer vision algorithms deployed for pressure ulcer staging. P2 offered a different explanation: “It doesn’t seem to come from the field – from actual needs or voices... now it’s just technology-first.” Technology adoption was often informed by what nurses described as conference exposure: “When (physician professors) see AI things at international conferences and come back saying ‘let’s try this too’ – there’s a lot of that.”
Multiple lines of evidence from our fieldwork point to the same pattern: predictive analytics, computer vision, and machine learning showcased at conferences like HIMSS (Healthcare Information and Management Systems Society) attracted institutional investment, while simple but high-impact video systems did not. P14, a charge nurse (senior nurse manager) with 25 years of experience, revealed the underlying logic when she described the hospital’s quality improvement trajectory: “Al-though AI and robot introduction saved lots of time, our expectations for medical quality rose accordingly... certification standards keep getting higher and higher than before.” Technology adoption decisions in academic medical centers respond to multiple institutional pressures, including accreditation, research, and clinical needs. The case of patient education automation suggests that simple, high-impact tools may be underrepresented when investment priorities are shaped primarily by external recognition criteria.
These three patterns – successful automation of acknowledged problems, failed prediction of volitional behavior and messy reality, and persistent gaps between nurse needs and institutional priorities – reveal how organizational hierarchies, design processes, and evaluation criteria shape which aspects of care work get automated and which remain untouched. The logistics robot succeeded because it solved a problem visible to both management and staff, required year-long collaborative design, and eliminated work without requiring patient compliance. CDSS and imaging systems failed because they attempted to calculate the volitional, assumed lab conditions in clinical reality, and prioritized institutional metrics over clinical utility. Education automation never happened because it wasn’t technically impressive despite being clinically impactful.
What links these patterns is the question of whose needs drive technology adoption. When we ask this question, we find that “the field” is not a unified entity but a hierarchy of voices with differential access to decision-making. The perception gap between charge nurses’ more positive assessments and bedside nurses’ more cautious accounts reflects not just individual differences but structural positions that influence which perspectives shape future technology decisions.
Discussion
The Role of a Labour Union in AI Adoption
Our findings indicate that AI systems in hospitals with unions, compared to those without, exhibit distinct characteristics in three key areas: 1) the values prioritized in their implementation, 2) the level of technological advancement and resources allocated, and 3) the degree of nurses’ involvement in the process. This comparison highlights the significant role that labour unions play in AI adoption.
While there are benefits to AI initiatives led by hospital leadership, unions are crucial in shaping AI to prioritize labour-centered interventions.
Some of the differences observed in our study may also stem from sampling bias, as we engaged different stakeholders through different methods. At MH, a hospital without a union, we conducted ethnographic observations and interviewed not only nurses but also hospital leadership and institutional innovation teams, whereas in the unionized hospitals, we interviewed only nurse union representatives. However, because nurses were the primary participants in both groups, the sampling differences and methodological variation may not be the central factors shaping the differences in AI adoption.
Central Values Prioritized in AI Adoption
Nurses in both unionized and non-unionized hospitals face similar labour challenges, such as high workloads and the expectation to perform tasks outside their primary expertise. However, the driving forces behind AI adoption differ. In hospitals with unions, the focus of AI adoption is on addressing these labour issues, while in non-unionized hospitals, priorities tend to center around technological innovation and potential profitability.
At MH, a hospital without a union, efforts to address nurses’ labour concerns have been made by involving nurses in the planning, adoption, and evaluation phases. However, nurses are not typically part of the decision-making team that leads the final adoption process. The institutional logic driving AI adoption at MH is illustrated by the case of the logistics robot, one of its most successful adoption initiatives. This project gained significant momentum, largely due to strong support from the hospital’s leadership. MH, like many established academic medical centers, faces significant space constraints that make it difficult to introduce new medical devices. According to unionized nurse participants, similar space constraints exist in other facilities, as most large hospitals in Seoul were built several decades ago when medical technology was limited. At MH, the leadership aimed to bring advanced equipment to the radiology clinic, but the existing building did not have sufficient room to accommodate the new technologies. While searching for available space in the cancer center, they discovered that a substantial area in the basement was being used to store medical materials and supplies – from syringes to medications.
The leadership realized that adopting the logistics robot system could free up this storage area for the new radiology equipment. With the logistics robot, logistics companies deliver pre-stocked cabinets instead of boxes of materials. These cabinets are then loaded onto mobile robot platforms, which transport them to the wards. As a result, tasks previously performed by MH’ s logistics specialists and nurses were shifted to a third-party logistics company. This allowed the hospital to repurpose its physical space for additional clinical services. While nurses were highly satisfied with this change – mainly because it reduced one category of miscellaneous tasks – the logistics team’s role was significantly restructured. The reduction in nurses’ workload, though substantial, was one of several outcomes of the adoption rather than its sole driver.
In contrast to the non-unionized hospital, the primary goal of AI systems in hospitals with unions is to directly address existing labour issues. If the logistics robot represents the most successful AI example in the non-unionized setting, the AI scheduling system and AI interview system are the most successful examples highlighted by the unionized nurse participants. Both systems are closely aligned with labour concerns that unions have long sought to resolve. As noted earlier, fair workload distribution among nurses has been a major priority, prompting central unions to advocate for the establishment of scheduling committees across hospitals with local unions. The AI interview system was also introduced as a potential solution to reduce the workload associated with low retention rates, which are closely tied to the demanding and stressful working conditions nurses experience.
Technological Advancement and Resource Gap
In terms of technological advancement, MH – the non-unionized hospital – has experimented with a wider range of advanced technologies than the unionized hospitals. Examples include a human-like mobile robot deployed for rehabilitation and inpatient rounding, smart food trays that automatically record patients’ intake and output, and the successful logistics robot, an automated system for material handling. Union representatives noted that such technologies were not available in their hospitals. By contrast, the AI systems used in unionized hospitals tend to be commercially available tools with relatively simple functionalities rather than cutting-edge technological innovations. These differences may reflect resource disparities – including differences in human resources, budget, and technical capacity – between MH and the unionized hospitals.
MH has access to a range of resources that enable it to test and adopt innovative technologies. The hospital hosts multiple innovation-focused teams, some of which are permanent units staffed by full-time employees with research backgrounds who secure government-initiated grants for various pilot tests. In addition, MH has a designated nursing-focused innovation team that monitors new AI systems – such as the fall-prevention AI model – although the team is small, consisting of only two nurses. MH also operates an annual short-term innovation program through which any nurses can apply to participate and develop ideas to improve their care work.
MH’s institutional affiliations support access to various internal grant programs that fund collaborations between clinical and engineering researchers. These funding opportunities enable multiple short-term and long-term projects exploring a wide range of AI technologies. In contrast, KHMU is primarily focused on addressing its members’ labour issues and only occasionally explores how AI systems might help alleviate those concerns. MH also has relatively easy access to IT services and consulting through in-house software engineering capabilities. However, as our findings show, this resource advantage did not prevent the fall-prevention AI system from generating low trust among bedside nurses due to accuracy problems and limited clinical transparency.
Compared to MH, the union primarily focuses on labour issues arising from its members’ work contexts and explores potential technological solutions. As a result of these efforts, AI is sometimes identified as a promising solution; however, the union generally only has access to existing commercialized technologies rather than research and development resources. Additionally, unions in Korea often face a mixed public reputation despite their importance. For example, the central union leader noted that local residents initially opposed the construction of a designated building for the KHMU. Increased funding and support are needed at the policy or national level to either provide unions with the resources to engage in AI adoption or to mandate that they play a more significant role in shaping AI policy for nursing.
Decision-making Process
In the absence of a union at MH, nurses are involved in the AI adoption process, but primarily as followers rather than as leaders or negotiators. The presence of a nurse innovation care team indicates that nurses’ perspectives are considered in technological innovation; however, the team is small, with only two members, and has limited budgetary resources. Other nurses, whose main focus is patient care, are occasionally included as participants, but the units and individuals selected for participation are chosen by the ward nurse managers and the Digital Transformation team – composed mainly of researchers rather than nurses – and are expected to follow the team’s directives.
Most decisions regarding AI system planning, implementation, and adoption are made by hospital leadership, with priorities including technical innovation, operational efficiency, and organizational strategy alongside clinical needs. This leadership-driven approach shapes how labor considerations are incorporated into AI system selection.
The adoption of BPOC at MH illustrates, for example, how technology adoption is largely driven by leadership decisions. When the system was first introduced, not all nurses were willing to use it. Nevertheless, hospital leadership monitored the technology’ s usage and reported the results to mid-level nurse managers in each unit. Leadership also provided comparisons between units, highlighting those with the lowest usage rates. This prompted managers to review individual nurses’ usage, and nurses with the lowest rates received warning messages.
During the early adoption phase, some nurses noted physical challenges with carrying relatively bulky and heavy BPOC devices throughout their daily routines. While many nurses eventually recognized the system’s usefulness, adoption was driven primarily through institutional metrics rather than ground-up uptake. Similarly, the fall-prevention AI system has been implemented in a way that nurses cannot bypass its suggestions when a patient is identified as high-risk. Although this leadership-driven approach can facilitate the successful adoption of new technologies, nurses in hospitals without unions can raise individual concerns through internal channels but have less collective leverage to shape or contest technology decisions that may negatively affect their work.
In contrast, in hospitals with unions, nurses are able to report their difficulties and have greater leverage to negotiate concerns related to technology adoption. Although nurses’ voices in Korean hospitals are generally weaker than those of doctors, the AI systems discussed by union representatives were largely developed through a bottom-up approach. All AI adoptions were grounded in the primary concerns of nurses.
Automation and Nursing
Based on the findings of this study, automation is unlikely to displace nurses in the near future, largely because the current demand for nursing labour far exceeds available staffing. Nursing in Korea is characterized by exceptionally high labour intensity: the average patient-to-nurse ratio is 12–13, compared to 4 in Australia and Canada, 5 in the United States, and 7 in Japan. This heavy workload contributes to significant burnout and turnover, with an overall dropout rate of 14.5%, half of which consists of nurses leaving within their first year. According to a 2022 news report, some nurses were able to take only three lunch breaks in an entire month due to extreme labour demands [28]. The combination of high workload, limited staffing, and low retention rates creates a practical need for automation – particularly for tasks that are not directly tied to nursing expertise. In this context, automation functions less as a replacement for nurses and more as a necessary support mechanism to alleviate the burden of non-core duties.
Compared to manufacturing settings, the automated logistics platform used in our field site – known as the Magic Cart – resembles systems commonly found in factories. Based on the PI’ s prior experience in two large multinational manufacturing plants in the United States, the introduction of automated platforms such as autonomous mobile robots (AMRs) and automated guided vehicles (AGVs) often heightened production workers’ concerns about job displacement – and in many cases, displacement did occur. As a result, production workers tended to view these robotic platforms very negatively due to threats to job security. In contrast, nurses in our field site responded almost oppositely. One possible explanation is that nurses are not the primary workers responsible for logistics; that responsibility falls to the logistics team. Similarly, in manufacturing settings, the workers most directly responsible for logistics tasks (e.g., forklift drivers) were the ones who expressed the greatest concerns about robotic platforms.
These contrasting reactions to the same robotic platform can also be interpreted through economist Acemoglu’ s task-based framework [28]. Acemoglu argues that automation can increase productivity and expand an industry – ultimately generating more employment for non-automated tasks – but only when there is an actual shortage of human labour. When applied to nursing, this theory suggests that, given the high labour intensity and chronic staffing shortages, automation can provide genuine benefits by alleviating non-core tasks and enabling nurses to focus on specialized care. In contrast, manufacturing work is highly streamlined and tightly structured, making tasks easier to automate even when human labour is readily available. In such contexts, automation often replaces workers rather than complementing them, leading to job displacement and limited productivity gains.
Although there may be a threshold beyond which additional automation is unnecessary, the current Korean nursing context does not yet appear to be close to that point. Increased automation – especially when AI systems are implemented with the meaningful participation of nurses or the collective input of unions – has the potential to substantially improve working conditions and support the workforce.
Conclusion
AI adoption in South Korean hospitals is rapidly expanding, spanning a diverse range of technologies – from embodied AI, such as Autonomous Mobile Robots (AMRs), to AI-driven nursing interview systems and fall-risk prediction tools. This study shows that technology availability alone does not determine success. What matters equally is whose needs drive adoption and whether frontline nurses are meaningfully included in design and decision-making. Technologies succeeded when they addressed problems acknowledged by both management and bedside staff; they failed when they prioritized institutional prestige over clinical utility; and the most impactful automations nurses requested were never built at all.
Organizational structure shapes these dynamics significantly. The implementation of AI systems often depends on a hospital’s specific resources and organizational structure: For unionized hospitals, AI integration tends to focus on core labour issues, such as ensuring an equitable division of labour and reducing burnout. For non-unionized hospitals, adoption is often driven by leadership’s vision. While this can include nurse-centric improvements, it is frequently influenced by market-driven perspectives and operational efficiency. Policy frameworks should support nurse representation in AI planning across both contexts, prioritize need-first over technology-first investment, and ensure AI literacy education so nurses can engage critically with the systems they work alongside. The central lesson is that “the field” is not a unified voice but a hierarchy of perspectives. Closing the gap between institutional definitions of innovation and frontline experiences of work is not just a design challenge – it is a matter of labor rights, patient safety, and the future of nursing.
References
[1] A. Martinez-Ortigosa, A. Martinez-Granados, E. Gil-Hernández, M. Rodriguez-Arrastia, C. Ropero-Padilla, and P. Román, “Applications of artificial intelligence in nursing care: A systematic review,” Journal of Nursing Management, Vol. 31, No. 3, pp. 730-743, 2023.
[2] S. Maleki Varnosfaderani and M. Forouzanfar, “The role of AI in hospitals and clinics: Transforming healthcare in the 21st century,” Bioengineering, Vol. 11, No. 4, p. 337, 2024.
[3] Q. Wei, S. Pan, X. Liu, M. Hong, C. Nong, and W. Zhang, “The integration of AI in nursing: Addressing current applications, challenges, and future directions,” Frontiers in Medicine, Vol. 12, p. 1507917, 2025.
[4] M. K. Rony, A. Das, M. I. Khalil, U. R. Peu, B. Mondal, M. S. Alam, A. Z. Shaleah, M. R. Parvin, D. M. Alrazeeni, and F. Akter, “The role of artificial intelligence in nursing care: An umbrella review,” Nursing Inquiry, Vol. 32, No. 1, p. e12648, 2025.
[5] H. von Gerich, H. Moen, L. J. Block, C. H. Chu, H. DeForest, M. Hobensack, M. Michalowski, J. Mitchell, R. Nibber, M. A. Olalia, L. Pruinelli, C. E. Ronquillo, M. Topaz, and L. Peltonen, “Artificial intelligence-based technologies in nursing: A scoping literature review of the evidence,” International Journal of Nursing Studies, Vol. 127, p. 104153, 2021.
[6] S. O’Connor, Y. Yan, F. J. Thilo, H. Felzmann, D. W. Dowding, and J. J. Lee, “Artificial intelligence in nursing and midwifery: A systematic review,” Journal of Clinical Nursing, Vol. 32, No. 13-14, pp. 2951-2968, 2022.
[7] Y. Park, S. J. Chang, and E. Kim, “Artificial intelligence in critical care nursing: A scoping review,” Australian Critical Care, Vol. 38, No. 4, p. 101225, 2025.
[8] G. T. Babalola, J. Gaston, J. Trombetta, and S. T. Jesso, “A systematic review of collaborative robots for nurses: Where are we now, and where is the evidence?” Frontiers in Robotics and AI, Vol. 11, 2024.
[9] C. E. Ronquillo, L. Peltonen, L. Pruinelli, C. H. Chu, S. Bakken, A. Beduschi, K. D. Cato, N. R. Hardiker, A. Junger, M. Michalowski, R. Nyrup, S. A. Rahimi, D. N. Reed, T. Salakoski, S. Salanterä, N. Walton, P. Weber, T. Wiegand, and M. Topaz, “Artificial intelligence in nursing: Priorities and opportunities from an international invitational think-tank of the Nursing and Artificial Intelligence Leadership Collaborative,” Journal of Advanced Nursing, Vol. 77, No. 9, pp. 3707-3717, 2021.
[10] J. White, M. Gunn, M. Chiarella, H. Catton, and D. Stewart, “Renewing the definitions of ‘nursing’ and ‘a nurse’: Final project report,” tech. rep., International Council of Nurses, Geneva, Switzerland, June 2025.
[11] K. H. Pine and M. Mazmanian, “Artful and contorted coordinating: The ramifications of imposing formal logics of task jurisdiction on situated practice,” Academy of Management Journal, Vol. 60, No. 2, pp. 720-742, 2017.
[12] A. M. Taylor, H. R. Lee, A. Kubota, and L. D. Riek, “Coordinating clinical teams: Using robots to empower nurses to stop the line,” Proceedings of the ACM on Human-Computer Interaction, Vol. 3, No. CSCW, pp. 1-30, 2019.
[13] A. Strauss, “Work and the division of labor,” The Sociological Quarterly, Vol. 26, No. 1, pp. 1-19, 1985.
[14] T. Greenhalgh, J. Wherton, C. Papoutsi, J. Lynch, G. Hughes, C. A’Court, S. Hinder, N. Fahy, R. Procter, and S. Shaw, “Beyond adoption: A new framework for theorizing and evaluating nonadoption, abandonment, and challenges to the scale-up, spread, and sustainability of health and care technologies,” Journal of Medical Internet Research, Vol. 19, No. 11, p. e367, 2017.
[15] J. Vines, R. Clarke, P. Wright, J. McCarthy, and P. Olivier, “Configuring participation: On how we involve people in design,” in Proceedings of the SIGCHI Conference on Human Factors in Computing Systems (CHI ’13), pp. 429-438, ACM, 2013.
[16] E. Cho, D. M. Sloane, E.-Y. Kim, S. Kim, M. Choi, I. Y. Yoo, H. S. Lee, and L. H. Aiken, “Effects of nurse staffing, work environments, and education on patient mortality: an observational study,” International journal of nursing studies, Vol. 52, No. 2, pp. 535-542, 2015.
[17] E. Cho, N.-J. Lee, E.-Y. Kim, S. Kim, K. Lee, K.-O. Park, and Y. H. Sung, “Nurse staffing level and overtime associated with patient safety, quality of care, and care left undone in hospitals: a cross-sectional study,” International journal of nursing studies, Vol. 60, pp. 263-271, 2016.
[18] J.-Y. Lee, Y. A. Song, J. Y. Jung, H. J. Kim, B. R. Kim, H.-K. Do, and J.-Y. Lim, “Nurses’ needs for care robots in integrated nursing care services,” Journal of advanced nursing, Vol. 74, No. 9, pp. 2094-2105, 2018.
[19] Y. A. Song, H. J. Lee, and H. J. Kim, “간호, 로봇, 과학기술혁명: 간호업무지원을위한로봇 시스템 (nursing, robots, and the scientific-technological revolution: Robot systems to support nursing tasks),” 노인간호학회지 (Journal of Korean Gerontological Nursing), Vol. 20, No. S1, pp. 144-153, 2018. In Korean.
[20] 병원간호사회(Korean Hospital Nurses Association), 병원간호인력배치현황실태조사(Hospital Nursing Staff Allocation Status Survey). Seoul: 병원간호사회 (Korean Hospital Nurses Association),2022. In Korean.
[21] J. Ko, T. Kim, S. Park, and Y. Yang, “제7차 근로환경조사 최종보고서 (7th Working Environment Survey Final Report),” tech. rep., 산업안전보건연구원 (Korea Occupational Safety and Health Research Institute, KOSHA), Ulsan, South Korea, November 2023. 연구과제번호 2023-산업안전보건연구원-734.
[22] OECD, “What do we know about young people’s interest in health careers?”, tech. rep., OECD Publishing, Paris, 2025.
[23] 보건복지부 (Ministry of Health and Welfare ), 보건의료인력실태조사 (Healthcare Workforce Survey). Sejong: 보건복지부(Ministry of Health and Welfare), 2023. In Korean.
[24] K. A. Cho and Y. H. Seo, “Dual mediating effects of anxiety to use and acceptance attitude of artificial intelligence technology on the relationship between nursing students’ perception of and intention to use them: A descriptive study,” BMC Nursing, Vol. 23, p. 186, 2024.
[25] C. SunHwa and L. InSook, “Qualitative research on nurses experiencing taeoom,” Korean Journal of Occupational Health Nursing, Vol. 25, No. 3, pp. 238-248, 2016.
[26] S.-K. Jeong, “Concept analysis of taeum in nurses,” Journal of the Korea Academia-Industrial cooperation Society, Vol. 19, No. 8, pp. 482-491, 2018.
[27] A. Fabris, N. Baranowska, M. J. Dennis, D. Graus, P. Hacker, J. Saldivar, F. Zuiderveen Borgesius, and A. J. Biega, “Fairness and bias in algorithmic hiring: A multidisciplinary survey,” ACM Transactions on Intelligent Systems and Technology, Vol. 16, No. 1, pp. 1-54, 2025.
[28] D. Acemoglu and P. Restrepo, “Robots and jobs: Evidence from us labor markets,” Journal of political economy, Vol. 128, No. 6, pp. 2188-2244, 2020.

